1475
Distinct fibre-specific white matter reductions pattern in early- and late-onset patients1Radiology, The 2nd Affiliated Hospital of Zhejiang University, School of Medicine, Hangzhou, China, 2MR Research, GE Healthcare, Shanghai, China
Synopsis
For the first time, we applied fixel-based analysis (FBA) to investigate fibre tract-specific WM changes in early-onset Alzheimer’s disease (EOAD) and late-onset AD (LOAD). To test the repeatability of the results, we repeated the analysis in two independent cohort. We demonstrated that EOAD in two cohorts had more widespread WM tracts loss than LOAD. The different FD extended from the limbic system to long posterior projection regions. Further, we found that FD, rather than FC, had a higher sensitivity in detecting WM loss of EOAD, and vice versa in LOAD. Results may provide clinical clues for early diagnosis of EOAD.
INTRODUCTION
Early-onset Alzheimer’s disease (EOAD) has different pathological and neuropsychological features from late-onset AD (LOAD). At a similar stage, patients with EOAD have severer and wider cognitive dysfunction, which may contribute to the differences of cerebral structural damage between AD patients. Specifically, EOAD associated with higher amyloid burden than LOAD in parietal and lateral temporal regions. In addition, EOAD had tau retention throughout the neocortex while LOAD had restricted pathologies in medial temporal lobe. Based