1601
CAWE and higher WEI on VW-MRI were associated with symptomatic unruptured intracranial aneurysms1Department of Magnetic Resonance, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2Department of Interventional Neuroradiology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 3Department of Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States
Synopsis
This study aimed to demonstrate the feasibility of aneurysmal wall enhancement (AWE) and wall enhancement index (WEI) in the identification of symptomatic and asymptomatic unruptured intracranial aneurysms by using vascular wall magnetic resonance imaging (VW-MRI) in a large cohort of Chinese patients with unruptured intracranial aneurysms (UIAs). VW-MRI were obtained at MAGNETOM Skyra/Verio/Prisma 3T MR scanner (Siemens Healthcare, Erlangen, Germany) in these patients. We found CAWE and WEI>0.91 were more frequently identified in symptomatic UIAs.
Introduction/Purpose
To explore the value of aneurysmal wall enhancement (AWE) and wall enhancement index (WEI) in vascular wall magnetic resonance imaging (VW-MRI) in the identification of symptomatic and asymptomatic unruptured intracranial aneurysms in Chinese.Method
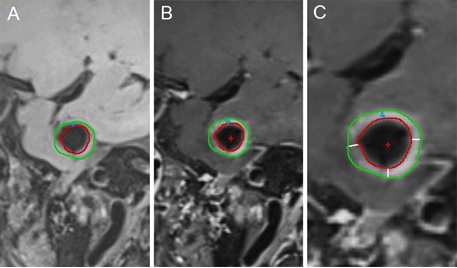
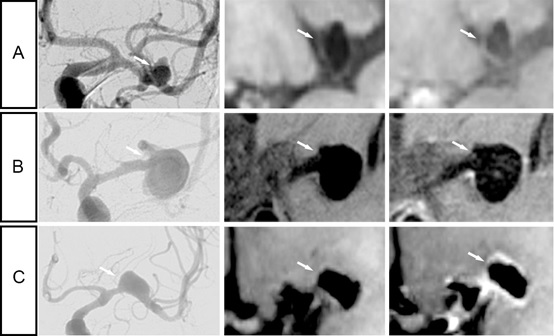
Patients were included from October 2014 to July 2019. Vessel wall images (VW-MRI) were acquired at 3T MR in patients with unruptured intracranial aneurysms (UIAs). 2D VW-MRI were collected on a MAGNETOM Skyra/Verio 3T MR scanner (Siemens Healthcare, Erlangen, Germany) with a 16-channel head coil. The scanning parameters of the T1 WI was, with 130 × 130mm field of view, a voxel size of 0.5 × 0.5 × 2mm; a scan comprising 5 slices, a repetition time/echo time of 861/18 ms. The total imaging time was 4 minutes and 55 seconds per sequence. 3D VW-MRI were collected on a MAGNETOM Prisma 3T MR scanner (Siemens Healthcare, Erlangen, Germany) with a 64-channel head coil. The scanning parameters of the three-dimensional sampling perfection with application optimized contrasts using different flip angle evolutions (3D SPACE) was, with 200 × 200 × 200mm field of view, a voxel size of 0.6 × 0.6 × 0.6mm; a scan comprising 224 slices, a repetition time/echo time of 800/14 ms. The total imaging time was 7 minutes and 36 seconds per sequence. Gadopentetate chelate (Magnevist; Bayer HealthCare Pharmaceuticals) was administered intravenously (0.1 mmol/kg), and the 3D SPACE (or T1-weighted imaging sequence) was repeated 5min after the contrast agent was infused. This study included 225 patients (89 symptomatic patients and 136 asymptomatic patients). Each aneurysm was evaluated by two readers to determine whether an AWE was present and its classification according to FAWE and CAWE(Figure 3). Then, quantitative analyses of AWE were performed by two readers to calculate the WEI. The vessel wall and alba signal intensity (SI) was measured by the Vessel-MASS software(Figure 2). The WEI was calculated as follows: ([SIwall/SIbrain on postcontrast imaging]-[SIwall/SIbrain on matched precontrast imaging])/(SIwall/ SIbrain on matched precontrast imaging)1, 2.Result
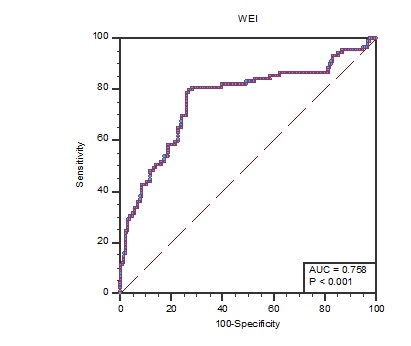
This study included 225 patients with 273 UIAs. Inter-reader agreement was excellent for the presence of AWE (k = 0.90 [95% confidence interval: 0.85 to 0.95]), AWE's classification (k = 0.89 [95% confidence interval: 0.84 to 0.93]) and the calculation of WEI (k = 0.97 [95% confidence interval: 0.96 to 0.97]). A CAWE was significantly more frequently observed in symptomatic than in asymptomatic UIAs (59/89, 66.3% versus 32/184, 17.4%, respectively; P = 0.0002). The WEI was significantly higher in symptomatic than in asymptomatic UIAs (1.3 ± 0.8 versus 0.6 ± 0.6, respectively; P < 0.0001). Multivariate logistic regression revealed that CAWE (odds ratio, 28.11; 95% confidence interval, 11.18 to 70.70; P<0.0001) and WEI (odds ratio, 4.99; 95% confidence interval, 3.12 to 7.98; P<0.0001) were the only independent factors associated with symptomatic UIAs. The receiver operating characteristic curve analysis found that the most reliable associated criterion of the WEI to differentiate symptomatic from asymptomatic UIAs was 0.91 (sensitivity, 80.9%; specificity, 71.7%), and the areas under the curve were 0.76 (P<0.0001)(Figure 1).Discussion
In this study, we found that CAWE and higher WEI were more commonly seen in symptomatic UIAs by using VW-MRI on a large sample of UIAs (about 300 aneurysms)3, 4. This study confirmed that CAWE could identify symptomatic UIAs through qualitative research with a larger sample size, and further confirmed that WEI>0.91 had a sensitivity of 80.9% and specificity of 71.7% in identifying symptomatic UIAs through quantitative methods.Conclusion
In conclusion, we confirmed CAWE and higher WEI were more commonly seen in symptomatic UIAs. This finding is conducive to risk stratification of UIAs in clinical practice and individualized evaluation of treatment for corresponding Chinese patients.Acknowledgements
References
1. Lou X, Ma N, Ma L, Jiang WJ. Contrast-Enhanced 3T High-Resolution MR imaging in symptomatic atherosclerotic basilar artery stenosis. Am J Neuroradiol. 2013;34:513-517
2. Omodaka S, Endo H, Niizuma K, Fujimura M, Inoue T, Sato K, Sugiyama SI, Tominaga T. Quantitative assessment of circumferential enhancement along the wall of cerebral aneurysms using MR imaging. Am J Neuroradiol. 2016;37:1262-1266
3. Edjlali M, Guédon A, Ben Hassen W, Boulouis G, Benzakoun J, Rodriguez-Régent C, Trystram D, Nataf F, Meder J, Turski P, Oppenheim C, Naggara O. Circumferential thick enhancement at vessel wall MRI has high specificity for intracranial aneurysm instability. Radiology. 2018;289:181-187
4. Fu Q, Guan S, Liu C, Wang K, Cheng J. Clinical significance of circumferential aneurysmal wall enhancement in symptomatic patients with unruptured intracranial aneurysms: A high-resolution MRI study. Clin Neuroradiol. 2017
Figures