1623
Towards non-invasive estimation of "resting-state" CVR: associations with congenital heart disease, cognition, and nasal nitric oxide1Radiology, Children's Hospital of Pittsburgh of UPMC, Pittsburgh, PA, United States, 2University of Pittsburgh, Pittsburgh, PA, United States
Synopsis
Estimation of cerebrovascular reserve/reactivity (CVR) typically necessitates an invasive vasoactive stimulus. We here propose a metric to non-invasively estimate “resting-state” CVR (rCVR), the capacity of the vasculature to respond to resting-state metabolic demand, as the negative ratio of functional connectivity strength (FCS) to regional cerebral blood flow (CBF). Construct validity was demonstrated via prediction of end-tidal CO2 levels (PETCO2). rCVR was lower in older children with congenital heart disease (CHD) in default mode network (DMN), salience network (SN), and central executive network (CEN), and was positively associated with neurocognitive outcome (NIH Toolbox) and nasal nitric oxide (nNO) levels.
Inroduction
Cerebrovascular reserve/reactivity (CVR), the ability of the vasculature to respond to increased metabolic demand over baseline, is impaired in a variety of pathologies and associated with impaired cognitive function. However, estimation of CVR typically involves an invasive vasoactive challenge. We explore here a metric, the negative ratio of functional connectivity strength (FCS) to cerebral blood flow (CBF), which may be measured non-invasively, as a proxy for “resting-state” CVR (rCVR) – the ability of the vasculature to respond to resting-state metabolic demand, which is likely closely related to standard CVR.Materials and Methods
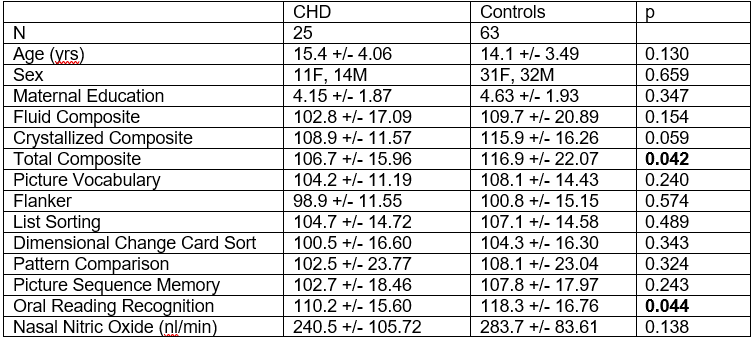
Resting-state BOLD and PCASL data were successfully acquired from 88 normal older children and children with congenital heart disease (CHD) on a Siemens 3T Skyra scanner (demographic/neuropsychological information in Figure 1). Previously published methods1 were used to volume censor the BOLD data in order to minimize spurious correlations from participant motion. After regressing out motion and drift parameters and band-pass filtering, FCS maps were constructed. FCS in a gray matter voxel is defined as the average correlation coefficient between it and all other gray matter voxels, with negative correlation coefficients set to zero. Gray matter voxels were determined by segmenting a T1-weighted anatomical image using routines in SPM8. After motion correction, CBF maps were computed from the raw PCASL images using the two-compartment model2 with literature parameter values3. rCVR maps were computed as the negative of the ratio of FCS to CBF (the ratio of CBF to FCS has been previously used; our ratio is selected due to noise considerations). A global gray matter mask was computed from all participants and voxels in the mask used for subsequent voxelwise analyses. For all participants, missing voxels were filled in using trilinear interpolation. Each participant also received the NIH Toolbox Cognitive Battery. Finally, a subset (44) of participants received nasal nitric oxide (nNO) measurements; nNO is a proxy for NO bioavailability.As a test for construct validity, the partial end-tidal CO2 (PETCO2) time course was estimated from the rCVR maps by demeaning and constructing the frequency-filtered weighted average of the BOLD resting-state signal. This was compared to a previously published method4 using the global BOLD signal; in the case of the null hypothesis that rCVR is not related to true CVR the correlation coefficient should be zero.
Voxelwise GLMs were performed with CHD status, NIH Toolbox Total composite score, and nNO the independent variables; sex, age covariates of no interest; and rCVR the dependent variable. Additionally, mediation analyses5 were performed with CHD status the independent variable, rCVR the mediator, and NIH Toolbox scores as the dependent variable. Bootstrapping (1000 repetitions) was used to test for statistical significance, using bias-corrected and accelerated confidence intervals6,7. Standard methods8 were used to correct for multiple comparisons across voxels via construction of noise maps; results were deemed significant at FDR-corrected q < 0.05.
