1612
Non-Contrast Enhanced Ultrashort Echo Time MR Angiography (Silent MRA) for Intracranial Aneurysms Treated with Flow-Diverter Stents and Coils1Department of Radiology, Juntendo University Hospital, Tokyo, Japan, Tokyo, Japan, 2Department of Neurosurgery, Juntendo University School of Medicine, Tokyo, Japan, Tokyo, Japan, 3Department of Neuroendovascular Therapy, Juntendo University School of Medicine, Tokyo, Japan, Tokyo, Japan
Synopsis
We evaluated the usefulness of non-contrast enhanced ultrashort TE MRA (Silent MRA) for intracranial aneurysms treated with flow-diverter (FD) stents and coils. FD stent has a higher metal coverage, thus it is difficult to visualize in-stent flow using TOF-MRA, due to the magnetic susceptibility. In contrast, silent MRA uses ultrashort TE, therefore may visualize in-stent flow. In silent MRA, in-stent flow score was superior to that of TOF-MRA (p<0.05). Moreover, aneurysm occlusion status was in good agreement with X-ray DSA (κ = 0.84). Therefore, silent MRA is useful for the evaluation of intracranial aneurysms treated with FD stents and coils.
Background and Purpose
Follow-up of intracranial aneurysms treated with flow-diverter (FD) stent using three-dimensional time of flight MRA (3D TOF-MRA) is difficult due to the susceptibility artifacts produced by metallic devices and T1 shortening of thrombus in the aneurysm. The FD stent has about 30-35% surface metal coverage, while the metal coverage of previous reported intracranial stents has approximately 8-20% coverage.1 After the treatment of FD stent, aneurysm residual, recurrence due to recanalization, in-stent stenosis, stent occlusion, and stent migration should be evaluated.2,3 In recent years, Silent MRA has been introduced after intracranial stent placement.4-6 Silent MRA uses ultrashort echo time (UTE) combined with arterial spin labeling (ASL). In magnetic resonance imaging, short echo time can reduce the phase dispersion of the blood flow signal and decreases the magnetic susceptibility artifacts. There is one report that the usefulness of Silent MRA in intracranial aneurysms treated with FD stent.7 However, the evaluation of the depiction of residual flow after placement of FD stent and coil has not reported yet. The purpose of this study was to assess the usefulness of non-contrast enhanced MRA using UTE acquisition (Silent MRA) in intracranial aneurysms treated with FD stents and coils and compare it with 3D TOF-MRA.Methods
Fifteen aneurysms treated with FD stents and coils underwent silent MRA, 3D TOF-MRA, and X-ray digital subtraction angiography (DSA). The following scan parameters were used for Silent MRA: TR/TE, 642.8/0.016 ms; flip angle, 5°; FOV, 180 × 180 mm; matrix, 180 × 180; section thickness, 1.0 mm (with section interpolation); NEX, 1.4; bandwidth, 31.2 kHz; acquisition time, 12 minutes 13 seconds; and reconstructed voxel size, 1.0 × 1.0 × 0.5 mm. The 3D TOF-MRA scan parameters were as follows: TR/TE, 20/2.9 ms; flip angle, 18°; FOV, 200 × 200 mm; acquisition matrix, 416 × 224; section thickness, 1.0 mm (with section interpolation); NEX, 1; bandwidth,41.7 kHz; acquisition time, 4 minutes 45 seconds (3 slabs, overlap between a slab: 14 sections, 1 slab: 38 sections); reconstruction matrix, 512; and reconstructed voxel size, 0.39 × 0.39 × 0.5 mm. Two neuroradiologists independently reviewed the MRA images, and subjectively scored the flow in the stents on a scale of 1 (not visible) to 4 (excellent). Moreover, we evaluated the aneurysm occlusion status using a 2-grade scale (total occlusion / remnant [neck or aneurysm]). The most recent X-ray DSA images were used as a reference standard. The scores of MRA images from the 2 observers were averaged, and the scores were compared between techniques by using the Wilcoxon signed rank test. A p value < 0.05 was statistically significant. Weighted κ statistics were used to evaluate interobserver and intermodality agreement.Results
