1631
Zero Echo Time Arterial Spinning Labeling Magnetic Resonance Angiography in the diagnosis of intracranial artery stenosis: a feasibility study1Liaocheng People's Hospital, Liaocheng, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
This study aimed to investigate if zero-echo-time arterial-spin-labeling (ZTE ASL) MRA is feasible in the diagnosis of intracranial artery stenosis(ICAD). 25 patients with confirmed clinically stroke or transient ischemic attacks were recruited. For these patients, the correspondingly acquired ZTE-MRA images were compared with those using TOF-MRA technique. DSA imaging was also applied for and considered as a reference standard. For large-medium-sized intracranial arterial segments, ZTE-MRA showed better performance in the image quality and diseased artery detection than TOF-MRA. Therefore, ZTE-MRA can be considered as a promising technique to be further applied in the clinic routinely for patients with ICAD.
Introduction
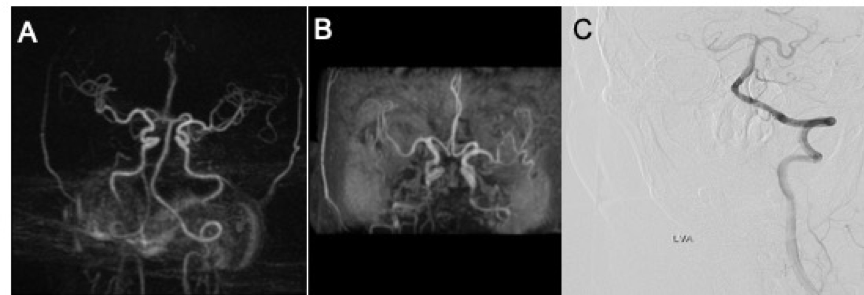
Stenosis is the most common abnormity occurred in intracranial arteries1and affects nearly 33%~50% of strokes and more than 50% of transient ischemic attacks (TIA) in Chinese population2. Accurate assessment and timely follow-up of intracranial artery stenosis (ICAD) can help to make a clinical treatment plan and estimate the prognosis3,4. Digital subtraction angiography(DSA) is considered the reference standard for evaluating the degree of ICAD,although the invasiveness as well as radiation risk limit its application. Zero-echo-time arterial-spin-labeling(ZTE ASL) MRA, has been reported to provide robust performance in blood vessel contrast and uniformity on carotid imaging5. We therefore, assume that this technique might also have potential in the diagnosis of ICAD. To investigate this, we applied ZTE-MRA technique in 25 patients with TIA or stroke. Time of flight (TOF) MRA images were also acquired for comparision. DSA imaging was also applied and served as a reference.Materials and Methods
SubjectsTwenty-five patients (11 male vs 14 female; mean age: 60.8±7.4 years old) were recruited due to TIA or stroke. All patients first underwent TOF-MRA, and were separately performed with ZTE-MRA and DSA within two days and four days afterwards. Written informed consent was obtained from each of them.
MR Experiments
All MRI experiments were performed on a 3T MR system (Discovery 750w, GE Healthcare, USA) along with a 24-channel head and neck joint coil. TOF-MRA sequence was applied with the scan parameters of field-of-view (FOV) = 240x211mm, matrix size=384x256, time of repetition (TR)=23ms, time of echo(TE)=3.0ms, number of slices=256and slice thickness=1.4mm. The acquisition time was 4 minutes 23s.
For ZTE-MRA measurement, the scan parameters included FOV =200 x 200mm, matrix size=166 x 166, (TR)=1116.4ms, number of slices=320and slice thickness=1.2mm. The scan time was 5 minutes 48s.
Data analysis
All acquired ZTE- and TOF-MRA images were reconstructed at GE MR workstation (AW 4.6, GE Medical Systems, USA).
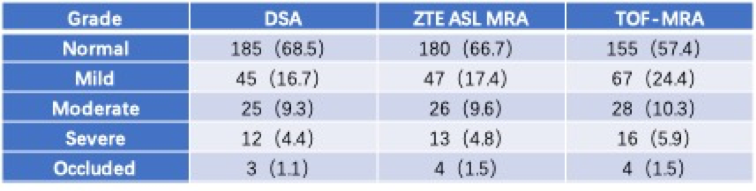
Intracranial artery was classified 26 segments and then divided into large-medium-sized and small-sized groups. Only large-medium-sized arterial segments (Supraclinoid ICA, infraclinoid ICA, A1, M1, P1, BA) due to clinical significance were measured the degree of stenosis. Image quality and ICAD assessment were performed by two blinded and independent readers. Disagreement was resolved by an unblinded consensus readings session. The North American Symptomatic Carotid Endarterectomy Trial(NASCET) criteria were used for stenosis calculations. Vascular stenosis was graded using 5-point grading scale as follows: normal (0~9%), mild (10~29%), moderate (30~69%), severe (70~99%), or occluded (no flow detected). Diseased vessels were defined as those whose NASCET stenosis rates fell into the moderate, severe, or occluded categories.