on diffusion tensor imaging (DTI), previous studies demonstrated that LOAD had altered diffusion properties in the posterior cingulum and temporal lobe (memory-related regions), while EOAD had more widespread impairment involving posterior association areas and fronto-parietal networks. The fixel-based analysis (FBA) metrics, including the fibre density (FD) and fibre cross-section (FC), represent the micro- and macrostructural properties of fibre bundle respectively. In addition, it provides a comprehensive indicator of FD and FC, namely FDC. Recently, the work of Remika Mito2 demonstrated that FBA could sensitively identify AD from the control group, and results are more advantageous in biological interpretation.In the current study, we aims to investigate the pathogenesis of EOAD and LOAD from the perspective of the white matter structure using FBA. The main objective was threefold: (1) to assess the fixel-based WM loss in patients with EOAD and LOAD, at both the fixel and tract-specific level; (2) to assess the relationship between fixel-based measures and cognitive performance/neuropathologies in subgroup level; (3) to evaluate the reproducibility of FBA, we repeated the analysis in two completely independent database. Further, we repeated our analysis using the commonly used tract-based spatial statistical (TBSS) methods. Considering the distinct cognitive picture and pathologies distribution, we thus hypothesized that LOAD patients would show a preferential WM loss connecting to the medial temporal regions, while EOAD patients would have a more widespread WM impairment connecting with parietotemporal regions. Further, due to the increased ability to display the intersection of the fibers, we hypothesized that we may observed altered fiber integrity extending beyond tracts known to be affected in EOAD.
METHOD
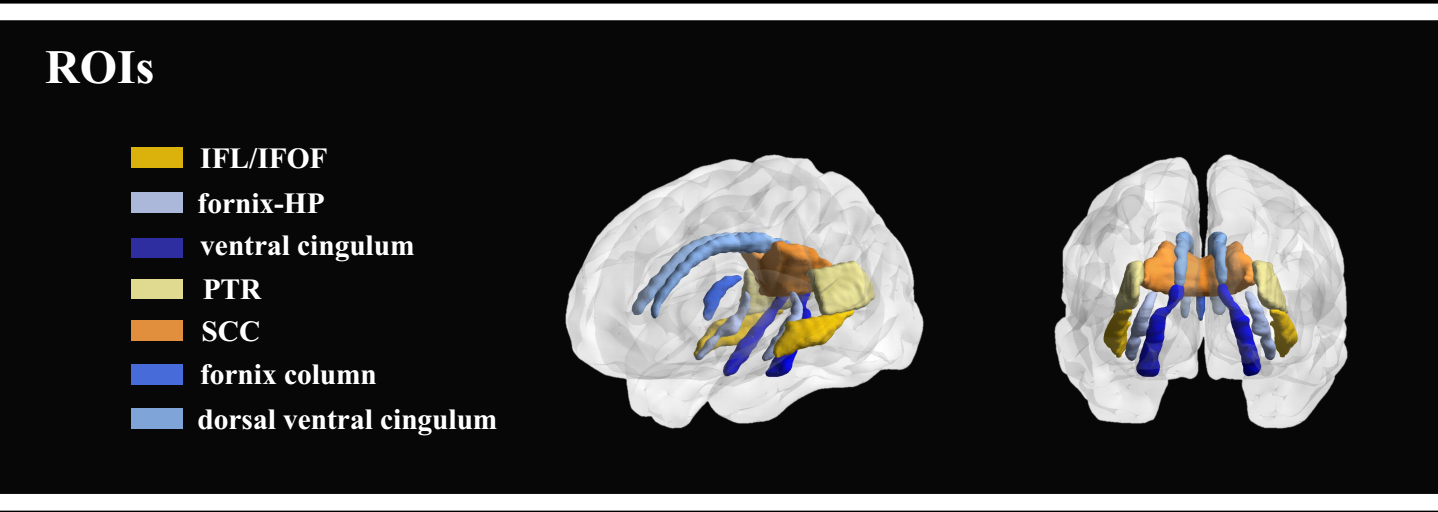
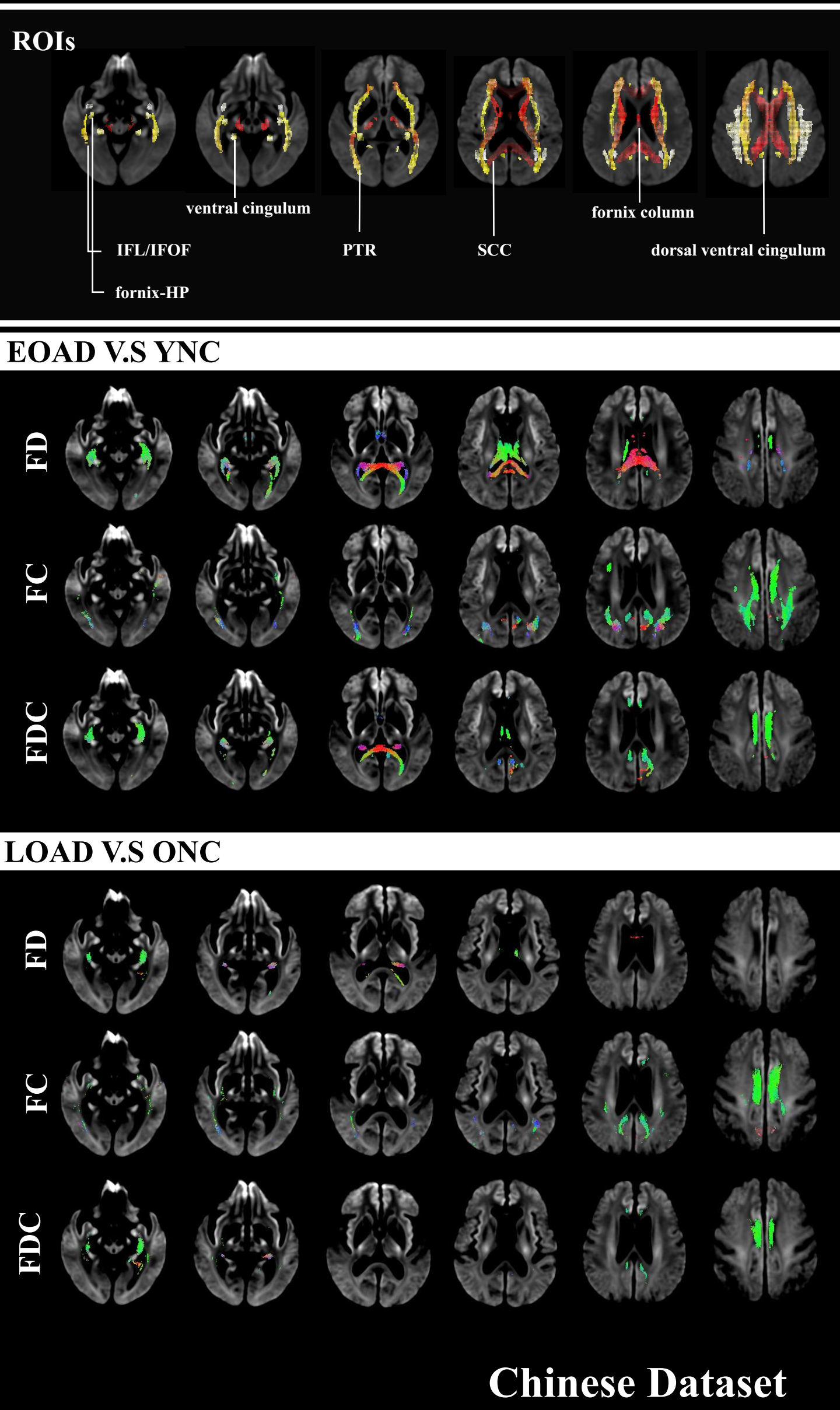
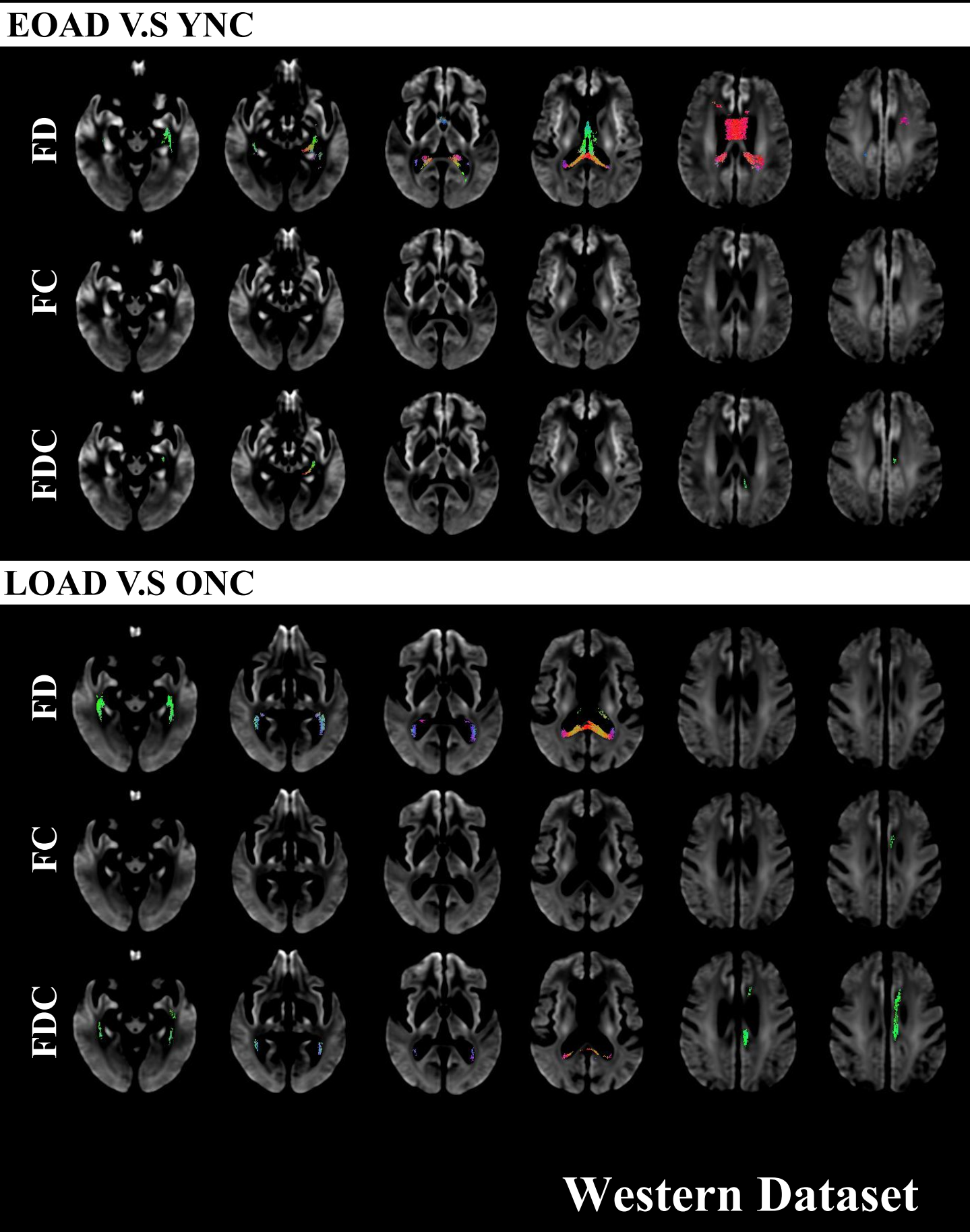
We included 31 EOAD, 45 LOAD, 64 young healthy controls (YHC), and 46 older HC (OHC) based on Chinese population. Also, we identified 17 EOAD, 30 LOAD, 31 YHC, and 34 OHC from ADNI database. Each subject underwent T1 weighted, diffusion MRI imaging, and comprehensive neuropsychological assessment. Some subjects from ADNI undergone amyloid and tau PET scanning. Based on fixel-based analysis (FBA), we measured the axonal degeneration of each fibre direction using the fiber density (FD), fiber bundle cross-section (FC), and bundle cross-section (FDC) metrics. We also performed tract-specific analyses across 12 selected WM tracts3,4, to investigate degeneration within fiber pathways (Figure 1). To test the repeatability of the results, we repeated the analysis in two independent cohort. Further, we correlated the fiber metrics with neuropathologies and cognitive performance.RESULTS