The average score ± standard deviation for silent MRA and 3D TOF-MRA were 3.59 ± 0.49 and 2.00 ± 0.87 (p < 0.05), respectively. Substantial interobserver agreement (κ = 0.66) was observed. The percentages of 2-grade scale were 34% and 66% for X-ray DSA, 31% and 69% for silent MRA, and 9% and 91% for 3D TOF-MRA, respectively. Intermodality agreement for X-ray DSA / Silent MRA and X-ray DSA / 3D TOF-MRA were 0.84 and 0.27, respectively.Discussion
Silent MRA uses an UTE combined with arterial spin labeling (ASL).4 ASL technique is used as a preparation pulse for visualization of the blood flow, and the data acquisition is based on 3D radial sampling.4,8 Our results demonstrated that silent MRA was able to depict in-stent flow and neck remnants despite the high metal coverage of FD stent. The use of UTE has minimized the phase dispersion of the signal of labeled blood flow and decreased the susceptibility artifacts to metallic devices. Therefore, silent MRA could show a better visualization compared to 3D TOF-MRA. In silent MRA, aneurysm occlusion status was in a good agreement with X-ray DSA. Thus,the silent MRA has a possibility to replace X-ray DSA for follow-up of intracranial aneurysms treated with intracranial stents such as FD stent.Conclusion
Non-contrast enhanced UTE MRA (Silent MRA) is useful for the follow-up of intracranial aneurysms treated with flow-diverter stents and coils.Acknowledgements
This work was supported by JSPS KAKENHI Grant Number JP16H06280. Grant-in-Aid for Scientific Research on Innovative Areas- Resource and technical support platforms for promoting research 'Advanced Bioimaging Support’.
References
1. Boddu SR, Tong FC, Dehkharghani S, et al. Contrast-enhanced time-resolved MRA for follow-up of intracranial aneurysms treated with the pipeline embolization device. AJNR Am J Neuroradiol 2014 Nov-Dec;35(11):2112-8.
2. Fiorella D, Albuquerque FC, Deshmukh VR, et al. Usefulness of the Neuroform stent for the treatment of cerebral aneurysms: results at initial (3–6-mo) follow-up. Neurosurgery 2005;56:1191–201, discussion 1201-02.
3. Siddiqui MA, Bhattacharya J, Lindsay KW, et al. Horizontal stentassisted coil embolisation of wide-necked intracranial aneurysms with the Enterprise stent: a case series with early angiographic follow-up. Neuroradiology 2009;51:411-18.
4. Irie R, Suzuki M, Yamamoto M, et al. Assessing Blood Flow in an Intracranial Stent:A Feasibility Study of MR Angiography Using a Silent Scan after Stent-Assisted Coil Embolization for Anterior Circulation Aneurysms. AJNR Am J Neuroradiol 2015 May;36:967-70.
5. Takano N, Suzuki M, Irie R, et al. Usefulness of Non–Contrast-Enhanced Magnetic Resonance Angiography Using a Silent Scan for Follow-Up after Y-Configuration Stent-Assisted Coil Embolization for Basilar Tip Aneurysms. AJNR Am J Neuroradiol 2017;38 (3):577–81
6. Takano N, Suzuki M, Irie R, et al. Non-Contrast-Enhanced Silent Scan MR Angiography of Intracranial Anterior Circulation Aneurysms Treated with a Low-Profile Visualized Intraluminal Support Device. AJNR Am J Neuroradiol 2017;38 (8):1610–16
7. Oishi H, Fujii T, Suzuki M, et al. Usefulness of Silent MR Angiography for Intracranial Aneurysms Treated with a Flow-Diverter Device. AJNR Am J Neuroradiol 2019;40(5):808-814.
