1610
Noninvasive assessment of revascularization in adult-onset moyamoya disease after bypass surgery using super-selective ASL perfusion1Department of Radiology, Seoul National University Hospital, Seoul, Korea, Republic of, 2Department of Neurosurgery, Seoul National University Hospital, Seoul, Korea, Republic of
Synopsis
The purpose of this study was to evaluate whether super-selective ASL (SS-ASL) perfusion imaging could precisely visualize the revascularization area after bypass surgery in moyamoya disease, compared to digital subtracted angiography (DSA). Twenty-eight bypassed hemispheres of twenty-six patients in moyamoya disease underwent postoperative six months SS-ASL and DSA. Subjective image analysis of the revascularization area, as well as collateral grading, were performed. The agreement of the revascularization area was excellent (weighted kappa, 0.83), and agreement of collateral grading was good (weighted kappa, 0.722.) SS-ASL could evaluate revascularization territory precisely in the patient of moyamoya disease who underwent bypass surgery.
INTRODUCTION
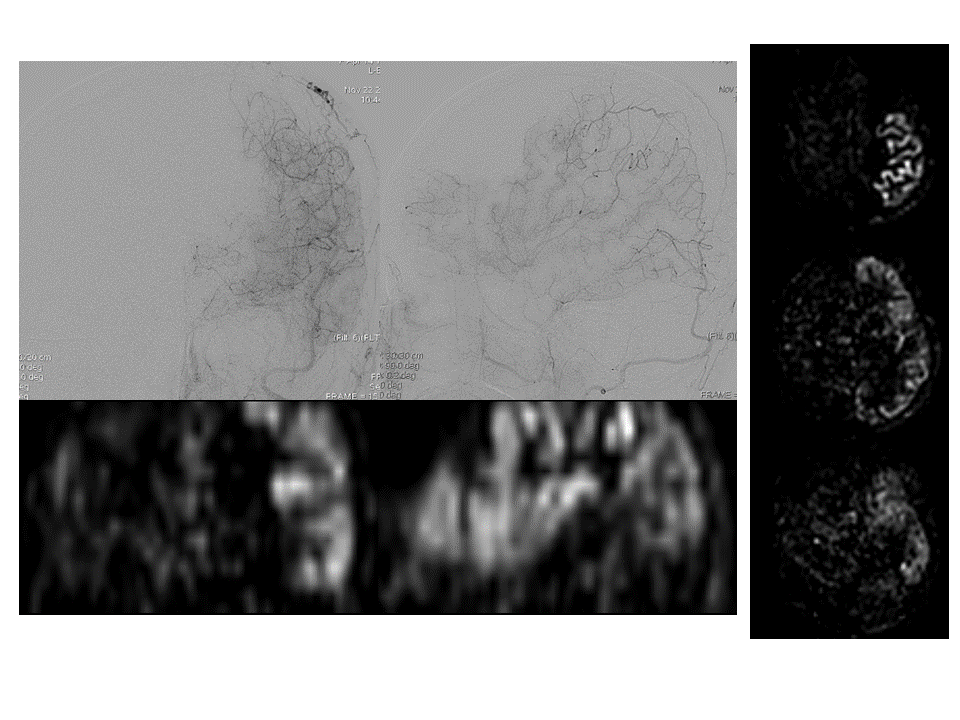
Moyamoya disease is a chronic occlusive cerebrovascular disease characterized by progressive stenosis of the terminal portion of the internal carotid artery and the formation of an abnormal vascular network at the base of the brain.1 The only effective treatment to prevent cerebral ischemia is surgical revascularization. After surgical revascularization, the patient has to be monitored to assess the patency of bypass and changes of perfusion. Conventional digital subtracted angiography (DSA) is still regarded as a gold standard modality to evaluate bypass; however, it is an invasive procedure and may have the potential of complication. Super-selective arterial spin labeling (SS-ASL) technique can provide regional perfusion imaging of each vessel, which gives information about actual areas of the cerebral perfusion territory of individual arteries.2 It can be used to monitor the bypass patency and to assess of revascularization area in moyamoya disease. Therefore, the purpose of the present study was to evaluate whether SS-ASL perfusion imaging could precisely visualize the revascularization area after combined direct and indirect bypass surgery in adult moyamoya disease, compared to DSA. Besides, we explored the change of perfusion territories of collateral supplies at the bypass side by using SS-ASL perfusion and compared with the finding of DSA.METHODS
