1561
Diffusion Kurtosis Imaging Detects Subclinical White Matter Abnormalities in Phenylketonuria
Thomas Welton1, Sarah C Hellewell1, Michel Tchan2, and Stuart M Grieve1
1University of Sydney, Sydney, Australia, 2Department of Genetic Medicine, Westmead Hospital, Sydney, Australia
1University of Sydney, Sydney, Australia, 2Department of Genetic Medicine, Westmead Hospital, Sydney, Australia
Synopsis
Diffusion kurtosis MRI (DKI) was used to measure changes in white matter structure in 20 patients with phenylketonuria and 43 controls. We found significant differences primarily in the periventricular parietal white matter in various DKI metrics. These scores were related to phenylalanine levels measured in the 3 years prior to MRI and with Scheltens score, reflecting white matter hyperintensities. DKI may be sensitive to pathology invisible to clinical MRI, and we propose a simple metric in the parietal lobe which robustly captures this effect.
Introduction
Phenylketonuria (PKU) is an autosomal recessive disorder of amino acid metabolism in which untreated, accumulation of phenylalanine (Phe) metabolites leads to progressive demyelination [1]. Phe levels are used to monitor PKU status, as opposed to any neuronal- or cognitive-based measure, and is treated with a low-protein diet. Non-diet-compliant patients often develop cognitive deficits and periventricular white matter (WM) hyperintensities [2]. Diffuse WM pathology may also be present [3] but may not be measurable with conventional imaging. Diffusion kurtosis imaging (DKI) is an extension of diffusion tensor imaging which uses kurtosis of the water diffusion probability distribution function to account for the non-Gaussianity of diffusion in biological tissue, and can detect subtle changes in brain parenchymal structure. DKI may, therefore, be sensitive to WM pathology in PKU [4]. We investigated the feasibility of DKI as a quantitative biomarker for longitudinal monitoring in clinically well-characterized adults with PKU, with the hypothesis that periventricular WM may show the largest abnormalities, compared to deep and peri-cortical WM.Methods
Our cohort of 20 patients was diagnosed with PKU at birth and variably adhered to a low-protein diet. A control cohort of 43 healthy individuals was matched for gender and age. Plasma Phe concentrations were gathered from clinical records and a computerized neurocognitive battery was performed using WebNeuro [5]. Multi-band DKI data were acquired over 3 shells with b-values of 700, 1000, and 2800 mm/s2, 66 slices, 140 unique gradient directions, TR=4323ms, TE=91.80ms, flip angle=90°, matrix=128x128, voxel dimensions=2mm isotropic and one reverse phase-encoded b=0 volume. DKI data were processed with Diffusion Kurtosis Estimator [6] to create axial, radial, mean and fractional anisotropy diffusion and kurtosis images. Personalised masks were generated from T1-weighted images of the lobes, periventricular, deep, and peri-cortical WM and co-registered to the DKI data. Scheltens score was measured in each patient by a clinical neuroradiologist to quantify WM hyperintensities. We tested for group differences in WM characteristics across our masks. Post hoc analyses were conducted following key findings by correlation with Scheltens score and Phe level in the 3 years prior to imaging.Results