Results
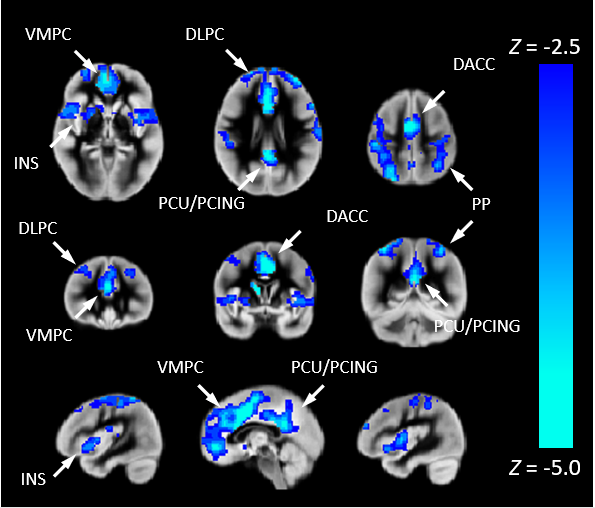
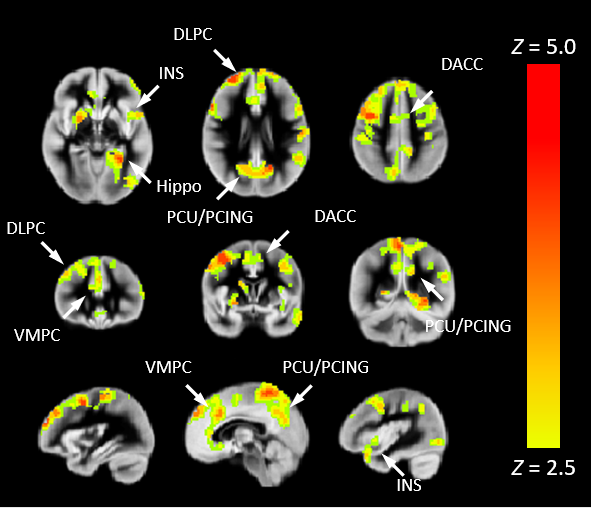
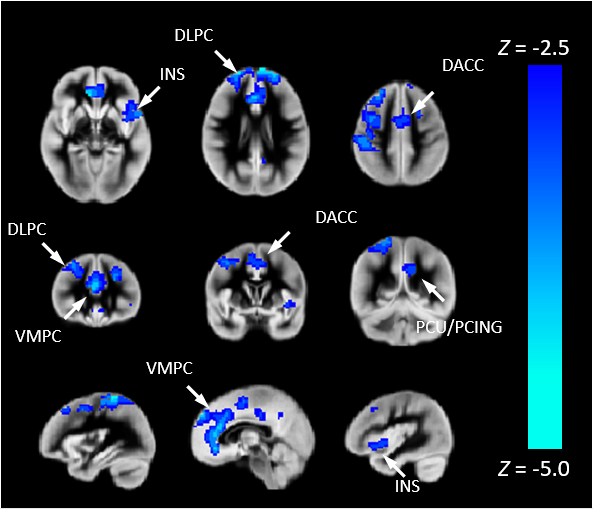
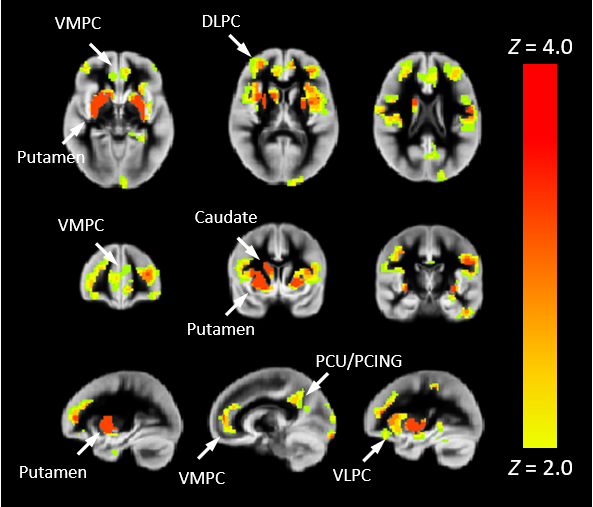
The average correlation coefficient between the PETCO2 time courses was 0.67 (p < 0.001), indicating a strong correspondence of rCVR to the true CVR.Individuals with CHD display lower rCVR (Figure 2) in regions comprising the default mode network (DMN): posterior cingulate/precuneus, medial prefrontal; salience network (SN): insula, anterior cingulate; and central executive network (CEN): dorsolateral prefrontal, posterior parietal. Regions in these three networks are also positively correlated with total composite cognition (Figure 3). The mediation analysis (Figure 4) also shows a negative indirect effect of rCVR on the relation between CHD status and cognition, indicating that reduced rCVR mediates worse neurocognitive outcome in CHD patients. Finally, rCVR is positively associated with nNO levels (Figure 5) in DMN and CEN regions as well as the putamen.
