1625
The relationship between cerebral arterial perforator function on 7 Tesla MRI and carotid occlusive disease
Tine Arts1, Laurien Onkenhout2, Doeschka Ferro2, Eline Oudeman2, Jaap Kappelle2, Thijs van Osch3, Jaco Zwanenburg1, Jeroen Hendrikse1, and Geert Jan Biessels2
1Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 2Neurology, University Medical Center Utrecht, Utrecht, Netherlands, 3Radiology, Leiden University Medical Center, Leiden, Netherlands
1Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 2Neurology, University Medical Center Utrecht, Utrecht, Netherlands, 3Radiology, Leiden University Medical Center, Leiden, Netherlands
Synopsis
Recently, flow velocity and pulsatility can be measured in cerebral perforating arteries. However, whether this perforator function is independent of upstream large vessel function is unknown. This study therefore investigates cerebral perforator velocity and pulsatility in the centrum semi-ovale (CSO) and basal ganglia (BG) using 7 Tesla MRI in patients with carotid occlusive disease and controls, and in patients inter-hemispherical. Cerebral perforator function was found to be similar in patients and controls, and also similar between hemispheres of patients with unilateral COD. These results show that cerebral arterial perforator function is independent of upstream large vessel disease.
Introduction
Recently, it has become possible to measure flow velocity and pulsatility of the cerebral perforating arteries. However, it is unknown whether this cerebral arterial perforator function depends on upstream large vessel function. This is a relevant, because these measures show promise as biomarkers for small vessel disease, yet many patients with small vessel disease also have large vessel atherosclerosis. Therefore, this study aimed to investigate this relationship by measuring cerebral perforator function in the centrum semi-ovale (CSO) and the basal ganglia (BG) in patients with carotid occlusive disease (COD), an extreme form of large vessel function disruption. Results were compared with matched controls and between hemispheres in patients with unilateral COD.Methods
Image acquisitionPatients and controls (recruited as part of the Heart Brain Connection) underwent 2D-Qflow acquisitions on 7 Tesla MRI (Philips) aimed at small perforators in the CSO and the BG (Figure 1). Scan parameters were described before1,2; briefly: retrospectively gated acquisition, 0.3 mm in-plane resolution, and Venc=4 and 20 cm/s for the CSO and BG respectively, 3:30 min:s acquisition at 80bpm heart rate. Similarly, 2D-Qflow measurement at the first branch of both left and right middle cerebral arteries (MCA, M1) were acquired (0.5mm resolution, Venc=120 cm/s).
Image processing
2D white matter and infarct masks at the Qflow locations were derived from 3 Tesla MRI T1-weighted and FLAIR images. The ROI in the CSO was obtained by subtracting the infarct mask (dilated with a 3x3 kernel) from the white matter mask. CSO white matter within 80 pixels from the brain surface was excluded to prevent partial volume effects from sulci touching the imaging plane. The BG was delineated manually, excluding dilated infarcts. Small perforators in the CSO and BG were detected using previously published methods.1,2 For the CSO, perforators located in ghosting artefact regions were automatically excluded3 as well as perforators in the BG oriented non-perpendicularly to the scanning plane. Perforators and M1 function were quantified by the mean blood flow velocity (Vmean) and pulsatility index (PI).
Results
Table 1 shows the characteristics of the included 21 patients (18 unilateral, 3 bilateral) and 19 controls. Figure 2 shows the exclusion numbers with explanation. Mask size differences due to excluded infarct areas did not affect results.Cerebral perforator function was similar in patients with COD and controls (Table 2; CSO Vmean mean difference [95% CI]=-0.1 cm/s [-0.2-0.0]; p=0.053 and PI=-0.1 [-0.2-0.0]; p=0.2; BG Vmean mean difference=-0.3 cm/s [-0.9-0.3]; p=0.3 and PI=-0.0 [-0.2-0.4]; p=1.0). In patients with unilateral COD, cerebral perforator function was also similar in both hemispheres (Table 3; CSO Vmean mean difference=6.5 cm/s [-1.2-4.2];p=0.23 and PI=-0.1 [-2.4-14]; p=0.35; BG Vmean mean difference=-0.1 cm/s [-0.5-0.4]; p=0.81 and PI=0.1 [-0.1-0.2]; p=0.23).
