1545
A pilot study of MR–guided focused ultrasound thalamotomy for refractory essential tremor1Chinese PLA General Hospital, Beijing, China, 2Wuhan Institute of Physics and Mathematics, Chinese Academy of Sciences, Wuhan, China
Synopsis
Essential tremor is the most common movement disorder and is often refractory to medical treatment, Deep brain stimulation in the thalamus has proved the efficiency for these patients. However, this treatment has risks associated with an open neurosurgical procedure. MR-guided focused ultrasound has been developed as a non-invasive means of generating precisely placed focal lesions. We examined its application to the management of refractory essential tremor. Satisfactory results were found that the mean reduction in tremor score of the treated hand was 86.7% at 1 month and 72.5% at 3 months, what’s more,no adverse events lasted beyond 3 months.
Introduction and purpose
Recent advances have suggested the favorable efficacy and safety in treatment of refractory essential tremor (ET) with MR–guided focused ultrasound (MRgFUS) thalamotomy1-3. The objective of this study is tantamount to further verify the efficacy and safety of MRgFUS in treatment of refractory ET.Methods
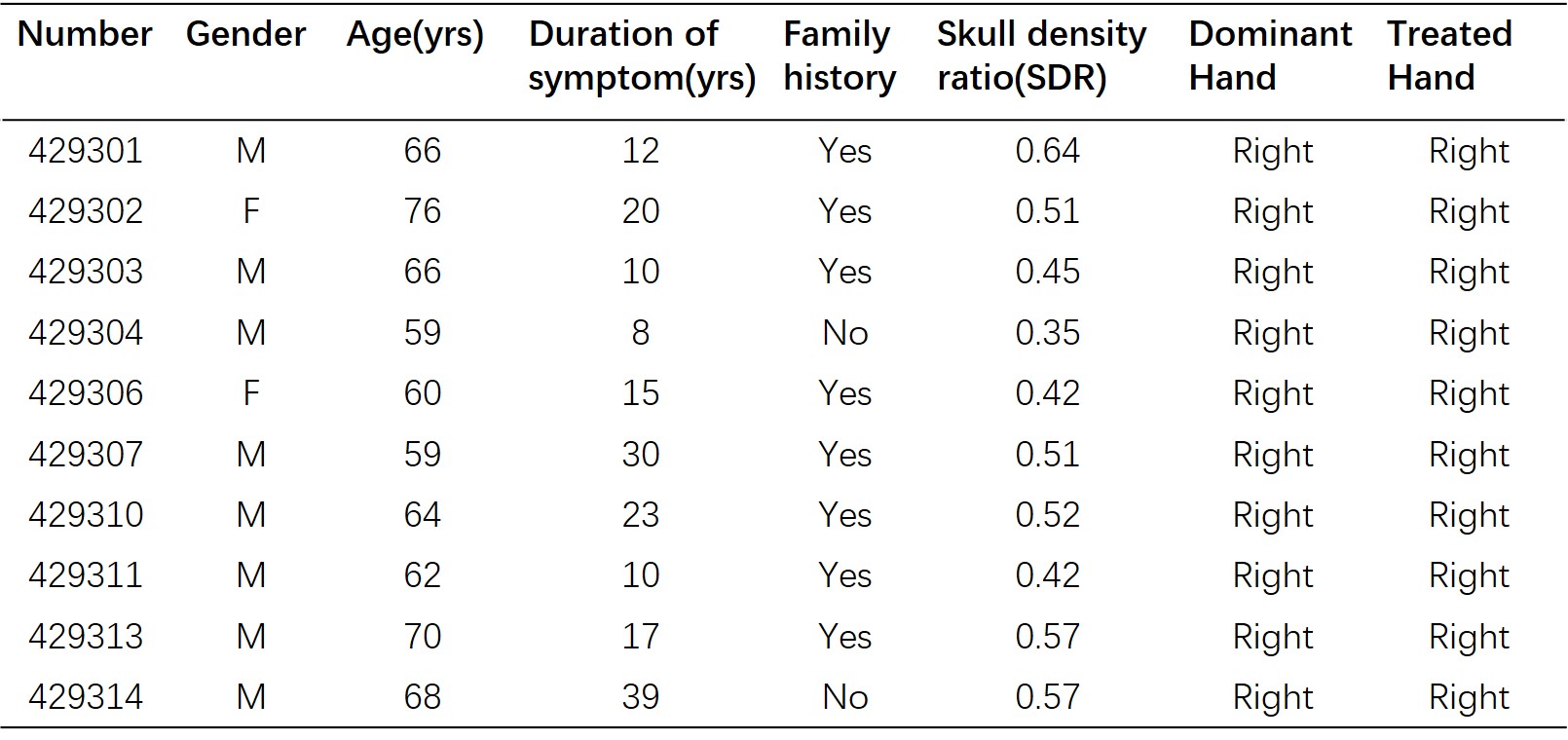
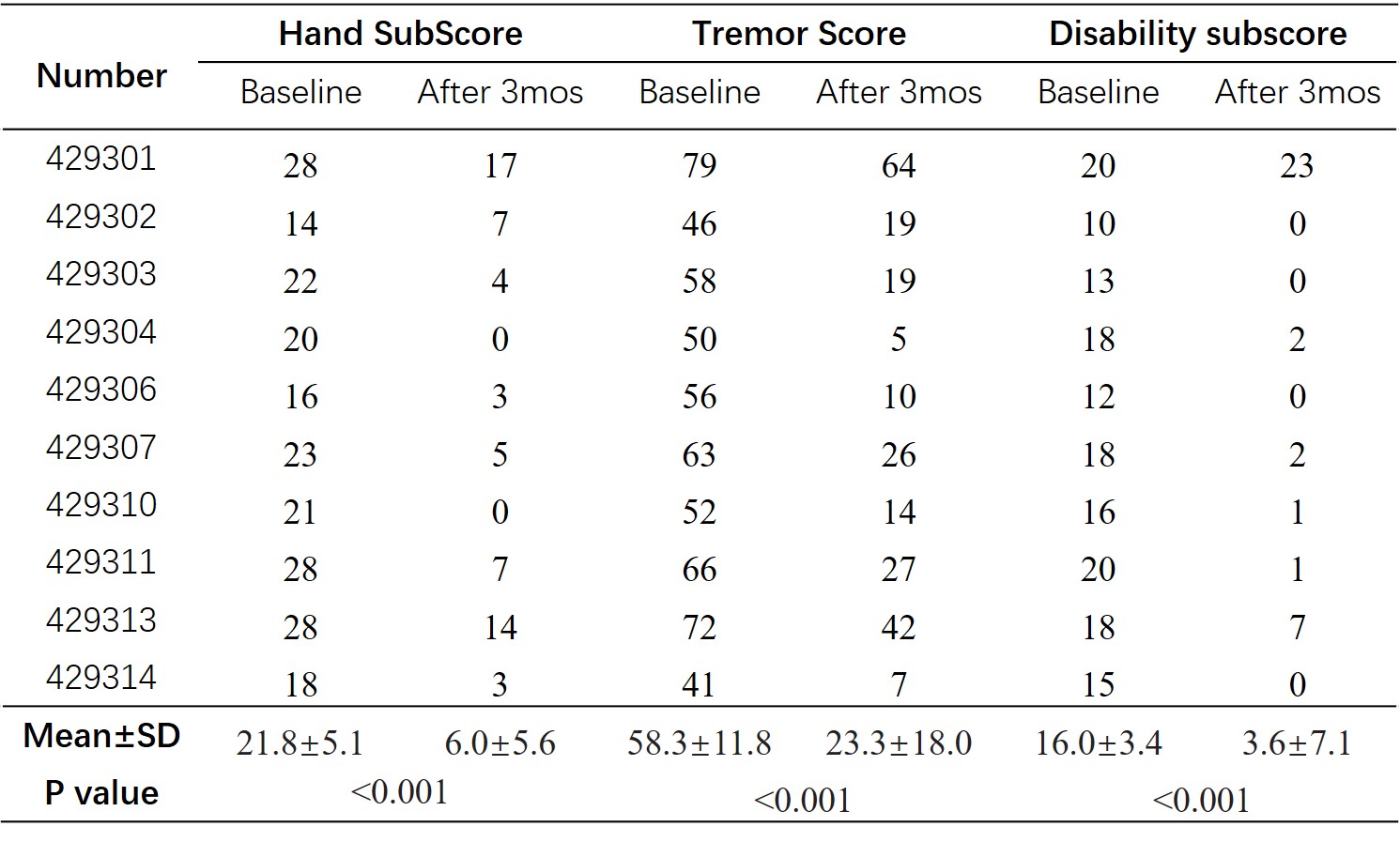
From January 2019 to April 2019, in an open-label, uncontrolled study, we used transcranial MRgFUS to target the unilateral ventral intermediate nucleus of the thalamus in 10 patients with severe, medication-refractory ET. We recorded all safety data and measured the effectiveness of tremor suppression using the Clinical Rating Scale for Tremor to calculate the total score (ranging from 0 to 160), hand subscore (primary outcome, ranging from 0 to32), and disability subscore (ranging from 0 to 32). Higher scores indicate worse tremor.Results
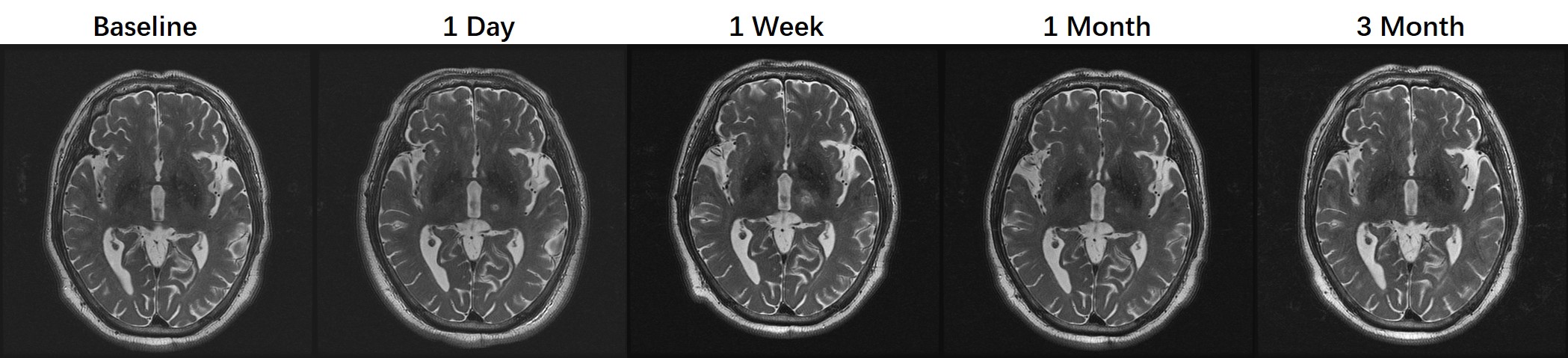