8. Alibek S, Vogel M, Sun W, et al. Acoustic noise reduction in MRI using Silent Scan: an initial experience. Diagn Interv Radiol 2014;20:360-3
Figures
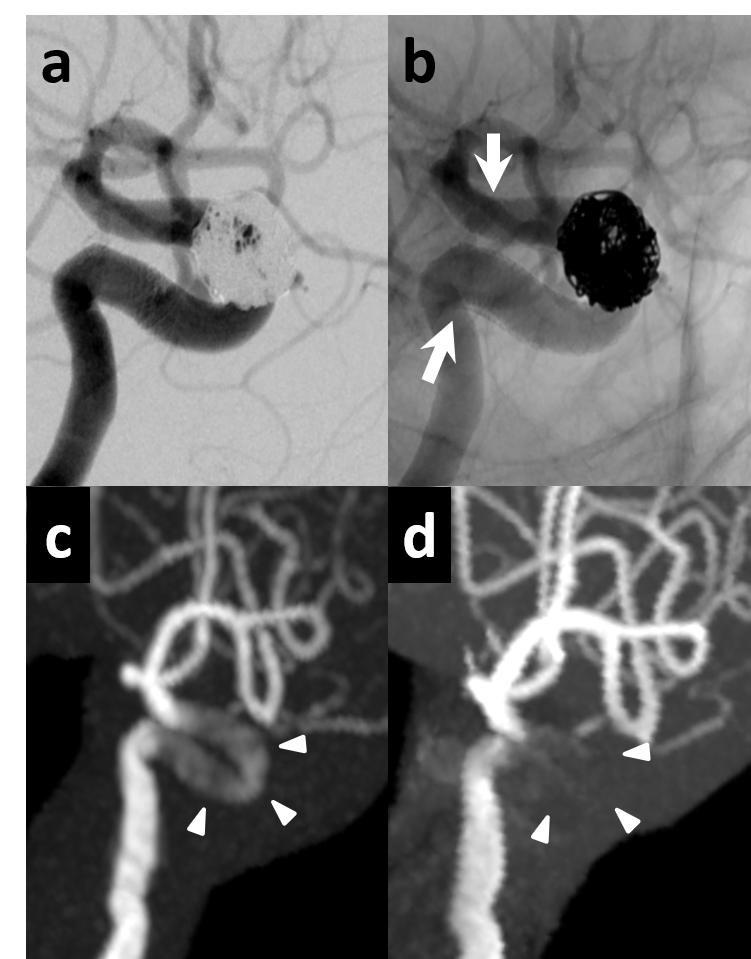
Fig.1
75 y.o Female (Right ICA : 4.75 × 35)
a.Digital subtraction angiography immediately after flow-diverter stent deployment is successful.
b.Non-subtraction angiography (White arrows are stent edge.)
c.Silent MRA with 1day interval demonstrates minimal signal loss of stented segment (white arrow heads).
d.3D TOF-MRA on same day shows complete signal loss at C2-C4 segment (white arrow heads).
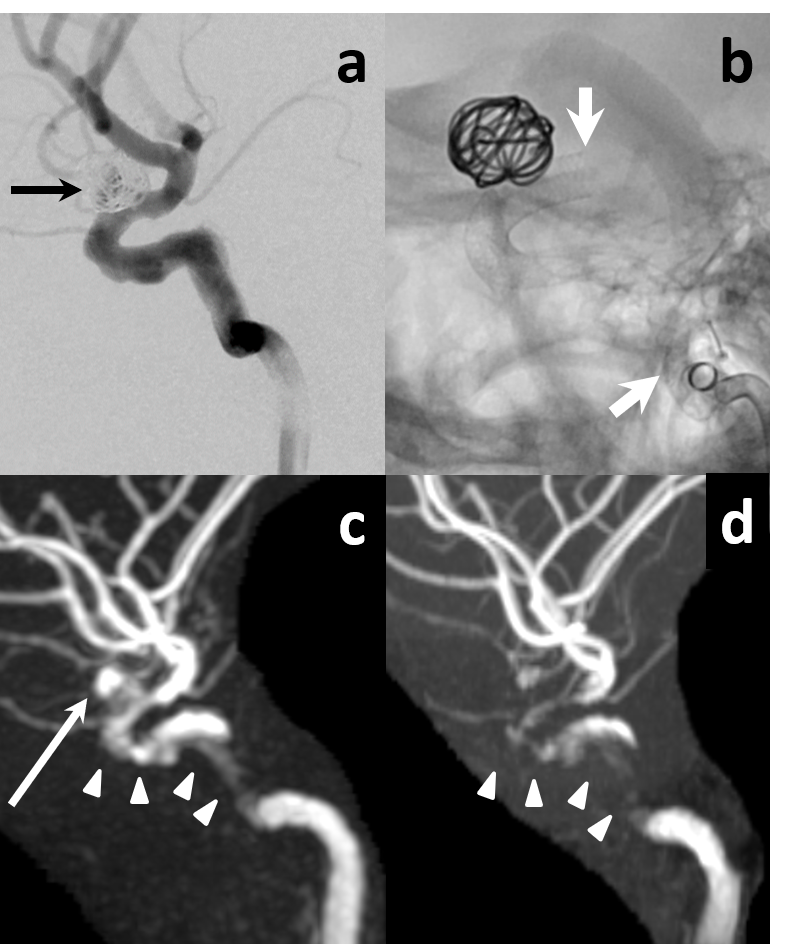
Fig.2
21 y.o Female (Left ICA : 3.0 × 18 and 5.0 × 16)
a.Digital subtraction angiography immediately after flow-diverter stents deployment is successful. Aneurysm remnant is depicted (black arrow).