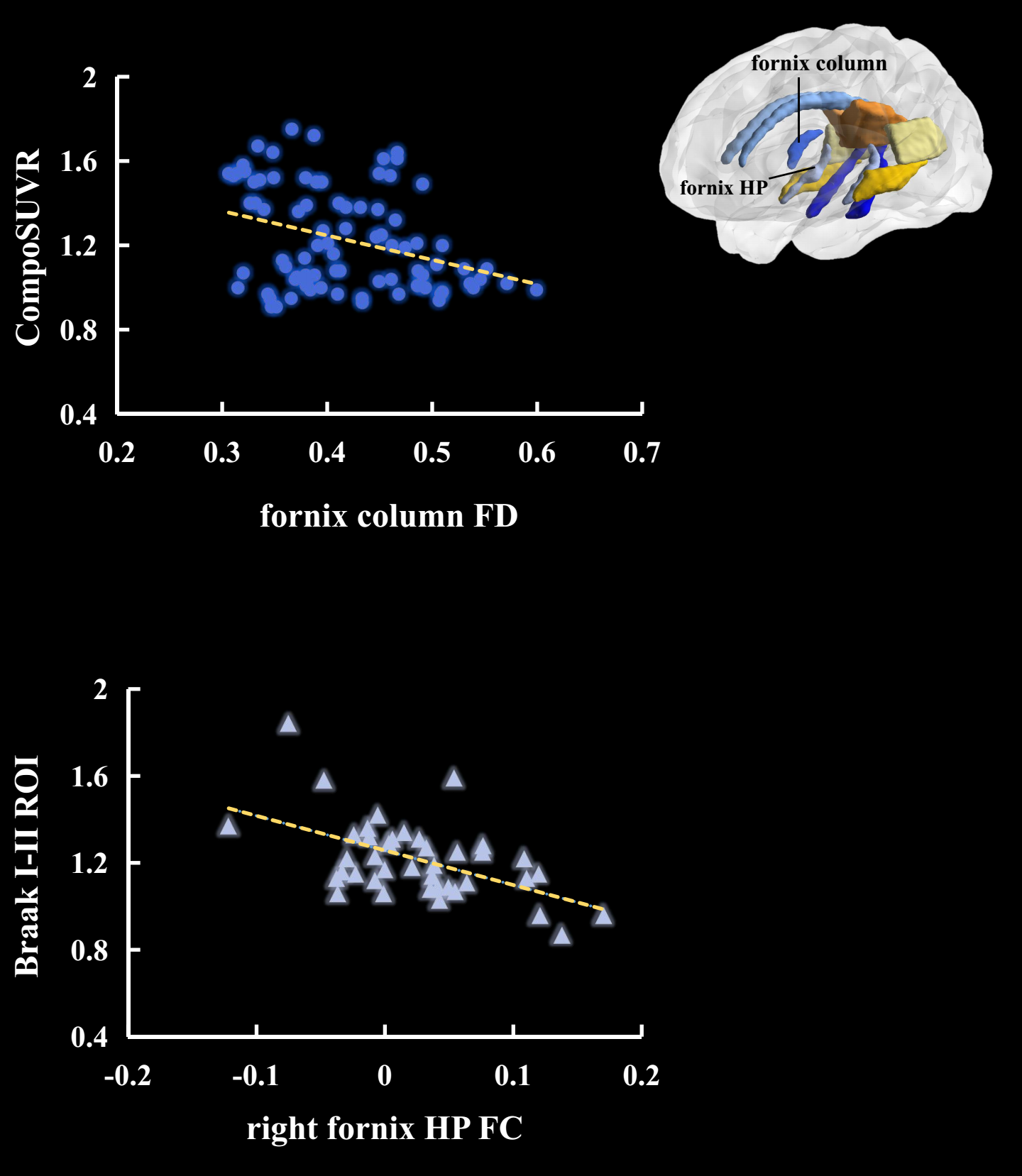
In fixel-wise level, results from two independent cohort had the same trend (p<0.05, FWE corrected). Specifically, LOAD had restricted WM loss than OHC, mainly involving bilateral dorsal and ventral cingulum bundle. By contrast, EOAD patients showed a greater damage effects in the commissural and long projection fiber, including fornix column and body, CCS, and PTR, apart from the limbic system-related WM fibers (Figure 2). Interestingly, in the both databases, EOAD patients had more widespread decrease of FD, rather than FC, than YHC, and vice versa in LOAD (Figure 3). However, EOAD and LOAD had comparable FDC decrease. In tract-specific level, results remained largely unchanged. Across groups, subsequent correlation analyses results showed that both the FD and FC metrics correlated well with general cognitive ability and multiple cognitive domains (p<0.05, Bonferroni corrected). Further, across groups in ADNI database (p<0.05, Bonferroni corrected), we found that fornix column FD correlated with composite amyloid deposition SUVR (r=-0.34); and right ventral cingulum FC correlated with Tau retention within Braak I-II ROI (r=-0.53).DISCUSSION & CONCLUSIONS
