1629
Investigation of the relationship between anatomical morphology of circle of Willis and the primary collateral blood flow based on t-ASL1Fujian Medical University Union Hospital, Fuzhou, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
We used 3D-TOF-MRA and territorial-ASL (t-ASL) maps to investigate the relationship between anatomical morphology of circle of Willis (CoW) and the primary collateral blood flow in physiological conditions. We found that the primary collateral blood flow had a direct relationship with anatomical structure of CoW. A1 segment has a role in controlling the blood flow in anterior circulation, while in posterior circulation, P1 segment and PcomA cooperate to dominate the blood flow.
Introduction
Primary collateral circulation through the circle of Willis (CoW) plays an important role in the regulation of cerebral blood flow, previous studies1-3 have reported that territorial ASL (t-ASL) is in good agreement with MRA and DSA. However, no studies have shown the relationship between the anatomical structure of CoW and primary collateral circulation. Our research aims to investigate the relationship between anatomical morphology of CoW and the primary collateral blood flow based on t-ASL.Methods
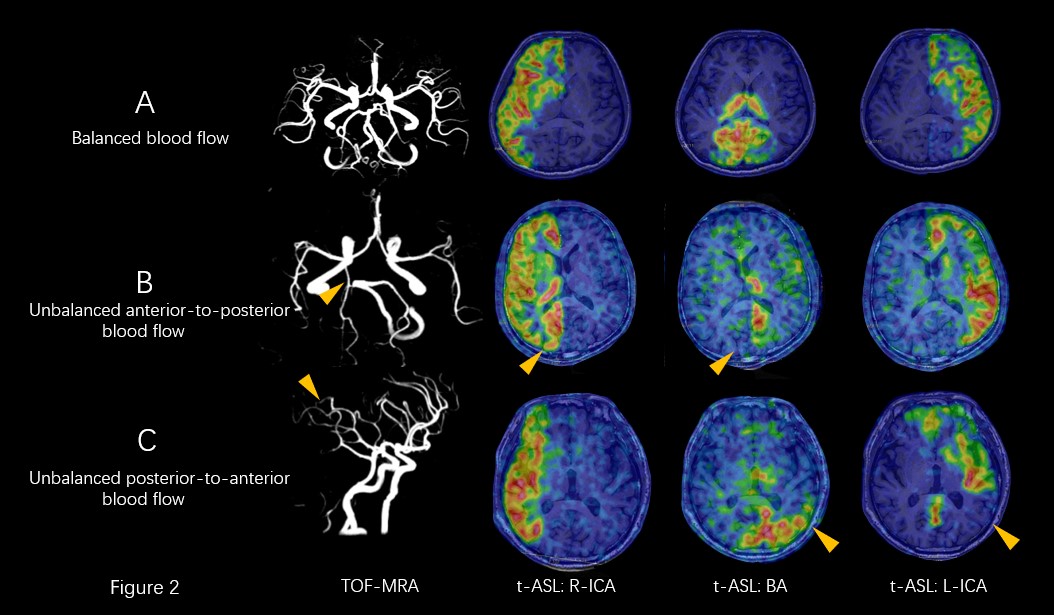
One hundred and nine healthy subjects underwent conventional MR imaging, 3D-TOF-MRA and t-ASL acquisition on a 3T MRI scanner (Discovery 750w, GE Healthcare, Wilwaukee, WI). According to the t-ASL results, the anterior circulation can be classified into three types, including balanced blood flow, unbalanced left-to-right blood flow and unbalanced right-to-left blood flow (Figure 1). The posterior circulation can also be classified into three types for each side, including balanced blood flow, unbalanced anterior-to-posterior blood flow, and unbalanced posterior-to-anterior blood flow (Figure 2). The diameters (in cm) of anterior communicating artery (AcomA), A1 segment in three t-ASL anterior circulation groups, posterior communicating artery (PcomA), and P1 segment in three t-ASL posterior circulation groups were measured using AW4.6 GE Workstation. Statistical analyses were performed using SPSS 20.0 software. The paired t-test was used to assess the diameter difference between bilateral A1 segments in each anterior circulation group, and the diameter difference between PcomA and P1 segment in each posterior circulation group. One-way ANOVA test was used to assess the difference A1right-A1left and AcomA across three anterior circulation groups, and the difference in P1-PcomA across three posterior circulation groups. The p value of less than 0.05 was considered to be significantly different.Results
In a total of 109 cases of t-ASL anterior circulation, there was no significant difference found between bilateral A1 segments in balanced blood flow group, while the diameter of the dominant side A1 was significantly larger than that of contralateral side in unbalanced blood flow groups (0.24±0.04, 0.15±0.04, P<0.001). A1right-A1left were significantly different across three anterior circulation groups (0.01±0.02, -0.09±0.06, 0.13±0.08, P<0.001), while AcomA showed no significant difference across three groups (0.11±0.03, 0.13±0.02, 0.11±0.04, P=0.222). In a total of 108 sides/54 cases of t-ASL posterior circulation, in balanced blood flow group, PcomA was always absent, and the diameters of P1 segment and PcomA were significantly different (0.20±0.03, 0.01±0.02, P<0.001). In anterior-to-posterior blood flow group, PcomA was always present, and the blood flow increased as the diameter of PcomA increased. The diameter of P1 segment and PcomA were significantly different (0.12±0.08, 0.17±0.05, P=0.004). In posterior-to-anterior blood flow group, the morphology of CoW lacks ipsilateral PcomA in unbalanced side, and the unbalanced blood flow was supplied to the middle cerebral artery territory via posterior cerebral artery (PCA) terminal branches. In addition, P1-PcomA were significantly different across three posterior circulation groups (0.19±0.04, -0.05±0.10. 0.19±0.14, P<0.001)Discussion
