1524
Multi-modality evaluation of Hyposmia in patients with Parkinson’s disease and atypical Parkinsonism
A Ankeeta1, Shefali Chaudhary1, S Senthil Kumaran1, Priyanka Bhat2, and Vinay Goyal2
1NMR and MRI facility, All India Institute of Medical Sciences, New Delhi, India, 2Neurology, All India Institute of Medical Sciences, New Delhi, India
1NMR and MRI facility, All India Institute of Medical Sciences, New Delhi, India, 2Neurology, All India Institute of Medical Sciences, New Delhi, India
Synopsis
The pattern of Hyposmia hemodynamic response, functional connectivity and ERP response was investigated in patients with Parkinson's disease, Multiple System Atrophy (MSA) and Progressive Supranuclear Palsy (PSP). Results revealed the presence of significant olfactory loss correlated with differential pattern in the olfactory pathway including frontal region and temporal areas. MRI, BOLD and EEG, can be used to detect early biomarker(s) for the identification of Parkinson and atypical Parkinsonism patients on the basis of hyposmia.
Introduction
Patients with Parkinsonism experience a range of non-motor symptoms during the onset and progress of the disease. Psycho physical and electrophysiological studies have suggested that hyposmia may be a characteristic sign of Parkinson's disease (PD)1,2. Deficits in the sense of smell may precede clinical motor symptoms by years and can be used to assess risk for developing PD in otherwise asymptomatic individuals. Recent data indicate that over 95% of patients with PD present with significant olfactory loss1. We investigated Hyposmia using fMRI and EEG, to identify the extent of olfactory dysfunction on cognition in Parkinsonism.Methodology
Twenty-five right-handed PD, 16 MSA, and 16 PSP patients were recruited from the movement disorder clinic of our institute (Figure 1). Standard diagnostic and exclusion criteria were followed. MR studies were carried out in a 3T MR scanner using 32 channel head coil (M/s. Philips, the Netherlands) in the “on” state. Echo planar imaging sequence was used for the functional MRI studies to study the Blood oxygen level dependent (BOLD) effects in the whole brain. We used a block paradigm design where the patients underwent sniff kit (Burghart Messtechnik GmbH, Germany) test during the active state, and a period of rest (no smell) during the baseline state. Data was analysed using SPM12 and EEG lab3,4. The BOLD activation pattern was overlaid onto the MNI template using the Talairach and Tornoux co-ordinates. two-sample t-test (p<0.001, cluster threshold 10) was used for inter-group comparisons.Results
Patients with Parkinson revealed less BOLD activation than patients with MSA and PSP (Figure 2). Activation was absent in the olfactory regions (middle frontal, orbitofrontal, and temporal cortex and also in inferior frontal, insular, and cingulate cortex) in patients with Parkinson's disease. Activation was observed in bilateral middle frontal and the orbitofrontal cortex, and left hemispheric inferior frontal, temporal, and cingulate cortex areas in patients with MSA and PSP3. The functional connectivity for the seed region amygdala to the olfactory pathway network areas (as target) exhibited a decrease in the frontal and mid brain areas, including the basal ganglia, pons, caudate and medulla oblongata (Figure 3) . The gray matter concentration in the olfactory bulb and the basal ganglia is reduced and white matter concentration was also disrupted in the primary motor area and cerebellum regions (Figure 4). A similar pattern was observed on the frequency change of Delta waveform of the EEG in PD and MSA groups, but the PSP exhibited a different pattern in the alpha waveform (Figure 5). An increase of spectral powers in the “slow” frequency bands <8 Hz (delta and theta) and a decrease in the “fast” frequency bands >8 Hz (alpha, beta, and, less significantly, gamma) was observed in PD and MSA patients, and different in PSP group.Discussion
The clinical (H and Y score, UPDRS-III and the MMSE/MOCA scores) and hemodynamic response did not reveal any significant correlation, and can be attributed to the absence of structural alterations of the olfactory bulb with the progression of the disease. EEG exhibited different spectral power of delta and alpha waves and a positive correlation with the clinical score in the frontal cortex suggesting the transmission of olfactory signals to temporal and cingulate regions (Figure 6).We observed decreased BOLD activation in amygdala and thalamus region of PD patients in the right hemisphere for the discrimination and identification of olfactory processing in the order PD>MSA >PSP suggesting alterations in the processing of emotional stimuli5. A decrease in the ventral striatum, prefrontal areas and orbitofrontal cortex (OFC) regions in PD and MSA patients (but not in PSP group) suggests the dependency of these dopaminergic areas on the hedonic value of the odour6. The global olfactory bulb volume correlated inversely with PD duration. Decreased connectivity between amygdala to inferior parietal lobule, lingual gyrus, fusiform gyrus, and superior/middle temporal gyrus was observed in PD than MSA and PSP groups, and reduction of gray matter volume in the olfactory bulb of PD patients (in comparison with that of MSA and controls) may be attributed to the difficulties in identification of the odour in Parkinson patients7.