Discussion
Functional connectivity is highly correlated to baseline metabolism, with highly metabolically active regions forming a “rich club” of highly connected hubs9. Thus the ratio of CBF/FCS (or its negative reciprocal) may represent a “resting-state” CVR, e.g. how well the cerebral vasculature responds to baseline metabolic demand. In turn, the ability of the vasculature to respond to baseline demand may reflect its ability to respond to demand above baseline (CVR). Our strong correlations of the PETCO2 estimates provide strong support for this hypothesis, especially since the PETCO2 estimate in the previously published method4 only itself provided correlation of R = 0.6 with the true timecourse. However, future research comparing CVR estimated via vasoactive stimuli will be necessary.rCVR is also strongly correlated with neurocognitive outcome, indicating that the vasculature is important for optimal cognitive function in cognitively normal as well as impaired individuals. Of note, rCVR is lower in CHD patients, and our mediation analyses confirm that the risk for adverse neurocognitive outcome in CHD is at least partially underlain by reduced CVR. Finally, the positive associations between rCVR and nNO support a biochemical basis for rCVR due to NO bioavailability, perhaps due to differences in the endothelial NO synthase (eNOS) gene or its expression.
Conclusion
A metric for “resting-state” CVR is proposed involving the negative ratio of FCS to CBF. Our test for construct validity suggests a strong association with CVR. rCVR is positively associated with neurocognitive outcome and nNO levels; reduced rCVR is also shown to underlie the risk for adverse neurocognitive outcomes in CHD patients.Acknowledgements
No acknowledgement found.References
1. Power JD, Mitra A, Laumann TO, Snyder AZ, Schlaggar BL, Petersen SE. Methods to detect, characterize, and remove motion artifact in resting state fmri. NeuroImage. 2014;84:320-341.
2. Wang J, Alsop DC, Li L, Listerud J, Gonzalez-At JB, Schnall MD, Detre JA. Comparison of quantitative perfusion imaging using arterial spin labeling at 1.5 and 4.0 tesla. Magnetic resonance in medicine. 2002;48:242-254
3. Schmithorst VJ, Hernandez-Garcia L, Vannest J, Rajagopal A, Lee G, Holland SK. Optimized simultaneous asl and bold functional imaging of the whole brain. Journal of magnetic resonance imaging : JMRI. 2014;39:1104-1117
4. Liu P, Li Y, Pinho M, Park DC, Welch BG, Lu H. Cerebrovascular reactivity mapping without gas challenges. NeuroImage. 2017;146:320-326
5. Hayes AF, Scharkow M. The relative trustworthiness of inferential tests of the indirect effect in statistical mediation analysis: Does method really matter? Psychological Science. 2013;24:1918-1927
6. DiCiccio T, Efron B. Bootstrap confidence intervals. Statistical Science. 1996;11:189-228
7. Efron B. Better bootstrap confidence intervals. J Am Stat Assoc. 1987;89:171-185
8. Ledberg A, Akerman S, Roland PE. Estimation of the probabilities of 3d clusters in functional brain images. NeuroImage. 1998;8:113-128
9. Collin G, Sporns O, Mandl RC, van den Heuvel MP. Structural and functional aspects relating to cost and benefit of rich club organization in the human cerebral cortex. Cereb Cortex. 2014;24:2258-2267
Figures