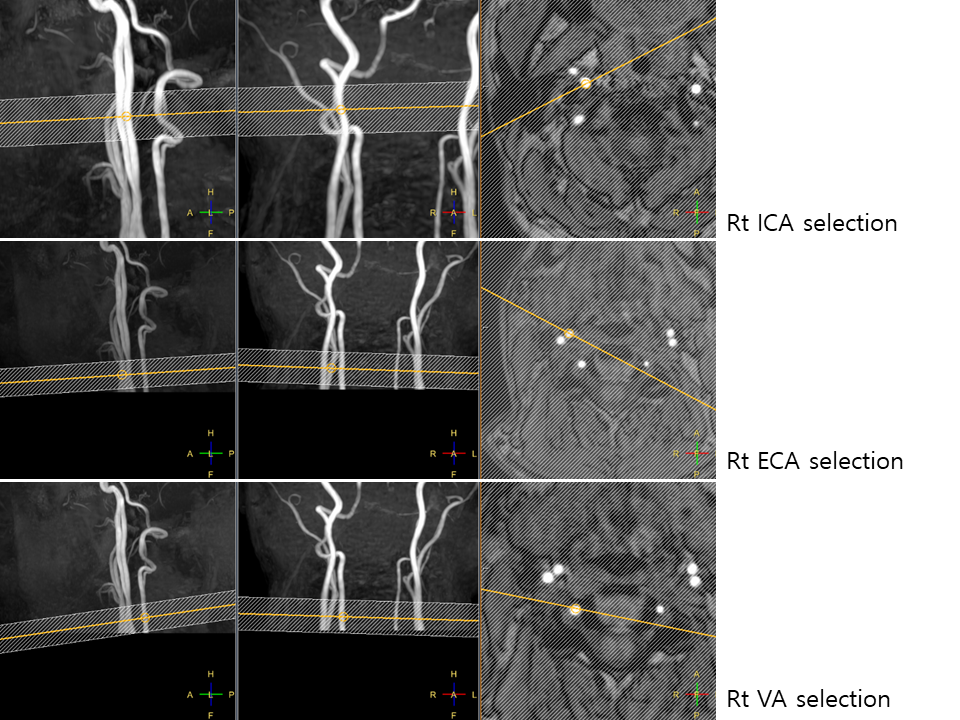
This retrospective study enrolled patients from June 2017 to April 2019 in a single institution by radiology database search. There were 51 SS-ASL perfusion studies in that period. We included the patients who underwent direct and indirect bypass surgery for moyamoya disease, performed SS-ASL and DSA preoperatively and postoperative six months. Finally, 26 patients with 28 hemispheres of bypass surgery were included in our study populations. The patients underwent SS-ASL by 3D pseudo-continuous ASL technique, using 3 T MR scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands), on each side of the internal and external carotid arteries (ICA and ECA), and one side of the vertebral artery (VA). The imaging time of all five vessels was about 15 minutes. The patients also underwent DSA after the selection of each side of ICA, ECA, and one side of VA with 5 Fr catheter. The image was subjectively analyzed to evaluate the areas of revascularization in each modality, by modified Matsushima grade.3 The changes in contralateral ECA and VA supplying territory were compared. Besides, we performed collateral grading of each SS-ASL images and DSA, guided by the Alberta Stroke Program Early CT Score (ASPECTS).4 We statistically analyzed the agreement of two modalities by weighted kappa statistics.RESULTS
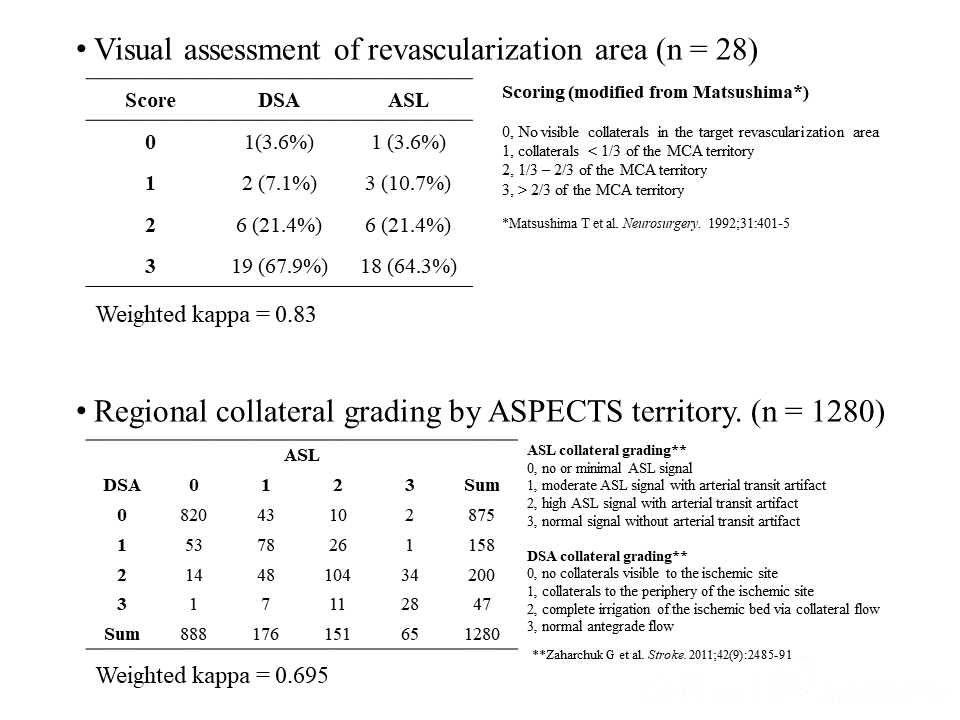
There were 19 and 18 hemispheres with revascularization grade 3 [>2/3 of middle cerebral artery(MCA) territory] by DSA and ASL, respectively. Only one hemisphere was no visible collaterals in the target revascularization area on DSA and ASL. The agreement of the revascularization area between DSA and ASL was excellent, with a weighted kappa value of 0.83. In the case of present preoperative contralateral ECA collateral (n = 3), one was decreased, and two were not changed of collateral on DSA, and all three were not changed on ASL. In the case of absent preoperative contralateral ECA collateral (n= 16), seven were developed contralateral ECA supply post-operatively, and six were similarly visualized on ASL. All patients had collaterals preoperatively from VA. VA collaterals were disappeared in four patients on DSA, but seven on ASL. The agreement of collateral grading in postoperative bypass side ECA territory imaging was good, with a weighted kappa value of 0.695. The overall agreement of collateral grading in all territories of the postoperative study was good, with a weighted kappa value of 0.722.DISCUSSION