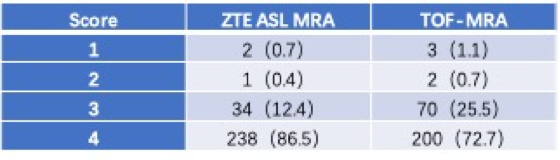
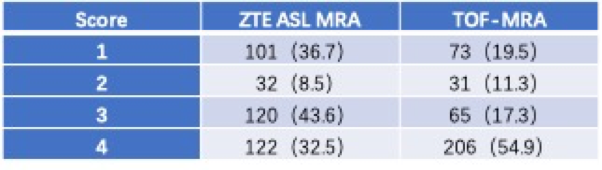
Four-point Likert scale was used for subjective image quality evaluation in the aspect of signal loss: scores 1 (severe signal loss, preventing image evaluation); 2 (moderate signal loss, compromising image assessment); 3 (minimal signal loss); 4 (no signal loss).
The statistical analysis was performed in SPSS 25.0 (IBM, Chicago, IL). Kappa-statistics statistics were firstly used to assess inter-observer agreement regarding the image quality and stenosis evaluation. The Mann–Whitney Uanalysis was used to assess the image quality between ZTE- and TOF-MRA by analyzing the signal loss. Sensitivity and specificity of ZTE- and TOF-MRA for diseased vessels were compared using the McNemar-test. Significance threshold was set as P<0.01.
Results
Good inter-observer agreements were separately shown in the assessment of image quality (κ=0.668 vs 0.625) and arterial stenosis(κ=0.660 vs 0.653) for both ZTE- and TOF-MRA images.Ensured with reliable image analysis, ZTE-MRA showed higher image quality than TOF-MRA for large-medium-sized arterial segments(3.85 [95%CI: 3.80 to 3.90] vs (3.70 [95% CI: 3.63 to 3.76]; p<0.01, Table 1), while an opposite pattern was observed in small-sized arteries(3.08 [95%CI: 2.96 to 3.20] vs 2.90 [95% CI: 2.79 to 3.02]; p<0.01, Table 2).
The frequency of the different stenosis severity grades based on DSA, ZTE-MRA and TOF-MRA are shown in Table3. For diseased artery detection, higher sensitivity and specificity were found for ZTE-MRA (97.5% and 98.3%) than for TOF-MRA(95.0% and 96.1%), indicating that ZTE-MRA has more accurate stenosis detection than TOF-MRA (P<0.01).
Discussion and Conclusion
In this study, we investigated the feasibility of ZTE-MRA in the diagnosis of ICAD. Although less qualified images in small-sized arterial segments were found in ZTE- than TOF-MRA, significantly higher image quality for large-medium-sized arterial segments has been found in ZTE-MRA images compared to TOF-MRA. Moreover, ZTE-MRA showed better performance than TOF-MRA in the detection of the diseased large-medium-sized artery segments which is the most important cause of stroke and TIA.In conclusion, due to superior performance in large-medium-sized segments, ZTE-MRA can be suggested as a routine method applied for patients with ICAD in the clinic.
Acknowledgements
This work is supported by National Natural Science Foundation of China(No. 61976110).
References
1. Wang Y, Zhao X, Liu L, et al. Prevalence and outcomes of symptomatic intracranial large artery stenoses and occlusions in China: The Chinese intracranial atherosclerosis (CICAS) study. Stroke 2014;45:663–9.
2. Wong LKS. Global burden of intracranial atherosclerosis. Int J Stroke 2006;1:158–9.
3. Wang T, Wang X, Yang K, et al. Endovascular treatment for symptomatic intracranial artery stenosis: Protocol for a systematic review and network meta-analysis. BMJ Open 2018;8.
4. Cai B, Peng B. Intracranial artery stenosis: Current status of evaluation and treatment in China. Chronic Dis Transl Med 2017;3:197–206.
5. Fujiwara Y, Muranaka Y. Improvement in visualization of carotid artery uniformity using silent magnetic resonance angiography. Radiol Phys Technol 2017;10:113–20.
Figures