The groups were matched for age (PKU, 35.2±11.5 years; control, 32.8±13.3 years; t-test, t=-0.69, p=0.47) and gender (PKU, 50% female; control, 46% female; χ2=0.067, p=0.80). The PKU group had significantly less cerebral WM (t=2.25, p=0.028), less total intracranial volume (t=2.99, p=0.004), and less CSF (t=2.28, p=0.026). Based on radiological impression, we focussed our analyses on the parietal lobe. Axial diffusivity in the periventricular WM of the parietal lobe clearly differentiated the groups (t=2.55, p=0.013). When comparing this measure across Scheltens scores, controls remained stable, while PKU patients’ parietal periventricular axial diffusivity measure decreased at high Scheltens scores (Figure 1). This measure was highly correlated with mean Phe level across the 3 years prior to imaging (r=-0.607, p=0.005), but not lifetime mean Phe level. At Scheltens scores above 6, the groups were fully differentiated. In the periventricular parietal WM, radial and axial kurtosis were also significantly different between groups (t=0.553, p=0.011; t=-9.59, p=0.021), as well as kurtosis FA (t=2.53, p=0.014). Based on these findings and inspection of scatter plots, we formed a composite measure as the ratio between radial kurtosis and kurtosis FA, measured in the periventricular parietal WM (Figure 2) which strongly differentiated the groups (t=-7.17, p<0.001) and strongly correlated with total Scheltens score (r=0.496, p<0.001).Conclusions
PKU may result in progressive WM changes which are invisible to conventional MRI. Importantly, these changes can occur even in diet-compliant patients, indicating a need for more sensitive, patient-specific monitoring. Our DKI findings suggest highlight the potential for a role of these metrics as future quantitative biomarkers of WM pathology in PKU.Acknowledgements
No acknowledgement found.References
1. Williams, R.A., C.D.S. Mamotte, and J.R. Burnett, Phenylketonuria: an inborn error of phenylalanine metabolism. The Clinical biochemist. Reviews, 2008. 29(1): p. 31-41. 2. Leuzzi, V., et al., The pathogenesis of the white matter abnormalities in phenylketonuria. A multimodal 3.0 tesla MRI and magnetic resonance spectroscopy (1H MRS) study. Journal of Inherited Metabolic Disease, 2007. 30(2): p. 209-216. 3. Phillips, M.D., et al., Diffusion-Weighted Imaging of White Matter Abnormalities in Patients with Phenylketonuria. American Journal of Neuroradiology, 2001. 22: p. 1583-1586. 4. Arab, A., et al., Principles of diffusion kurtosis imaging and its role in early diagnosis of neurodegenerative disorders. Brain Res Bull, 2018. 139: p. 91-98. 5. Silverstein, S.M., et al., Development and validation of a World-Wide-Web-based neurocognitive assessment battery: WebNeuro. Behav Res Methods, 2007. 39(4): p. 940-9. 6. Tabesh, A., et al., Estimation of tensors and tensor-derived measures in diffusional kurtosis imaging. Magn Reson Med, 2011. 65(3): p. 823-36.Figures
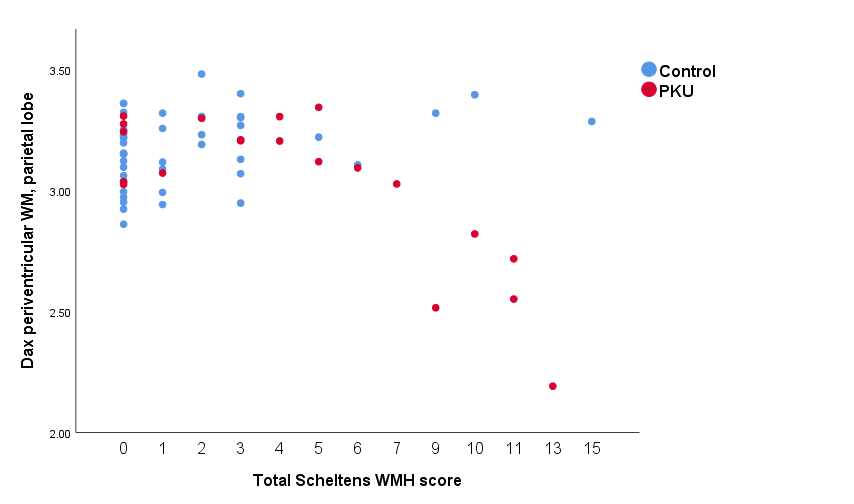
Figure 1. Axial
diffusivity in the periventricular WM of the parietal lobe across the range of Scheltens
scores.
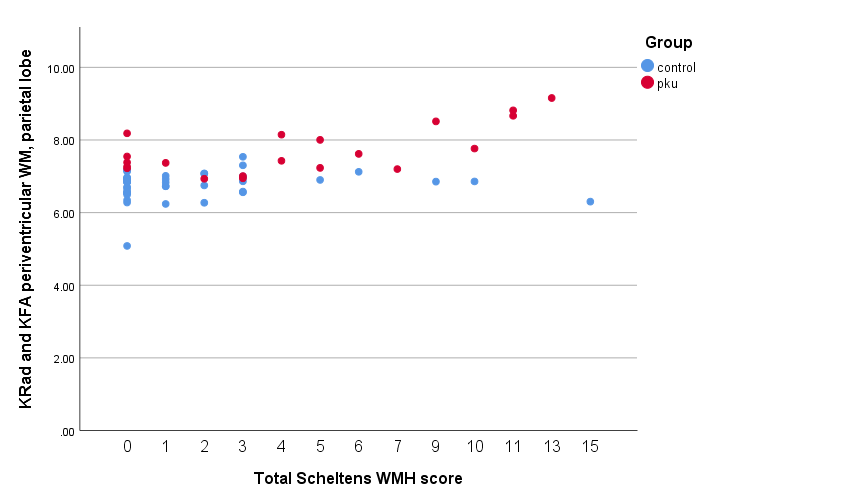
Figure 2. Radial
kurtosis and kurtosis FA in the periventricular parietal WM across the range of
Scheltens scores.