Discussion
Cerebral arterial perforator blood flow velocity and pulsatility on 7 Tesla MRI are new non-invasive measures of small vessel function. The relationship between these measures and up- and downstream vascular function is largely unknown. Here we zoomed in on the relation with the carotid artery. Literature addressing cerebral arterial function in patients with COD mainly focused on the MCA and MCA territory perfusion, with large methodological variability. Collateral perfusion of patients with COD appears to be crucial for normal or decreased MCA dynamics or tissue perfusion. Rosenkranz et al. found normal MCA velocities between patients and controls and within patients, and a reduced PI in the ipsilateral hemisphere4. Other studies reported a lower MCA velocity.5–8 Studies assessing cerebral blood flow in the MCA territory found either normal or decreased CBF in both hemispheres, ipsilateral, or in the basal ganglia.9–12 We found borderline significance in MCA PI difference between hemispheres in unilateral COD patients consistent with literature. Between patients and controls no significant differences were found (although CSO perforator velocity tended to be lower patients). This suggests relative hemodynamic stability of our patients, and the need for more statistical power given the similarity between patients and controls.Observed perforator function in the CSO is in agreement with earlier studies, as well as the PI values in the BG.1,2 The velocities found in the BG are slightly lower. This can be due to the removal of non-perpendicular perforators, which are often larger vessels with higher velocities.1,2,13 The M1 velocity and PI values found in this study are lower compared to earlier studies using ultrasound Doppler8,14, which may reflect Doppler overestimations, which can be as much as 47%15.
Strengths of this study include the assessment of small perforator function at different intracranial levels. Also, the automatic removal of perforators located in ghosting artefacts in the CSO and of non-perpendicular perforators in the BG results in more accurate results in a limited amount of time.3 A limitation of this study is the considerable number of excluded subjects due to movement during the sensitive Qflow scan. Secondly, our patients are relatively hemodynamically stable which may mean they have fairly sufficient compensatory mechanisms to maintain normal blood flow, velocity and PI.
Conclusion
In this study cerebral arterial perforator function was not affected by severe carotid occlusive disease, neither relative to controls, nor when comparing the affected and unaffected hemisphere in patients.Acknowledgements
We acknowledge the support from the Netherlands CardioVascular Research Initiative: the Dutch Heart Foundation (CVON 2018-28 & 2012-06 Heart Brain Connection), Dutch Federation of University Medical Centres, the Netherlands Organisation for Health Research and Development and the Royal Netherlands Academy of Sciences. This work was supported by the SVDs@target program (supported by the European Union’s Horizon 2020 research and innovation programme under grant agreement 666881).References