Conclusion
Alteration in structural, connectivity and EEG changes associated with the hyposmia suggests that olfactory loss can be used as distinct markers and may help in the assessment of disease progression.Acknowledgements
We thank Department of Science and Technology, Government of India for funding the study.References
- Iannilli E Stephan L, Hummel T, Reichmann H, Haehner A. (2017). Olfactory impairment in Parkinson's disease is a consequence of central nervous system decline. J Neurol. 264:1236-1246
- Haehner A, Hummel T, Reichmann H. (2009). Olfactory dysfunction as a diagnostic marker for Parkinson's disease. Expert Rev Neurother. 912:1773-9
- Friston KJ (2003). Learning and inference in the brain. Neural Netw.16:1325–52
- Delorme A, Makeig S (2004). EEGLAB: an open source toolbox for analysis of single-trial EEG dynamics. Journal of Neuroscience Methods. 134:9-21.
- Yoshimura N, Kawamura M, Masaoka Y, Homma I (2005). The amygdala of patients with Parkinson's disease is silent in response to fearful facial expressions. Neuroscience 131, 523–534.
- Royet JP, Zald D, Versace R, et al.,. (2000). Emotional responses to pleasant and unpleasant olfactory, visual, and auditory stimuli: a positron emission tomography study. J. Neurosci. 20, 7752–7759
- Savic I, Gulyas B, Larsson M, Roland P (2000). Olfactory functions are mediated by parallel and hierarchical processing. Neuron 26, 735–745
Figures
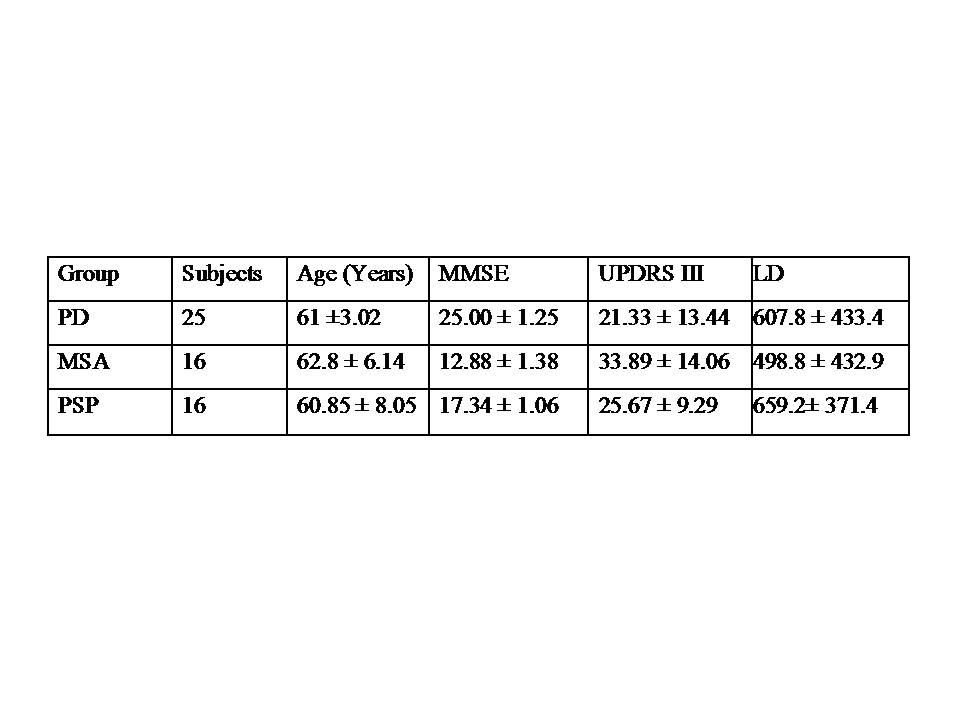
Figure 1. Demographic detail of subjects
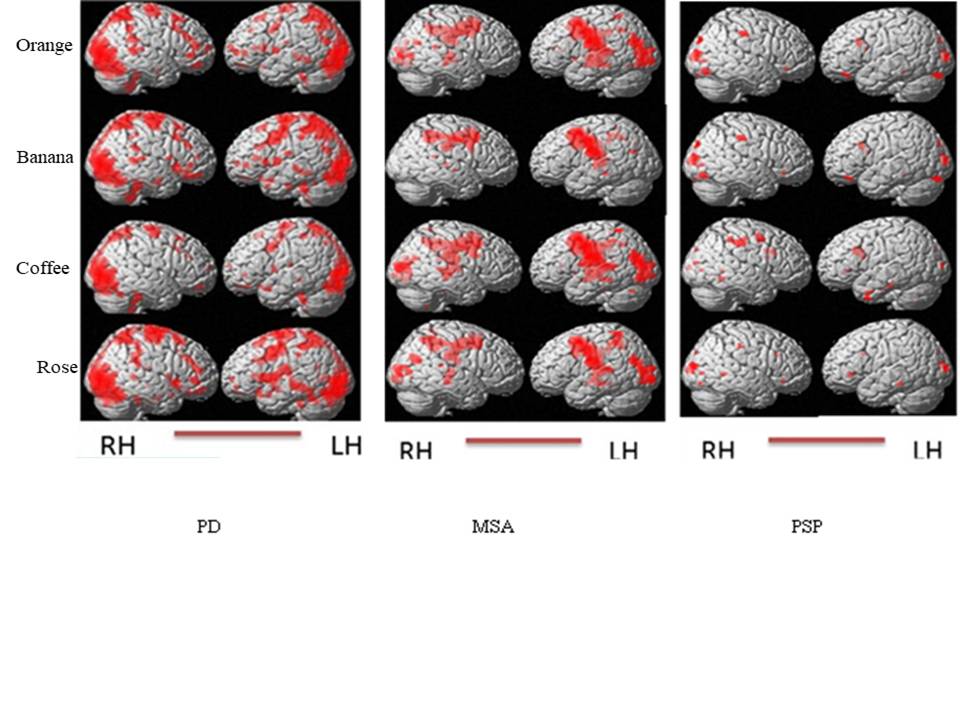
Figure 2. Group level differences
for the BOLD response for the smell (coffee, banana, orange, and rose) stimulation of sniff kit during MRI scanning in PD, MSA and PSP patients (rendered on whole brain images, two-sample t-test, p<0.001 unc, voxel threshold 10).
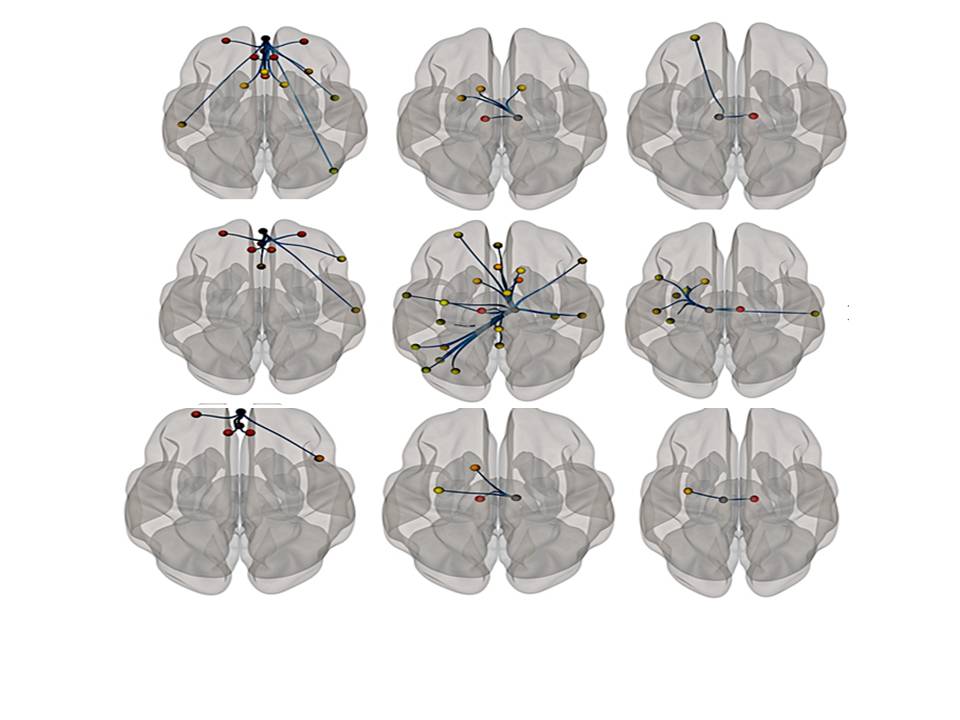
Figure 3. Group level differences
for the functional connectivity during MRI scanning in PD, PSP and MSA
patients (using CONN, p<0.001 unc).
