1592
FDG-PET imaging shows mesiotemporal hypometabolism in MRI-negative temporal lobe epilepsy1USC Stevens Neuroimaging and Informatics Institute, University of Southern California, Los Angeles, CA, United States, 2UCSF Weill Institute for Neurosciences, San Francisco, CA, United States, 3University of Alabama at Birmingham, Birmingham, AL, United States
Synopsis
The pathophysiology of MRI-negative temporal lobe epilepsy is not well understood. Here, we used a surface-based approach for investigating metabolic changes in the subregions of mesiotemporal structures for MRI-negative TLE patients. We found significant hypometabolism in the anterior to the intermediate hippocampus, the intermediate entorhinal cortex and the centro-medial and laterobasal amygdala. In patients with poor outcome, metabolism tended to be more interhemispherically symmetric in all three regions compared to those with good outcome, which suggests a more complicated seizure origin in this subtype of the disorder.
Introduction
The pathophysiology of MRI-negative temporal lobe epilepsy (TLE) is not well understood. In addition, it represents a challenge for surgical planning due to the lack of identifiable lesions and its association with poorer surgical outcomes compared to MRI-positive cases.1 For TLE patients with normal hippocampal volume, however, previous studies showed subtle volume changes in subregions of mesiotemporal lobe (MTL) structures including the hippocampus, amygdala and entorhinal cortex.2 Here, for the first time, we proposed to use a surface-based approach that allowed us to investigate metabolic changes in the subregions of MTL structures for MRI-negative TLE patients and to what extent it is able to explain seizure lateralization and surgical outcome.Methods