1. Bouvy WH, Geurts LJ, Kuijf HJ, et al. Assessment of blood flow velocity and pulsatility in cerebral perforating arteries with 7-T quantitative flow MRI. NMR Biomed. 2016;29(9):1295-1304. doi:10.1002/nbm.3306 2. Geurts L, Biessels GJ, Luijten P, Zwanenburg J. Better and faster velocity pulsatility assessment in cerebral white matter perforating arteries with 7T quantitative flow MRI through improved slice profile, acquisition scheme, and postprocessing. Magn Reson Med. 2018;79(3):1473-1482. doi:10.1002/mrm.26821 3. Arts T, Siero J, Biessels GJ, Zwanenburg J. Method for vessel selection effects the outcome and reproducibility of velocity and pulsatility measures in cerebral penetrating arteries. In: Annual Meeting of the International Society of Magnetic Resonance. Montreal; 2019:#3264. 4. Rosenkranz K, Langer R, Felix R. Transcranial Doppler sonography: collateral pathways in internal carotid artery obstructions. Angiology. 1991;42(10):819-826. doi:10.1177/000331979104201007 5. Kelley R, Namon R, Juang S, Lee S, JY C. Transcranial Doppler ultrasonography of the middle cerebral artery in the hemodynamic assessment of internal carotid artery stenosis. Arch Neurol. 1990;47(9):960-964. doi:10.1001/archneur.1990.00530090030009 6. Norris JW, Krajewski A, Bornstein NM. The clinical role of the cerebral collateral circulation in carotid occlusion. J Vasc Surg. 1990;12(2):113-118. doi:10.1016/0741-5214(90)90098-U 7. Gibbs JM, Leenders KL, Wise RJS, Jones T. Evaluation of cerebral perfusion reserve in patients with carotid-artery occlusion. Lancet. 1984;323(8370):182-186. doi:10.1016/S0140-6736(84)92110-X 8. Schneider PA, Rossman ME, Bernstein EF, Torem S, Ringelstein, Bernd, Otis SM. Effect of Internal Carotid Artery Occlusion on Intracranial Hemodynamics. Stroke. 1988;19(5):589-593. 9. Cosottini M, Pingitore A, Michelassi MC, et al. Redistribution of cerebropetal blood flow in patients with carotid artery stenosis measured non-invasively with fast cine phase contrast MR angiography. Eur Radiol. 2005;15(1):34-40. doi:10.1007/s00330-004-2524-9 10. Hartkamp NS, Petersen ET, Chappell MA, et al. Relationship between haemodynamic impairment and collateral blood flow in carotid artery disease. J Cereb Blood Flow Metab. 2018;38(11):2021-2032. doi:10.1177/0271678X17724027 11. Hartkamp NS, Bokkers RPH, van Osch MJP, de Borst GJ, Hendrikse J. Cerebrovascular reactivity in the caudate nucleus, lentiform nucleus and thalamus in patients with carotid artery disease. J Neuroradiol. 2017;44(2):143-150. doi:10.1016/j.neurad.2016.07.003 12. Hendrikse J, van Osch MJP, Rutgers DR, et al. Internal carotid artery occlusion assessed at pulsed arterial spin-labeling perfusion MR imaging at multiple delay times. Radiology. 2004;233(3):899-904. doi:10.1148/radiol.2333031276 13. Geurts LJ, Luijten PR, Klijn CJM, Zwanenburg JJM, Biessels GJ. Higher Pulsatility in Cerebral Perforating Arteries in Patients With Small Vessel Disease Related Stroke, a 7T MRI Study. Stroke. 2018;50(1):62-68. doi:10.1161/strokeaha.118.022516 14. Hennerici M, Rautenberg W, Sitzer G, Schwartz A. Transcranial doppler ultrasound for the assessment of intracranial arterial flow velocity-Part 1. Examination technique and normal values. Surg Neurol. 1987;27(5):439-448. doi:10.1016/0090-3019(87)90251-5 15. Hoskins P. Accuracy of maximum velocity estimates made using Doppler ultrasound systems. Br J Radiol. 1996;69(818):172-177. doi:10.1259/0007-1285-69-818-172Figures
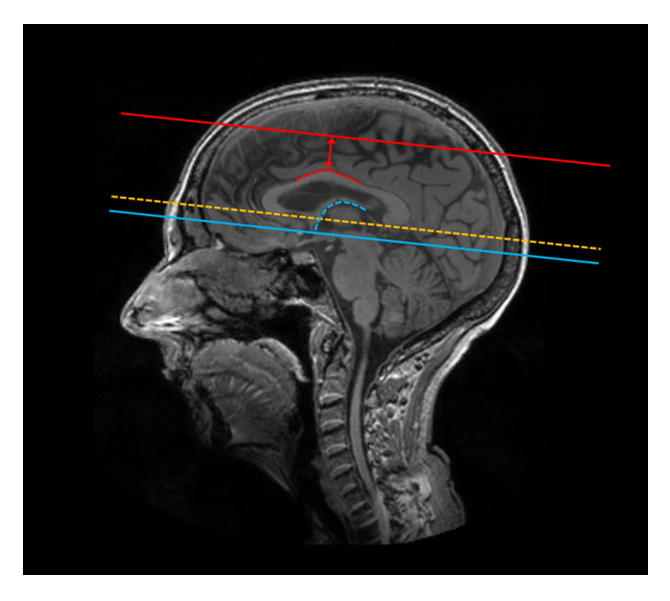
Figure 1: Planning of the CSO Qflow slice (red
solid line) and BG Qflow slice (blue
solid line). The dotted yellow line shows the orientation of the slices, i.e.
the bottom of the corpus collosum. The CSO slice (red solid line) is located
15mm above the top of the corpus collosum (red dotted line). The BG slice (blue
solid line) is planned at the bottom of the splenium (blue dotted line).