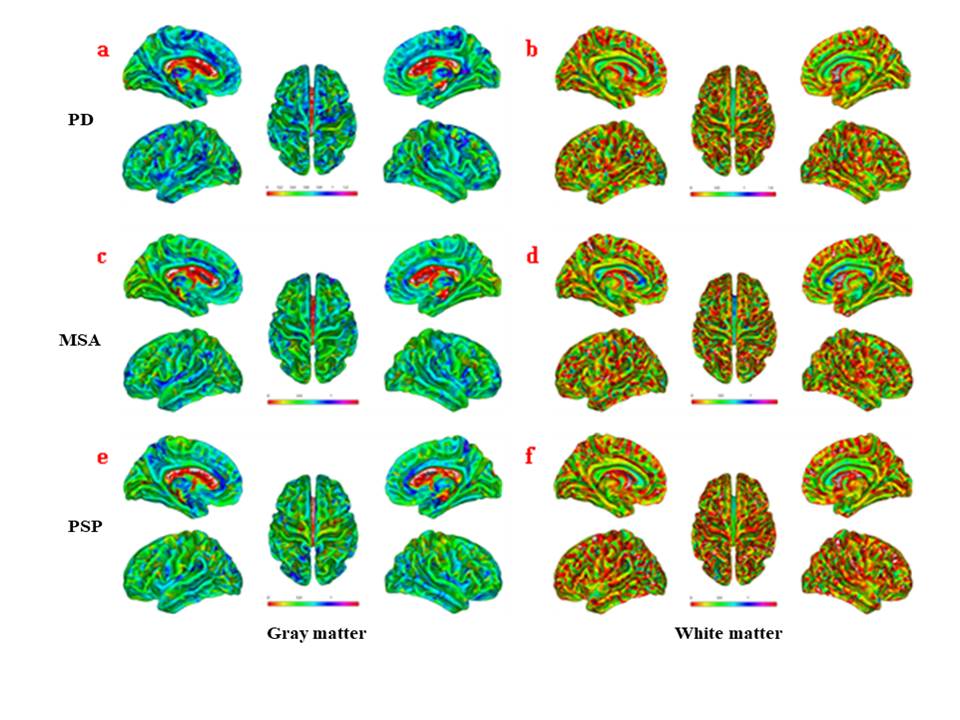
Figure 4. Group level differences of the gray and white matter, estimated using volumetric analysis in anatomical regions associated with olfactory disorder in PD, MSA and PSP patients (using CAT12).
