1332
Spiral bSSFP Phase-contrast Flow at 0.55T1National Heart, Lung & Blood Institute, National Institutes of Health, Bethesda, MD, United States
Synopsis
A balanced SSFP (bSSFP) phase-contrast using a spiral readout was implemented for quantitative flow measurements at 0.55T. bSSFP flow is challenging at 1.5T and 3T due to off-resonance. However, at 0.55T, this sequence exploits the improved field inhomogeneity for a long readout (TR = 7.2ms) bSSFP spiral acquisition. This sequence provided improved signal-to-noise ratio (SNR) normalized by voxel, especially during diastole (Cartesian gradient echo SNR/voxel = 3.6, spiral bSSFP SNR/voxel = 9.4), to produce quality flow measurements at 0.55T.
Introduction
Low-field (<1.5T) MRI has been of recent interest for cardiac MR (CMR). Low-field scanners offer the advantages of reduced heating of implants and interventional devices, lower SAR, reduced signal loss from shorter T1 and longer T2*, and potential lower costs. We recently described a commercial MRI system modified to operate at 0.55T, retaining high-performance contemporary hardware, which is well-suited for technically-demanding CMR1.For phase contrast flow measurements, the low SNR of gradient-echo acquisitions during diastole can potentially limit the measurement of slow-flowing regurgitant volume. Balanced steady-state free precession (bSSFP) phase-contrast flow measurements have been previously proposed to improved SNR2,3, but can be challenging at 1.5T and 3T due to off resonance.
At 0.55T, we implemented a bSSFP phase-contrast sequence using a spiral readout. Long spiral readouts are amenable to maintain image quality and SNR, whilst exploiting the reduced SSFP-banding and image blurring due to the improved field homogeneity at lower fields.
Methods
Institutional review board approval and informed consent was obtained for imaging studies. Healthy volunteers (n=11) were imaged at 0.55T (prototype MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). Phase-contrast flow was measured through the ascending aorta and main pulmonary artery using free-breathing gradient-echo (GRE) Cartesian and bSSFP spiral imaging.A uniform-density, 60-shot, spiral-out design with zeroth and first-moment gradient balancing was implemented (TE/TR = 1.6/7.2 ms, flip angle = 70°, 1.4 x 1.4 mm2 resolution, 6 mm slice thickness, venc = 150 cm/s, total acquisition time ~2min). Spiral arms were rotated by the golden angle throughout the acquisition.
For comparison, gradient-recalled echo (GRE) Cartesian flow data was matched in acquisition time, slice position and venc (1.8 x 1.8 mm2 resolution, TE/TR = 4.6/7.3 ms, flip angle = 30°, 3 averages, acceleration factor 2, venc = 150 cm/s, total acquisition time ~2 min).
Data was retrospectively binned using the recorded ECG to thirty cardiac frames with a mean temporal resolution of 32.9 ± 5.4 ms. Spiral images were reconstructed using iterative conjugate gradient SENSE and Cartesian images were reconstructed with GRAPPA.
Cardiac output estimated from both the aorta and main pulmonary artery were compared for spiral and Cartesian imaging. SNR was calculated by performing 100 pseudo-replicas 4 on the magnitude images at peak-systole and in diastole, and normalized by voxel volume for direct comparison.
