1590
White matter alterations in mild traumatic brain injury: A tract-based spatial meta-analysis exploring the effects of trauma type1Huaxi MR Research Center (HMRRC), Department of Radiology, West China Hospital of Sichuan University, ChengDu City, China
Synopsis
Many tract-based spatial statistics (TBSS) studies in mild traumatic brain injury (mTBI) have been inconsistent. Meanwhile, there is evidence that trauma type may have an effect on white matter (WM) microstructure in mTBI. We performed a tract-based spatial meta-analysis of mTBI and examined the potential effects of trauma type on regional WM microstructure. Our findings identified the left anterior thalamic radiation and right superior longitudinal fasciculus were the most convergent circuitry affected in mTBI and indicated distinct patterns of anatomical connectivity abnormalities in accident related and sport related mTBI, which highlighted the potential importance of trauma specific alterations in mTBI.
Introduction
Mild traumatic brain injury (mTBI) is synonymous with concussion and is typically caused by blunt non-penetrating head trauma. The trauma causes stretching and tearing of axons, which results in diffuse axonal injury [1]. Identification of white matter (WM) microstructural alterations is a momentous step for gaining insights about underlying mechanisms of mTBI and improving the efficacy of therapies for this condition. Many tract-based spatial statistics (TBSS) studies have revealed abnormalities of fractional anisotropy (FA; an index of WM integrity) in mTBI. However, researches have not drawn robust conclusions. Furthermore, there is evidence that trauma type may have an effect on brain structural connectivity [2]. Therefore, we integrated the findings of TBSS studies to identify the most consistent FA changes in mTBI using meta-analytical approach and examined the potential effects of trauma type on regional WM microstructure.Methods
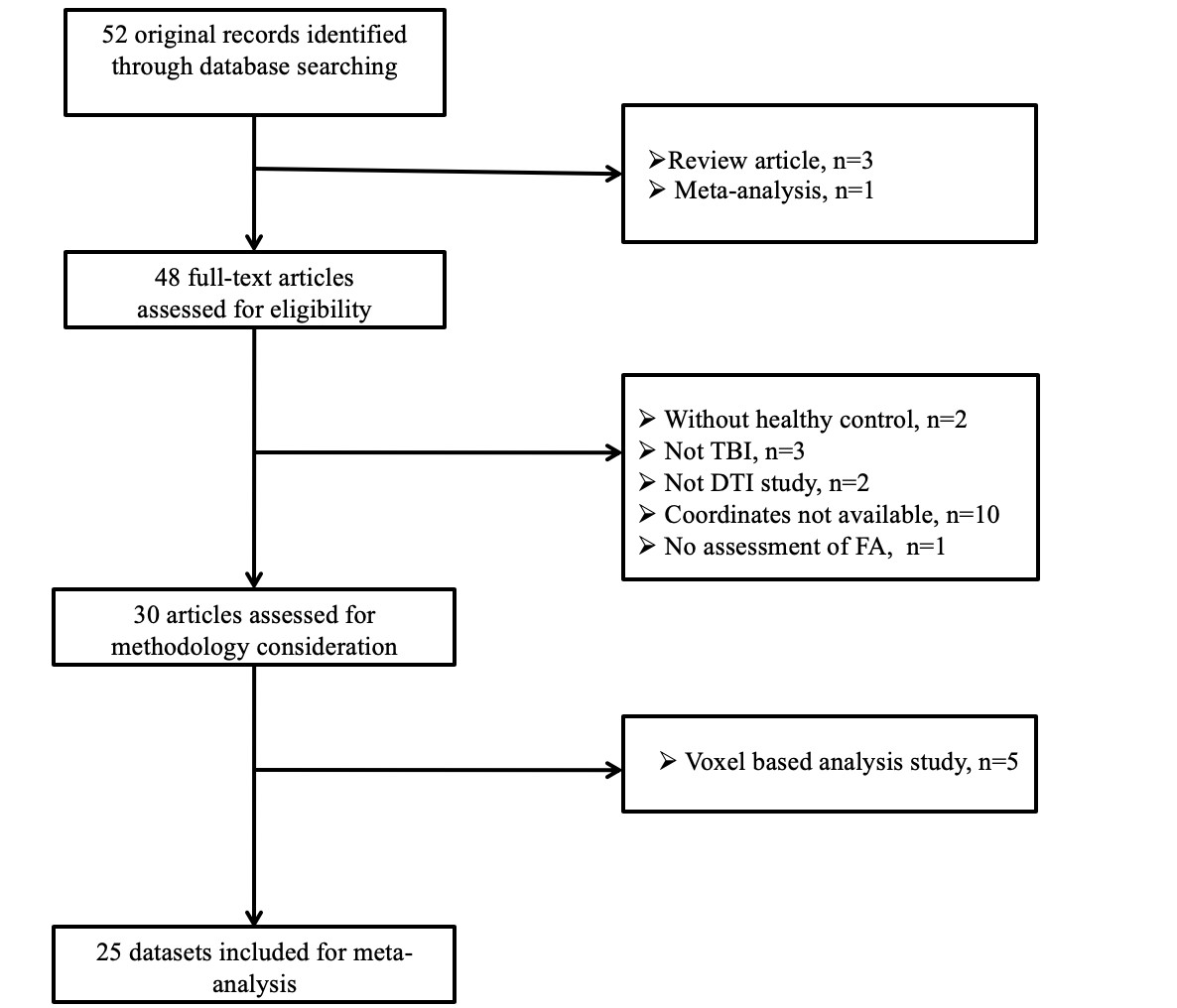
Systematic and comprehensive searches of the PubMed, ISI Web of Science, Medline, Cochrane Library, and EMBASE databases were performed to identify whole-brain TBSS studies comparing FA between mTBI patients and HCS published between January 1999 and October 2019 and “in press” articles. The keywords for the search were “mild traumatic brain injury” plus ("diffusion tensor imaging" or "DTI") or ("fractional anisotropy" or "FA") or ("tract-based spatial