Dataset: Patients (N=58) with either left (N=31) or right (N=27) lateralized MRI-negative TLE between the ages of 14 and 70 were collated from the databases of University of California, San Francisco and University of Alabama, Birmingham. Both 3D T1-MPRAGE MRI and [18F] FDG-PET were acquired prior to temporal lobectomy and the Engel score was used to assess patient outcome at 1-year post surgery.Image Processing: The hippocampus, entorhinal cortex and amygdala were each segmented on T1-MPRAGE MRI using a multi-atlas and label fusion method.3 These segmentations were converted to a spherical harmonic description (SPHARM), then sampled into triangulated surfaces using point-distribution models (SPHARM-PDM).4 The PET intensity was normalized using the mean intensity of each individual’s white-matter and CSF voxels, then was projected onto the SPHARM surface. The asymmetry was calculated as the difference between the ipsilateral and contralateral hemispheres divided by their sum.
Results
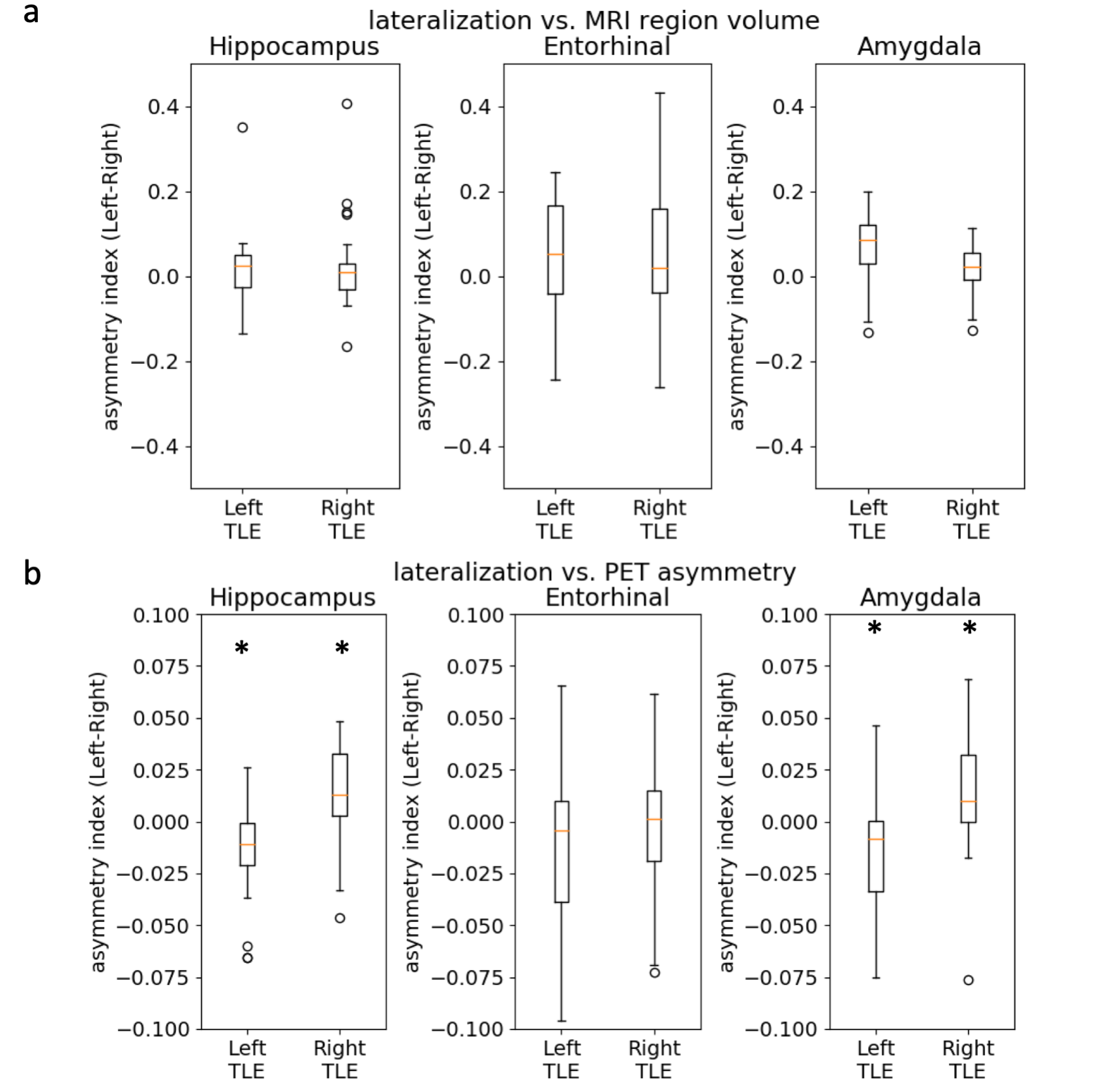
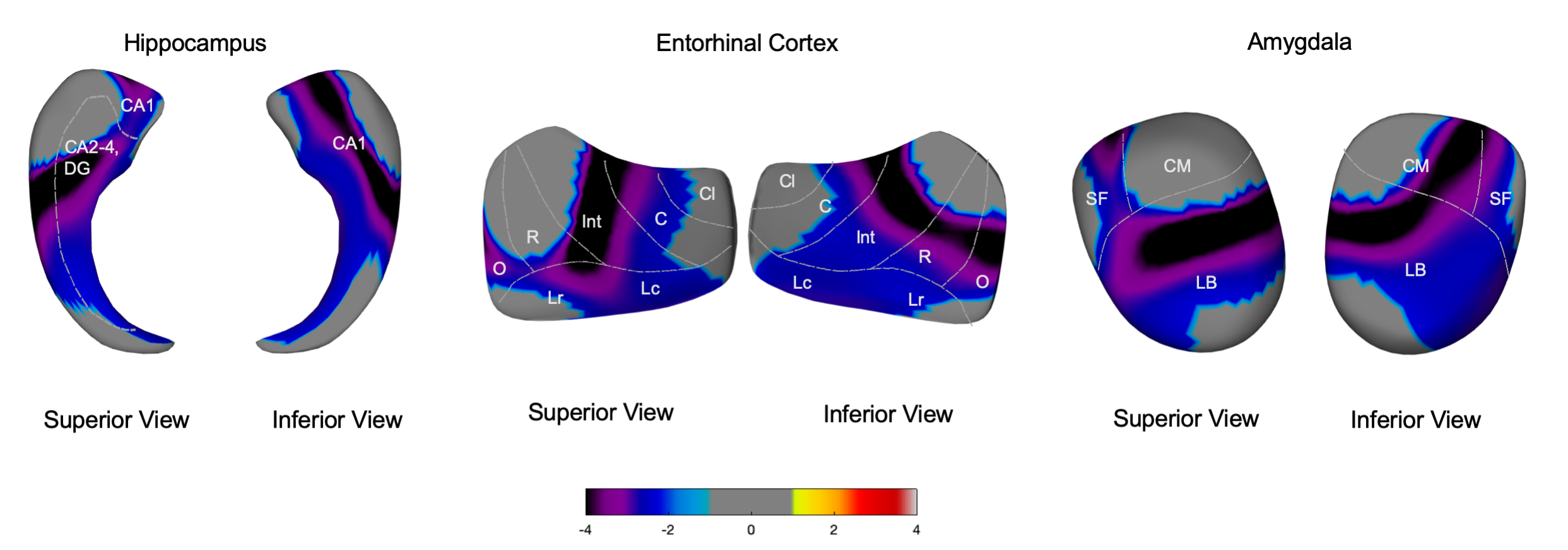
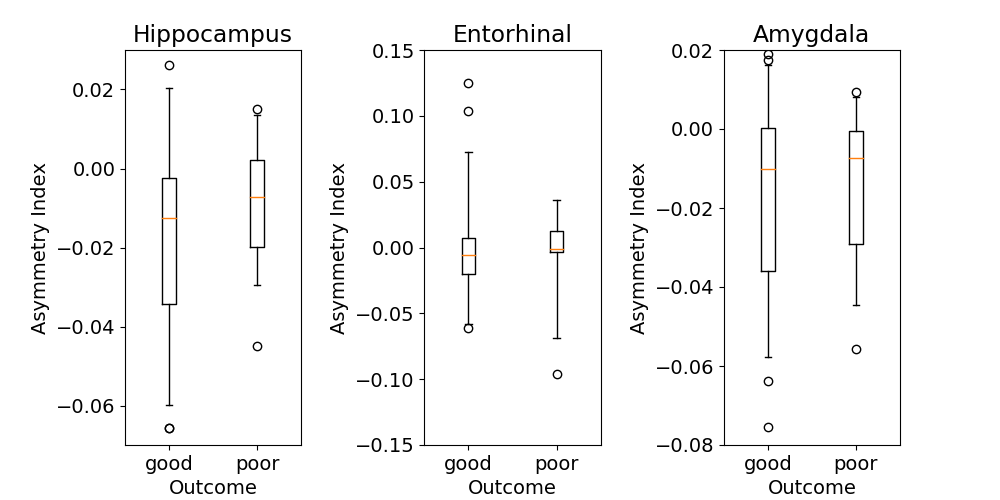
We first investigated the presence of asymmetries in the medial temporal lobe regions. Volumes were not significantly asymmetric in the hippocampus, amygdala or entorhinal cortex, although left TLE patients exhibited a slightly larger amygdala ipsilateral to the epileptogenic region (Fig. 1a). There was significant hypometabolism on FDG-PET in the hippocampus and amygdala for both left and right TLE patients (p<0.05), i.e. lower metabolism in the MTL structures ipsilateral to the epileptic focus compared to the contralateral side (Fig. 1b). Using SPHARM-PDM, we analyzed the pattern of these asymmetries across cytoarchitectonic subregions for each of the MTL structures (Fig. 2). The significant hypometabolism in the MTL ipsilateral to the focus was mapped in the anterior to the intermediate hippocampus, the intermediate entorhinal cortex and the centro-medial and laterobasal amygdala. Finally, we investigated whether this asymmetry differed between patients with good surgical outcome (Engel 