CoW is the primary collateral circulation pathway in brain, and plays the first role in the changes of cerebral hemodynamics. Previous studies have reported more than one criterion for diagnosis of vascular hypoplasia: the vessel diameter is smaller than 0.8 mm, 1.0 mm or half less than the normal lateral4-6. In anterior circulation, we found that unbalanced blood flow occurs when the diameter of bilateral A1 segments differs by 0.35 mm, even though there is no hypoplasia. Our results showed that the most important factor affecting anterior circulation blood flow was A1 segment, but not the AcomA. In the posterior circulation, P1 segment and PcomA cooperated to control blood flow. We speculated that the difference in blood flow between AcomA and PcomA was due to the blood pressure gradient. Usually blood pressure of bilateral internal carotid arteries (ICA) is almost equal, and the AcomA is closed. Only when the diameters of bilateral A1 segments are greatly different, resulting in an unequal blood pressure of bilateral anterior cerebral arteries (ACA), the blood will flow from the dominate side to the opposite, at which time AcomA is open. On the other hand, the blood pressure of ICA is higher than that of basiler artery in most situations, thus PcomA exists in a state of open. Overall, t-ASL can reflect unbalanced blood flow of primary collateral without contrast agent and ionizing radiation, and the long-term existence of this unbalanced blood flow status may cause some pathological changes afterwards.Conclusion
Anatomical morphology of CoW has important influence on primary collateral blood flow. A1 segment plays the most vital role in anterior circulation blood flow, while AcomA has no obvious effect. Different from AcomA, PcomA governs posterior circulation blood flow with P1 segment together.Acknowledgements
/References
1. Wu B, Wang X, Guo J, et al. Collateral circulation imaging: MR perfusion territory arterial spin-labing at 3T. AINR Am J Neuroradiol. 2008,29(10):1885-60.
2. Chng SM, Petersen ET, Zimine I, et al. Territorial arterial spin labeling in the assessment of collateral circulation comparison with digital subtraction angiography. Stroke. 2008,39 (12):3248-54.
3. Hartkamp NS, Petersen ET, Chappell MA, et al. Relationship between haemodynamic impairment and collateral blood flow in carotid artery disease. J Cereb Blood Metab. 2018,38(11):2021-2032.
4. Krabbe-Hartkamp MJ, van der Grind J, de Leeuw FE, et al. Circle of Willis: morphologic variation on three-dimensional time-of-flight MR angiograms. Radiology. 1998,207(1):103-11.
5. Klimek-Piotrowska W, Rybicka M, Wojnarska A, et al. A multitude of variations in the configuration of the circle of Willis: an autopsy study. Anat Sci Int. 2016,91(4):325-33.
6. Qiu C, Zhang Y, Xue C, et al. MRA study on variation of the circle of willis in healthy Chinese male adults. Biomed Res Int. 2015,976340.
Figures
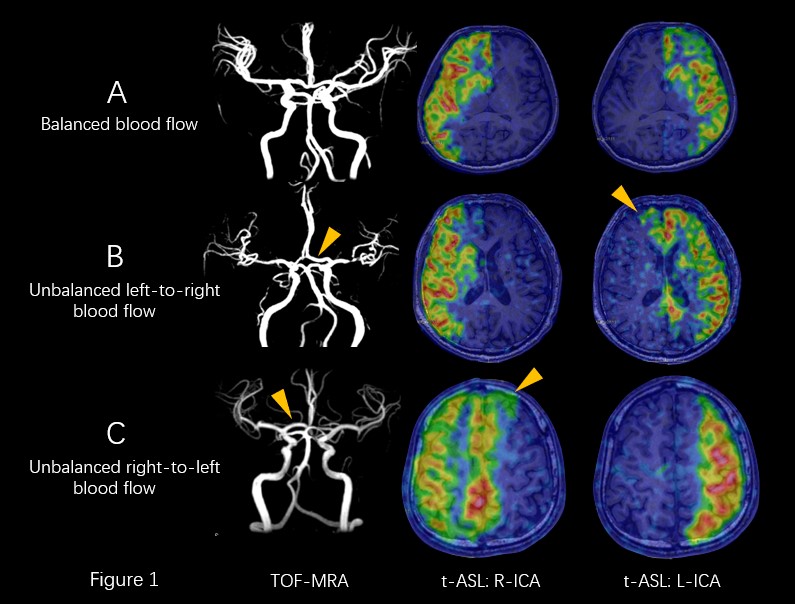
A: Balanced blood flow type; B and C: Unbalanced blood flow type. A: Case example of a 50-year-old woman, MRA shows diameters of bilateral A1 segments are approximately equal, t-ASL maps are balanced blood flow type. B: Case example of a 36-year-old man, MRA shows the diameter of left A1 is much larger than right, t-ASL maps are left-to-right unbalanced blood flow type. C: Case example of a 45-year-old man, MRA shows the diameter of right A1 is much larger than left, t-ASL maps are right-to-left unbalanced blood flow type.