For the first time, we applied FBA to investigate fibre tract-specific WM changes in patients with EOAD and LOAD. To test the repeatability of the results, we repeated the analysis in two independent cohort. We demonstrated that EOAD in two cohorts had more widespread WM tracts loss than LOAD, especially in microstructural level. The different FD extended from the limbic system to long posterior projection regions. Subsequent correlation analyses results suggested these imaging differences may account for the clinical phenotypes of EOAD and LOAD. Further, we found that FD, rather than FC, had a higher sensitivity in detecting WM loss of EOAD, and vice versa in LOAD in LOAD. Our research may provide clinical clues for the early diagnosis of EOAD.Acknowledgements
Processing was performed using the MRtrix3 package (www.mrtrix.org).References
1. Toyota Y, Ikeda M, Shinagawa S, et al. Comparison of behavioral and psychological symptoms in early‐onset and late‐onset Alzheimer's disease. International Journal of Geriatric Psychiatry: A journal of the psychiatry of late life and allied sciences 2007;22:896-901.
2. Mito R, Raffelt D, Dhollander T, et al. Fibre-specific white matter reductions in Alzheimer’s disease and mild cognitive impairment. Brain 2018;141:888-902.
3. Wakana S, Jiang H, Nagae-Poetscher LM, Van Zijl PC, Mori S. Fiber tract–based atlas of human white matter anatomy. Radiology 2004;230:77-87.6. Mori S, Wakana S, Van Zijl PC, Nagae-Poetscher L. MRI atlas of human white matter: Elsevier, 2005.
4. Mori S, Wakana S, Van Zijl PC, Nagae-Poetscher L. MRI atlas of human white matter: Elsevier, 2005.
Figures