Results
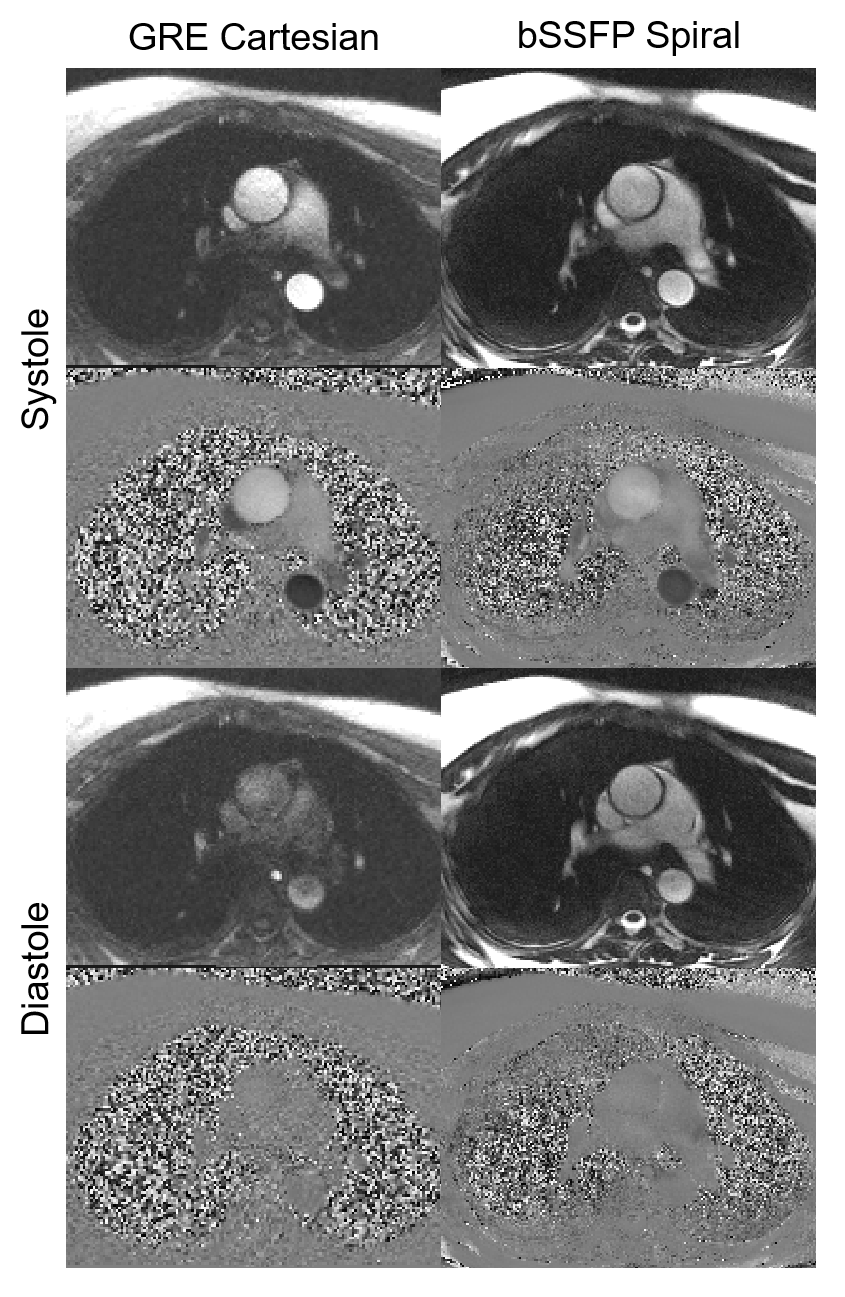
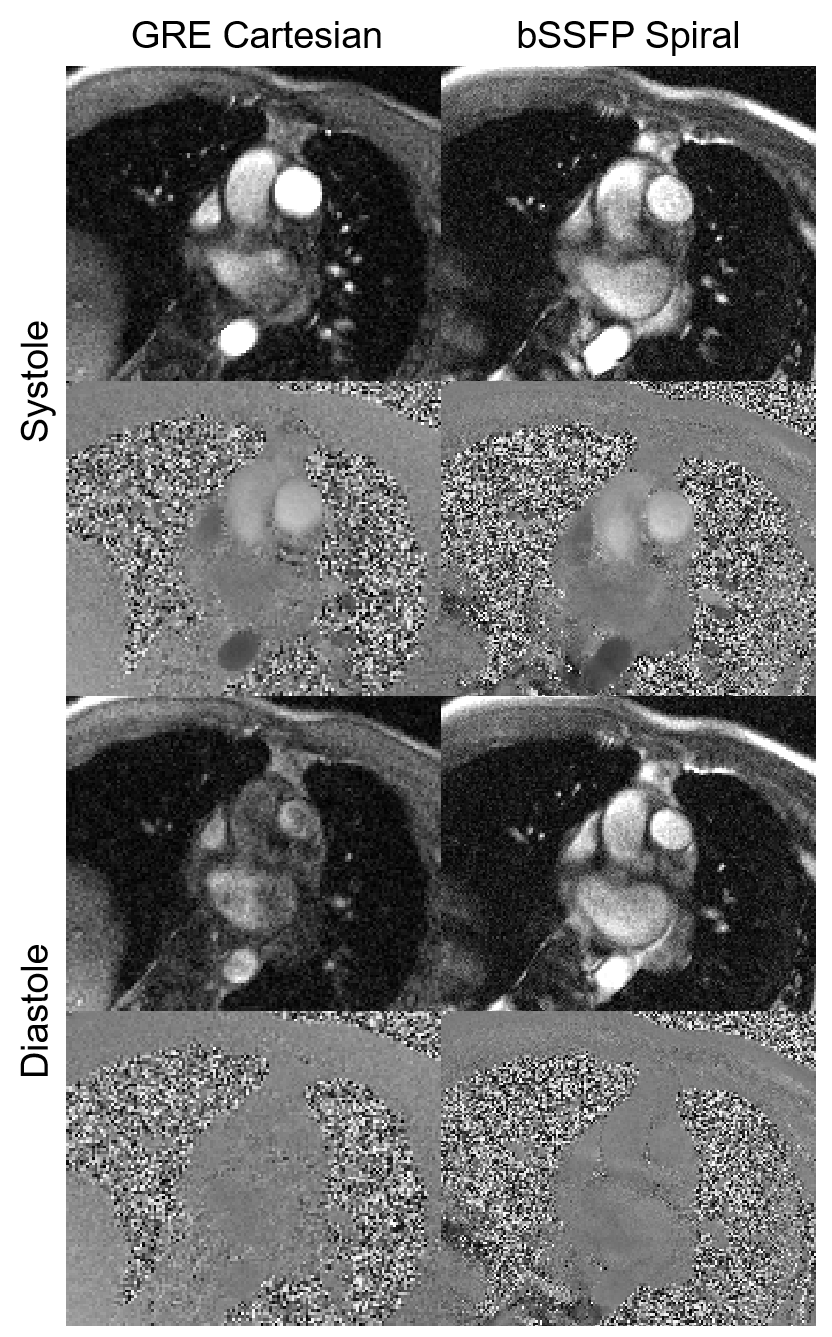
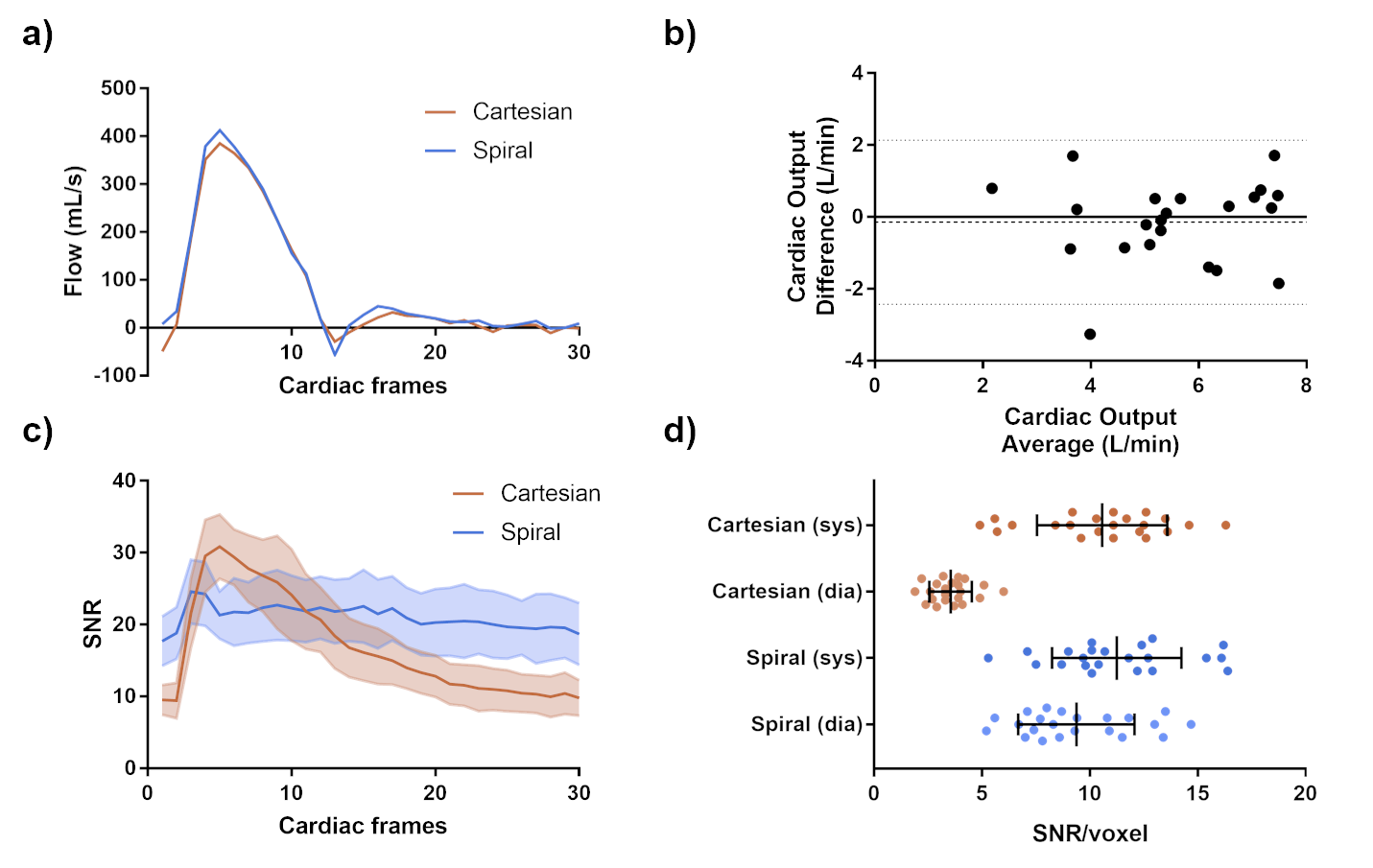
Phase-contrast spiral bSSFP yielded high-quality images (Figures 1 & 2) and flow curves (Figure 3a). Estimates of cardiac output had a small bias (-0.15 L/min) but a poor correlation (0.54) (Figure 3b), compared to the reference GRE Cartesian. The reference GRE acquisition had higher SNR/voxel in systole (10.6 ± 3.0) due to inflow but reduced during diastole (3.6 ± 1.0). However, the bSSFP spiral acquisition maintained good SNR/voxel during both systole (11.3 ± 3.0) and diastole (9.4 ± 2.7) within the blood vessels (Figure 3c & d).Discussion and Conclusion