1) and poor outcome (Engel score 2-4) (Fig. 3). In patients with poor outcome, metabolism was more interhemispherically symmetric in all 3 regions compared to those with good outcome (Engel 1), although this did not reach statistical significance p>0.2. In addition, there were no significant local associations between asymmetry and outcome.Conclusions
Here, we investigated the distribution of hypometabolism in the medial temporal lobe in MRI-negative TLE patients. Asymmetry was highest in the anterior to intermediate hippocampus, intermediate entorhinal cortex, lateral-baso and centro-medial amygdala. We also found a trend of less asymmetric hypometabolism in patients with poor surgical outcome. The nature of interhemispherically symmetric metabolism in this group potentially suggests a more complicated seizure origin in these types of patients and could relate to the lower likelihood of seizure freedom after surgery. The absence of healthy controls is a primary limitation of the current study, which complicates interpretation of the findings (e.g., whether there exists bilateral hypometabolism or normal metabolism).Acknowledgements
This study is supported by the National Institutes of Health grants (P41EB015922) and the BrightFocus Foundation grant (A2019052S).References
1. Muhlhofer W, Tan YL, Mueller SG, Knowlton R. MRI-negative temporal lobe epilepsy-What do we know? Epilepsia. 2017;58(5):727-742.
2. Bernhardt BC, Hong SJ, Bernasconi A, Bernasconi N. Magnetic resonance imaging pattern learning in temporal lobe epilepsy: classification and prognostics. Ann Neurol. 2015;77(3):436-446.
3. Wang H, Suh JW, Das SR, Pluta JB, Craige C, Yushkevich PA. Multi-Atlas Segmentation with Joint Label Fusion. IEEE Trans Pattern Anal Mach Intell. 2013;35(3):611-623.
4. Styner M, Oguz I, Xu S, Brechb¨uhler C, Pantazis D, Gerig G. Statistical Shape Analysis of Brain Structures using SPHARM-PDM. MICCAI 2006 Opensource workshop; 2006.
Figures