Our study demonstrated that SS-ASL showed excellent agreement with DSA to assess the Matsushima revascularization grade. Qualitative collateral grading using ASPECTS regions also gives good agreement between SS-ASL and DSA. The conventional perfusion imaging such as ASL could be used to evaluate perfusion changes after bypass surgery. However, SS-ASL is the only MR technique that gives information about the revascularization area by a bypass. Therefore, our study supports the alternative or supplemental use of SS-ASL to a non-invasive evaluation of the revascularization status. Another merit of SS-ASL is that it gives cross-sectional images; the exact location of perfusion territory can be evaluated more precisely than projection images by DSA. There were a few limitations in SS-ASL. The SS-ASL takes a longer time than conventional ASL images. It is vulnerable to motion artifact; subtle patient movement can cause mislabeling to other vessels. In the case of the indirect dominant bypass, the arterial transit time is prolonged, which causes a decrease of perfusion signal with increased arterial transit artifact. Finally, SS-ASL still cannot give quantitative blood flow information. Additional use of conventional ASL perfusion could be a solution to quantify the CBF as well as to investigate perfusion territory by SS-ASL.CONCLUSION
SS-ASL could evaluate revascularization territory precisely in the patient of moyamoya disease who underwent bypass surgery. In addition, it also could visualize the changes in the vascular supplying territories before and after bypass surgery.Acknowledgements
No acknowledgement found.References
1. Kim JS. Moyamoya Disease: Epidemiology, Clinical Features, and Diagnosis. J Stroke 2016;18:2-112.
2. Hartkamp NS, Petersen ET, De Vis JB, et al. Mapping of cerebral perfusion territories using territorial arterial spin labeling: techniques and clinical application. NMR Biomed 2013;26:901-9123.
3. Matsushima T, Inoue T, Suzuki SO, et al. Surgical treatment of moyamoya disease in pediatric patients--comparison between the results of indirect and direct revascularization procedures. Neurosurgery 1992;31:401-4054.
4. Kim JJ, Fischbein NJ, Lu Y, et al. Regional angiographic grading system for collateral flow: correlation with cerebral infarction in patients with middle cerebral artery occlusion. Stroke 2004;35:1340-1344
Figures