b.Non-subtraction angiography (White arrows are stent edge.)
c.Silent MRA with 1day interval demonstrates minimal signal loss of stented segment (white arrow heads). Aneurysm remnant is depicted (long arrow).
d.3D TOF-MRA on same day shows almost signal loss at stented segment (white arrow heads).
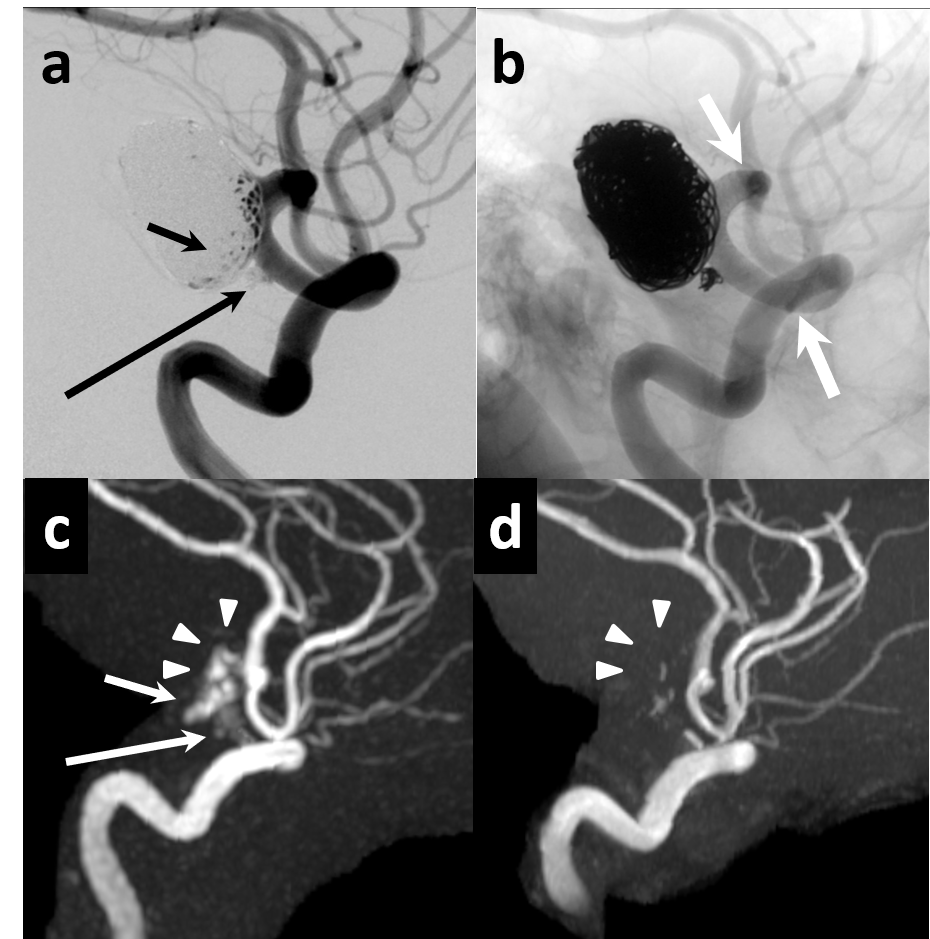
Fig.3
65 y.o Male (Right ICA : 3.75 × 25 and 3.75 × 16)
a.Digital subtraction angiography immediately after flow-diverter stents deployment is successful. Aneurysm remnant (short arrow) and neck remnant are depicted (long arrow).
b.Non-subtraction angiography (White arrows are stent edge.)
c.Silent MRA with 1day interval demonstrates minimal signal loss of stented segment (white arrow heads). Aneurysm and neck remnants are depicted (long arrows) like a DSA.
d.3D TOF-MRA on same day shows complete signal loss at stented segment (white arrow heads). Remnants are not depicted.