1583
Conventional and synthetic MRI in children with drug-resistant epilepsy: a comparative study
XIAONA Zhang1, QUANXIN YANG1, and XIAOCHEN WEI2,3
1The Second affiliated hospital of Xi'an JiaoTong Uuniversity, Xi'an, China, 2GE Healthcare, MR Research China, Beijing, China, 3GE Healthcare, MR Research China, Xi'an, China
1The Second affiliated hospital of Xi'an JiaoTong Uuniversity, Xi'an, China, 2GE Healthcare, MR Research China, Beijing, China, 3GE Healthcare, MR Research China, Xi'an, China
Synopsis
The current study aims to assess whether multi-contrast qualitative and quantitative relaxation imaging derived from the synthetic MRI can enhance detection of epileptogenic lesions in children. It was concluded that the synthetic MRI has the potential to be more sensitive in detecting lesions than conventional neuroimaging. Studies with more patients are needed to further demonstrate the relative advantages of the synthetic MRI over conventional MRI, and compare the synthetic MRI with 3-dimentional high resolution MRI.
Introduction
Epilepsy affects approximately 50 million people around the world. Up to 40% of individuals with epilepsy have drug-resistant epilepsy[1]. Surgery has been shown to be effective and cost-effective to this population. Brain imaging has a crucial role in the presurgical assessment of patients who may be potential surgery candidates. Unfortunately, greater than 20% of patients with drug-resistant epilepsy do not have a structural lesion visible on conventional MRI neuroimaging, which may be due to the lack of contrast in conventional MRI neuroimaging. The recently developed synthetic MRI technology, with four saturation delays and two echo times, is able to generate variable qualitative, weighted imaging as well as quantitative maps[2]. Studies have shown that the synthetic MRI has shorter scan time, better imaging contrast, and quantitative measurement of normal appearing brain tissue. The current study aims to investigate whether the synthetic MRI can enhance detection of epileptogenic lesions relative to conventional neuroimaging in children with drug-resistant epilepsy.Material and Methods
A total of 52 infants and children (age 8±2 years, age range 3-15 years) were included in this study. The mean duration of epilepsy at the time of evaluation was 6 years (range 2-11 years). All brain imaging was performed on a 3-T MRI system (Pioneer, GE Healthcare) with a 21-channel head coil. All patients underwent a synthetic MR sequence (fast spin echo multi-dynamic multi-echo sequence) in addition to conventional MR sequences. The synthetic MR sequence includes four saturation delays and two echo times. Each acquisition produced 16 complex images per section with different echo time and saturation delay combinations. The synthetic sequence parameters were as follows: TR=4600ms, two echo times (TEs, 20.3 and 101.7 ms), four delay times (146, 546, 1879, and 3879 ms), Bandwidth=22.5kHz, NEX=1, FOV=24cm×24cm, slice thickness/gap=4/0.5mm, matrix=320×256, and scanning time = 5 min 20 s. The synthetic weighted images, including T1- , PD-, and T2-weighted images, T1- and T2-FLAIR, short time inversion recovery (STIR), phase sensitive inversion recovery (PSIR) and PSIR Vessel, double IR gray matter (DIR-GM) . double IR white matter (DIR-WM), and quantitative relaxation images, included T1-, T2-, R1-, R2, and PD-map, were generated from the raw data produced by synthetic imaging sequence using a vendor-provided program (MAGiC,version 100.1.1). Conventional T1- and T2-weighted images and T2-FLAIR images were acquired based on the standard imaging protocol of our institution. Total acquisition time for conventional imaging sequences was 7 min 5 s. The conventional and synthetic MR image data sets were evaluated separately by two neuroradiologists. Interobserver agreement was assessed by weighted kappa statistics. Clinical epilepsy data, including Video-electroencephalography findings and seizure semiology, was recorded.Results