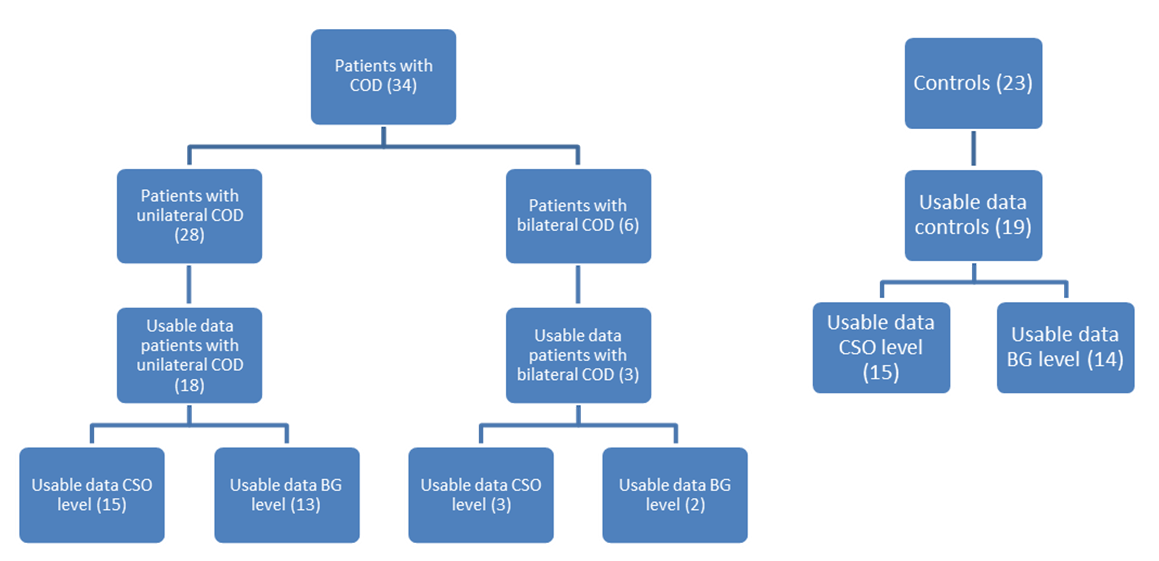
Figure 2: flow chart showing the number of excluded scans for
patients as well as controls
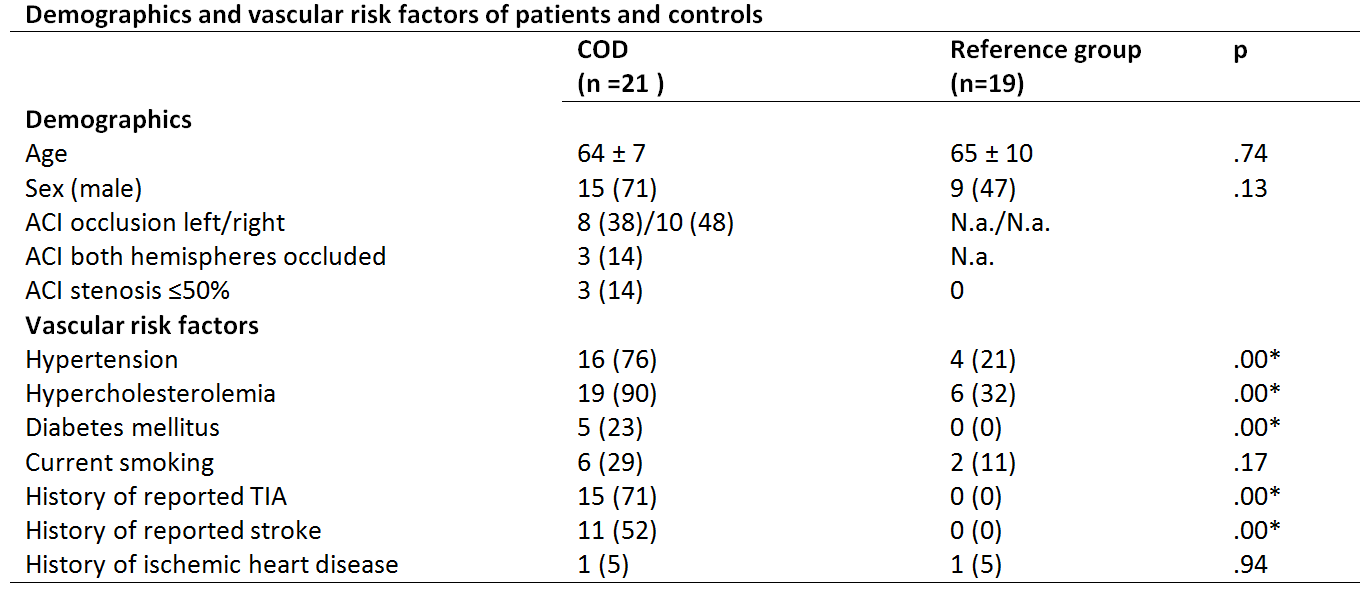
Table 1: ACI=internal carotid artery;
BG= basal ganglia; CSO= centrum semi-ovale; WB= whole brain. Data presented
as group mean ±SD, n (%) and median [range]. All comparisons between groups
were performed with T-test. * p ≤0.05 was considered significant.