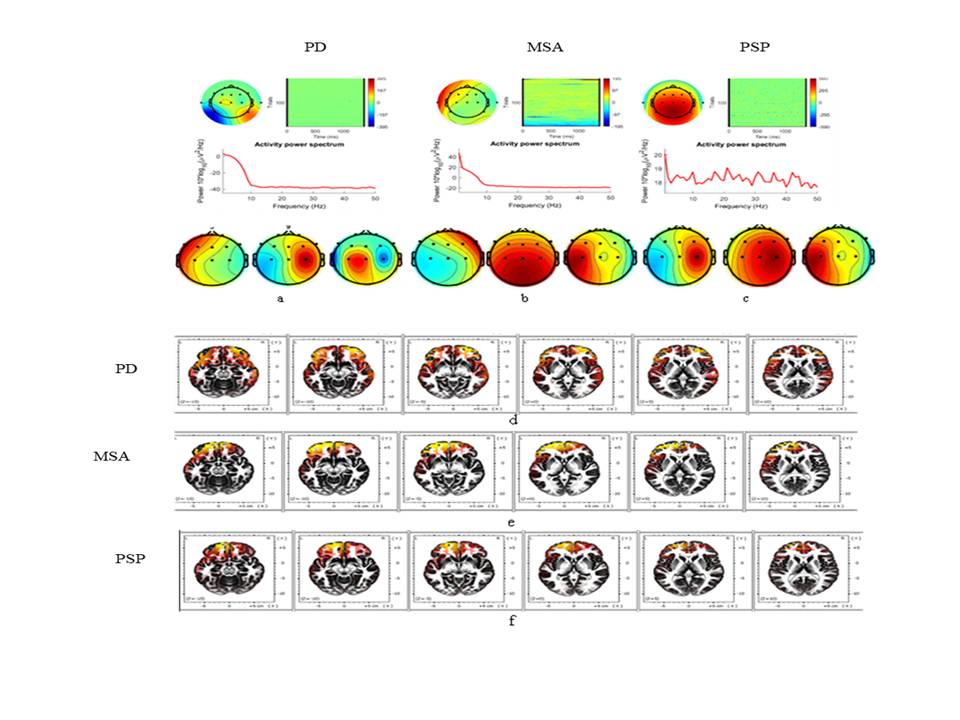
Figure 5. Group level differences
for the EEG and ERP during the presentation of smell (Sniff kit) in
PD, MSA and PSP patients.
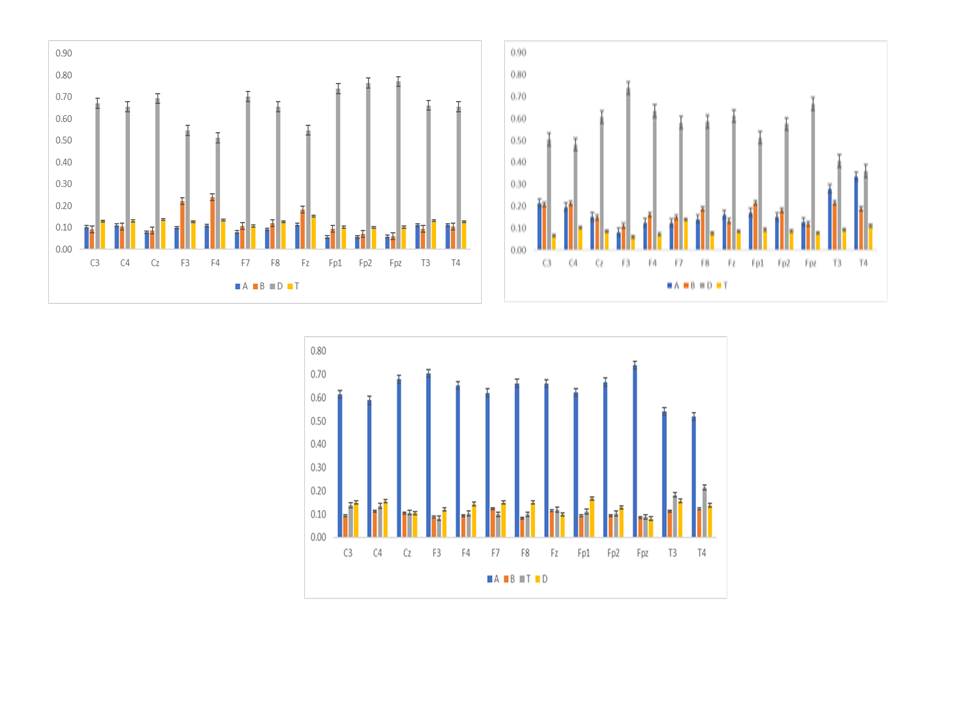
Figure 6. Correlation between cluster count of BOLD activation and the EEG
frequencies in (A) PD, (B) PSP, and (C) MSA patients.