All of 52 studies, 34 had a lesion identified with 21/34 abnormalities being non-specific. Of 13 remaining studies, 10 (19%) demonstrated suspicious lesion on the conventional imaging, and significant lesion on synthetic PSIR, DIR-GM and R2 map (Fig 1), and 3 (6%) revealed quantitative abnormalities only on synthetic T1- and T2- map, and R1- and R2- map (Fig 2). The synthetic MRI lesions were concordant with clinical epilepsy data in all 13 subjects. Interobserver agreement between the two neuroradiologists was perfect for the synthetic MRI (k = 0.96), and moderate for conventional imaging (k = 0.62).Discussion and Conclusion
To our best knowledge, this is a preliminary study of applying the synthetic MRI in children with drug-resistant epilepsy. As compared with conventional neuroimaging, the synthetic MRI could identify lesion more significantly in 19% and uniquely in 6% of our patients, with shorter acquisition time. PSIR of the synthetic MRI combines inversion recovery with phase-sensitive reconstruction, while DIR-GM of the synthetic MRI suppresses the signal from both CSF and normal WM. These promote the contrast between gray matter and white matter, and between lesions and the normal-appearing brain tissues[3,4], which could explain that lesion was revealed more significantly. In our study, synthetic quantitative maps were found to be capable of revealing the lesion more significantly. This indicates that quantitative relaxometry might be a sensitive means of revealing early or subtle abnormalities. In conclusion, the synthetic MRI show the potential to be more sensitive in detecting epileptogenic lesions relative to conventional neuroimaging in children with drug-resistant epilepsy. Studies with more patients are needed to further demonstrate the relative advantages of the synthetic MRI over conventional MRI, including 3-dimentional high resolution MRI.Acknowledgements
No acknowledgement found.References
[1] WHO. Epilepsy: a public health imperative. https://www.who.int/mental_health/neurology/epilepsy/report_2019/en/. 2019. [2] Warntjes JB, Leinhard OD, West J, et al. Rapid magnetic resonance quantification on the brain: optimization for clinical usage. Magn Reson Med 2008, 60(2): 320-329. [3] Hou P, Hasan K M, Sitton C W, et al. Phase-sensitive T1 inversion recovery imaging: a time-efficient interleaved technique for improved tissue contrast in neuroimaging. AJNR Am J Neuroradiol 2005, 26(6): 1432-1438. [4] Motegi S, Shimada T, Hayashi N, et al. Double inversion recovery imaging of the brain: deriving the most relevant sequence through real images. Radiol Phys Technol 2017, 10(3): 364-375.Figures
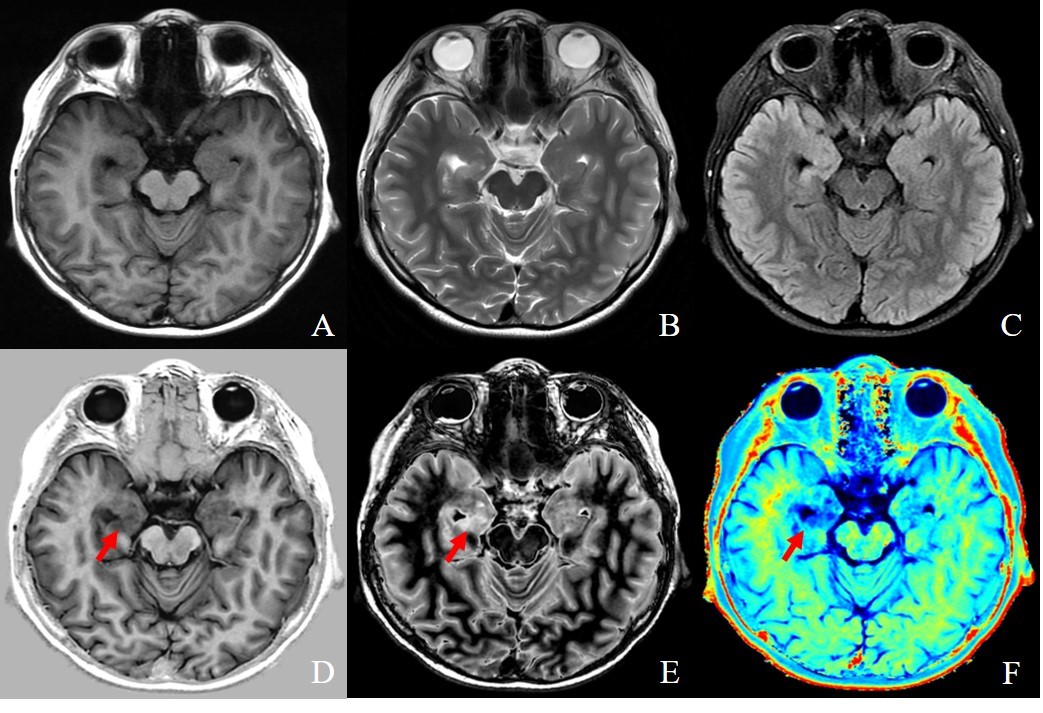
Comparison of conventional
MRI (A ~ C) and synthetic MRI (D~F). Conventional T1FLAIR (A), T2WI (B), and
T2FLAIR(C). Synthetic PSIR (D), DIR GM (E), and R2 Map (F). Red arrow indicates
lesion of right hippocampus.
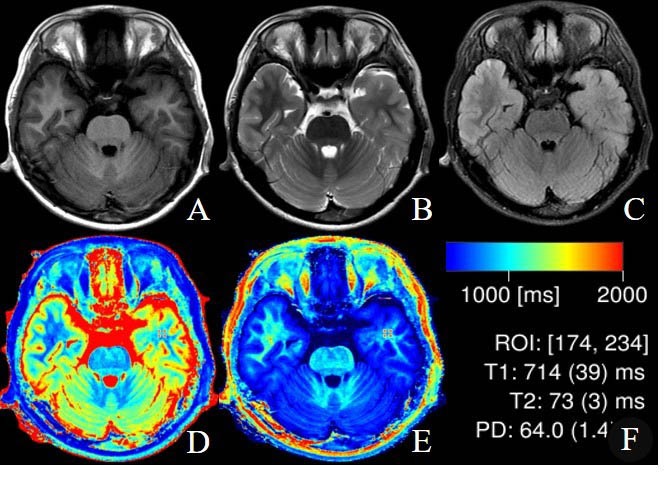
Comparison
of conventional MRI (A ~ C) and synthetic MRI (D~F). Conventional T1FLAIR (A),
T2WI (B), and T2FLAIR(C). Synthetic T1 map (D) and R1 map (E), and the quantitative
result (F, the T1 and T2 relaxation value of white matter of left temporal lobe
decreased; the data of right temporal lobe is not shown ).