This investigation demonstrated that bSSFP phase-contrast can be combined with spiral readouts, exploiting improved field inhomogeneity at low field, and yield improved signal-to-noise over the cardiac cycle and high-quality flow measurements for CMR at 0.55T. In some cases, artifacts due to remote flow through an bSSFP band were observed but did not interfere with the vessel of interest. Further investigation is required to optimize the flow quantification and estimates of cardiac output.Acknowledgements
This work was supported by the NHLBI DIR (Z01-HL006039, Z01-HL005062). We would like to acknowledge the assistance of Siemens Healthcare in the modification of the MRI system for operation at 0.55T under an existing cooperative research agreement between NHLBI and Siemens Healthcare.References
1. Campbell-Washburn, A.E. et al, Opportunities in interventional and diagnostic imaging using high-performance low field MRI. Radiology, 2019; 293: 384-393.
2. Markl M, Alley MT, Pelc NJ. Balanced phase-contrast steady-state free precession (PC-SSFP): a novel technique for velocity encoding by gradient inversion. Magn Reson Med. 2003 May;49(5):945-52.
3. Nielsen JF, Nayak KS. Referenceless phase velocity mapping using balanced SSFP. Magn Reson Med. 2009; 61(5):1096-102.
4. Robson PM, et al. Comprehensive Quantification of Signal-to-Noise Ratio and g-Factor for Image-Based and k-Space-Based Parallel Imaging Reconstructions. Magn Reson Med. 2008; 60(4): 895–907.
Figures