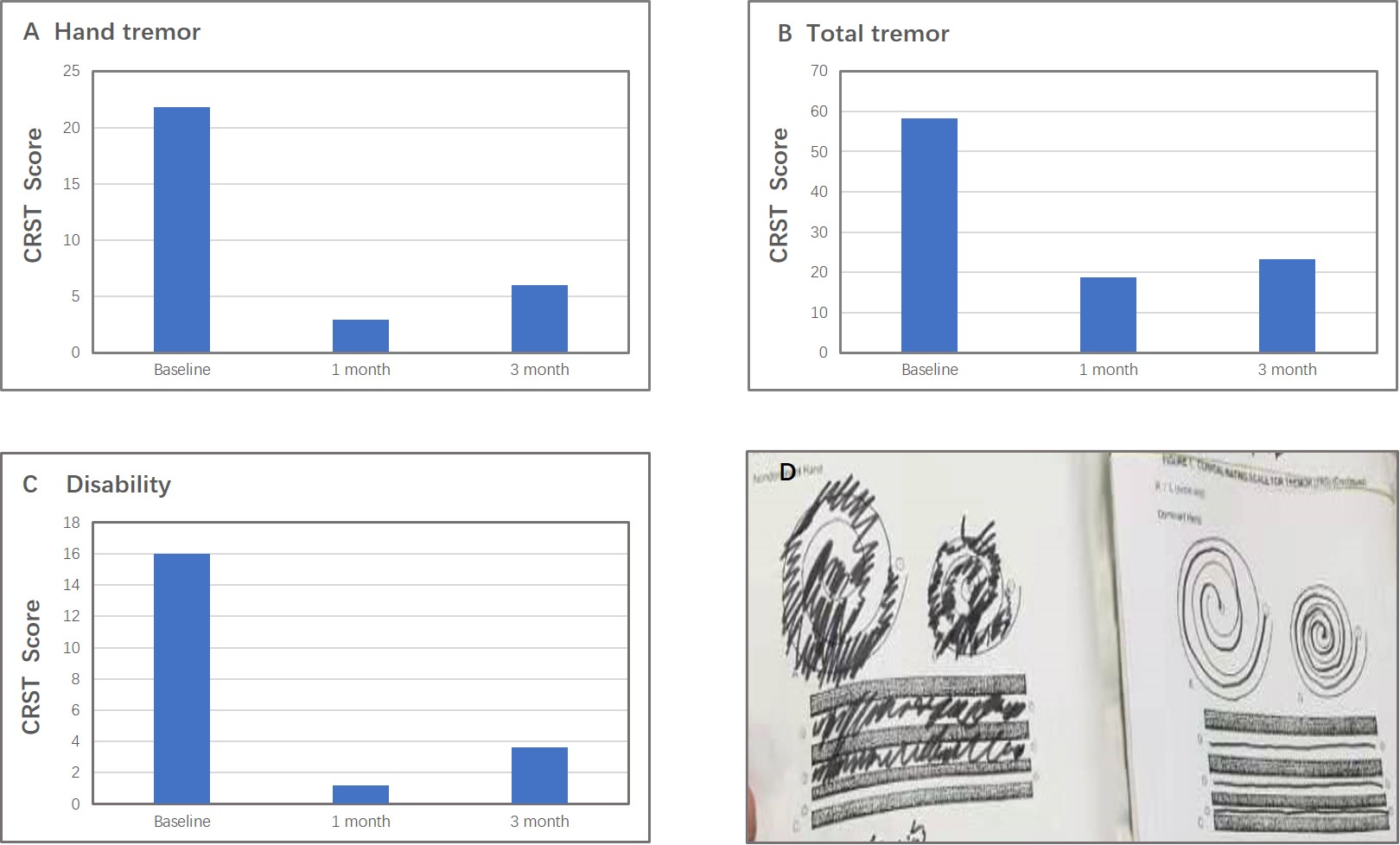
Thermal ablation of the thalamic target took place in all patients (Table 1, Figure 1). Score for hand tremor improved from 21.8±5.1 at baseline to 6.0±5.6 at 3 months (P<0.001). Total tremor score improved from 58.3±11.8 to23.3±18.0 (P<0.001). Disability score improved from 16.0±3.4 to 3.6±7.1 (P<0.001) (Table 2, Figure 2). Adverse events that transiently occurred during sonication included short-lasting vertigo (n=2) and burning scalp sensation (n=2), vomiting (n=2). Adverse events which lasted after the procedure included gait ataxia (n=1), unsteady feeling (n=1), asthenia(n=2), lip paresthesia (n=5). No adverse events lasted beyond 3 months.Discussion
Noninvasive and effective treatment of medication-resistant ET is of great significance to patients4. The results of this study revealed that MR–guided focused ultrasound thalamotomy could provide effective tremor relief with an acceptable profile of adverse effects. The primary limitations of this study were that the sample size was small and lack of a control group.Conclusion
MR–guided focused ultrasound thalamotomy, as a novel, precise and noninvasive treatment to relieve medication-resistant essential tremor is perfectly safe and effective.Acknowledgements
References
[1]Elias WJ, Huss D, Voss T, et al. A pilot study of focused ultrasound thalamotomy for essential tremor. N Engl J Med. 2013. 369(7): 640-8.
[2]Elias WJ, Lipsman N, Ondo WG, et al. A Randomized Trial of Focused Ultrasound Thalamotomy for Essential Tremor. N Engl J Med. 2016. 375(8): 730-9.
[3]Mohammed N, Patra D, Nanda A. A meta-analysis of outcomes and complications of magnetic resonance-guided focused ultrasound in the treatment of essential tremor. Neurosurg Focus. 2018. 44(2): E4.
[4]Haubenberger D, Hallett M. Essential Tremor. N Engl J Med. 2018. 378(19): 1802-1810.
Figures