statistics" or "TBSS"). The reference lists of identified articles and review articles were manually scrutinized to obtain additional papers. Coordinates were extracted from clusters of significant FA difference between TBI patients and HCS. The current voxel-wise meta-analysis was performed using Anisotropic effect size signed differential mapping (AES-SDM) software [3]. First, we performed pooled meta-analyses of all the included studies. Meanwhile, a systematic whole-brain voxel-based jackknife sensitivity analysis was carried out to test the replicability of the main results. A threshold of P < 0.005 with peak Z > 1 and a cluster extent of > 10 voxels was used for the meta-analyses and jackknife sensitivity analyses. Additionally, we performed subgroup meta-analyses regarding trauma type (accident-related mTBI and sport-related mTBI). Finally, meta-regression analyses were conducted with the duration between injury and mTBI as regressor. As in previous studies [4], the results from the meta regressions were thresholded more conservatively (P < 0.0005) and were only considered when significant slopes were accompanied by significant differences at one extreme. All these analytical processes are described in the AES-SDM tutorial (https://www.sdmproject.com) and related publications.Results
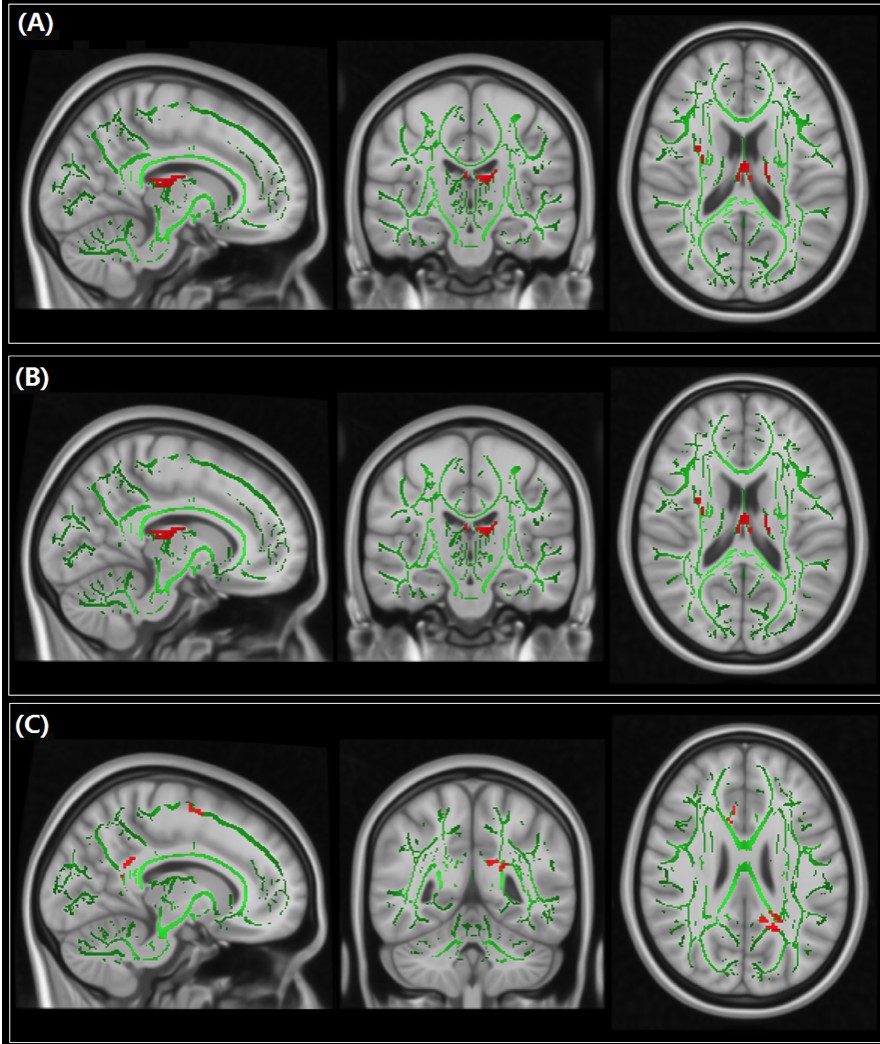
A total of 25 datasets were enrolled, including 745 mTBI patients and 589 HCS(Figure 1). FA reductions were identified in the left anterior thalamic radiation (ATR) and the right superior longitudinal fasciculus (SLF) in patients with mTBI relative HCS (Figure 2A). The whole brain jackknife sensitivity analysis indicated that FA reductions in the current meta-analysis were highly replicable as these findings remained significant in all but one combinations of studies(Figure 3).The findings of the subgroup meta-analysis regarding accident-related mTBI (15 datasets, 486 mTBI patients vs. 384 healthy controls) remained the same as the main effect of pooled meta-analysis (Figure 2B). However, in the subgroup meta-analysis concerning sport-related mTBI (10 datasets, 259 mTBI patients vs. 205 healthy controls), lower FA was identified in the body and splenium of the corpus callosum, the cingulum bundle and the white matter of the left supplementary motor area (Figure 2C). Meta-regression analysis didn’t reveal significant association between the duration from injury to mTBI and FA changes.