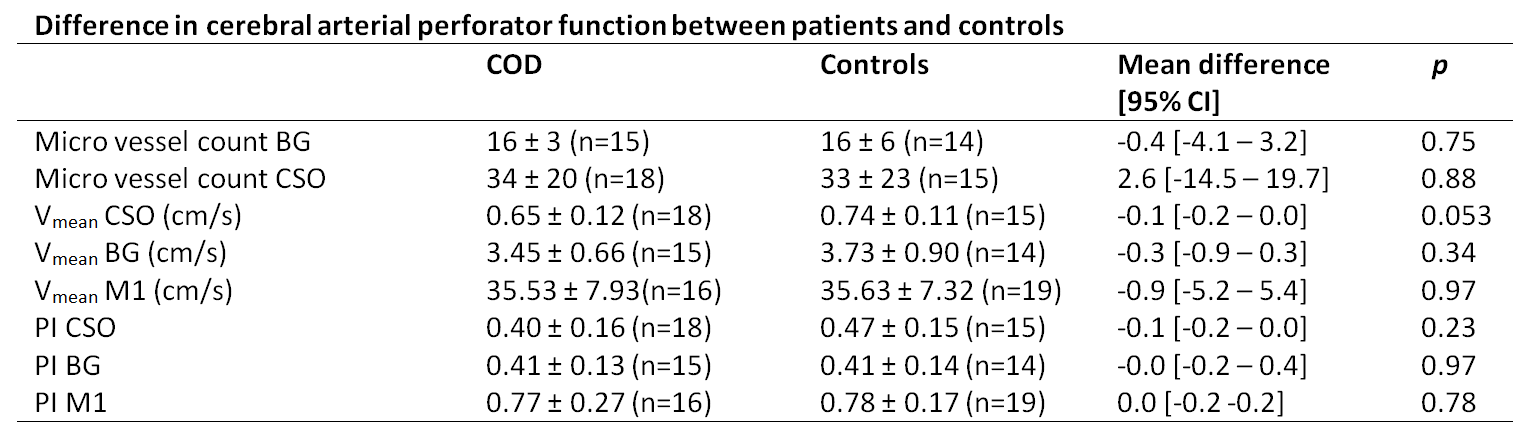
Table 2: Whole
brain results are shown for 21 patients with COD and 19 controls. ACI= internal
carotid artery; BG=basal ganglia; CSO= centrum semi-ovale; Vmean=
mean blood flow velocity; PI= pulsatility index; M1= first branch of middle
cerebral artery. For the M1, data of both hemispheres was averaged and only
included in this table if measures of both hemispheres were present. Data are
presented as group mean±SD. Statistical testing: independent samples t-test. *
p ≤0.05 was considered significant.

Table 3: Results
are shown for 18 patients with unilateral COD. ACI=internal carotid artery; BG=
basal ganglia; CSO= centrum semi-ovale; M1 = first branch of middle cerebral
artery; Vmean= mean blood flow velocity; PI= pulsatility index; Data
are presented as group mean ±SD. Statistical testing: paired samples t-test. *
p ≤0.05 was considered significant.