Discussion & Conclusion
Our results identified lower FA in the left ATR and the right SLF in patients with mTBI than HCS, which was in agreement with published meta-analysis [5]. Additionally, obvious differences were found in subgroup between sport-related and accident-related mTBI. As white matter is sensitive to micro injury, our results provide evidence for effect of different traumatic injury on brain structure and function. In addition, the methodological differences between TBSS and voxel based analysis (VBA) might lead to ambiguous results, so merely the former approach were included in current meta-analysis, which make our meta analysis more reliable in particularly for those WM tracts surrounding the ventricular system[6].Our meta-analysis gave a thorough profile for the WM abnormalities in mTBI and identified left ATR and right SLF as the most convergent circuitry in mTBI. More importantly, accident-related mTBI is associated with the disruption of the deep WM especially the ATR while sport-related mTBI is related to midline tract abnormalities including the corpus callosum and the cingulum bundle. These findings indicated distinct patterns of anatomical connectivity abnormalities in accident-related and sport-related mTBI, which highlighted the potential importance of trauma specific alterations in mTBI.
Acknowledgements
This study was supported by National Nature Science Foundation (Grant NO. 81671669), Science and Technology Project of Sichuan Province (Grant NO. 2017JQ0001).References
[1].Blennow, K., et al., Traumatic brain injuries. Nat Rev Dis Primers, 2016. 2: p. 16084.
[2].Schneider, D.K., et al., Diffusion Tensor Imaging in Athletes Sustaining Repetitive Head Impacts: A Systematic Review of Prospective Studies. J Neurotrauma, 2019. 36(20): p. 2831-2849.
[3].Radua, J., et al., Anisotropic kernels for coordinate-based meta-analyses of neuroimaging studies. Front Psychiatry, 2014. 5: p. 13.
[4].Radua, J. and D. Mataix-Cols, Voxel-wise meta-analysis of grey matter changes in obsessive-compulsive disorder. Br J Psychiatry, 2009. 195(5): p. 393-402.
[5].Aoki, Y. and R. Inokuchi, A voxel-based meta-analysis of diffusion tensor imaging in mild traumatic brain injury. Neurosci Biobehav Rev, 2016. 66: p. 119-26.
[6].Wise, T., et al., Voxel-Based Meta-Analytical Evidence of Structural Disconnectivity in Major Depression and Bipolar Disorder. Biol Psychiatry, 2016. 79(4): p. 293-302.
Figures
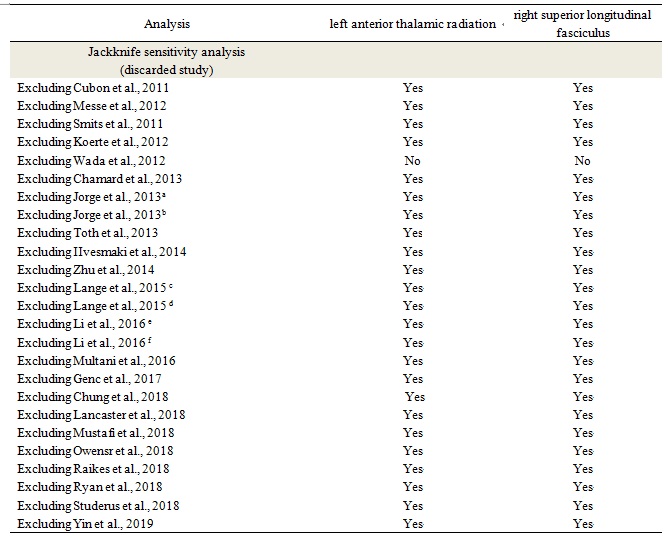
Results of the sensitivity and subgroup analysis of regions with lower fractional anisotropy from 25 datasets included in the meta-analysis.
Note: a. Subgroup of possible mTBI patients. b. Subgroup of probable mTBI patients. c. Subgroup of postconcussional syndrome absent mTBI patients. d. Subgroup of postconcussional syndrome presesnt mTBI patients. e. Subgroup of poor recovery mTBI patients. f. Subgroup of successful recovery mTBI patients.