1330
Retrospective camera-based respiratory binning for 4D flow MRI – A comparison with liver navigator and self-gating1Radiology and Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 2MR R&D – Clinical Science, Philips Healthcare, Best, Netherlands, 3Department of Biomedical Engineering, University of Technology, Eindhoven, Netherlands, 4Biomedical Engineering and Physics, Amsterdam UMC, Amsterdam, Netherlands
Synopsis
This study aimed to compare the performance of the novel camera-based respiratory navigation sensor (VitalEye) in retrospective respiratory binned Cartesian 4D flow MRI to conventional liver navigator and self-gating. Analyzed were the cross-correlation of the respiratory signals, peak flow rate error compared to 2D flow and the image quality in terms of edge sharpness of the liver/diaphragm border and signal-to-noise ratio. The novel camera-based respiratory navigation sensor VitalEye performed as good as conventional liver navigator and self-gating. Respiratory signal, flow rate error, and image quality showed no significant difference, but VitalEye has the advantage of a 10-times higher sampling frequency.
Introduction
Respiratory correction is important in cardiac MRI to avoid blurring and motion artifacts. Several techniques have been implemented, mainly by restricting the acquisition to the same short time window during the end-expiratory phase. Recently, a novel contact-less camera-based respiratory navigation sensor has been introduced1 and shown improved image quality in abdominal MRI compared to respiratory belt-based triggering2. This may also apply to 4D flow MRI in which the recommended method is a liver/diaphragm MR navigator3 or self-gating4.This study aimed to compare the performance of the novel camera-based respiratory navigation sensor (VitalEye) in retrospective respiratory binned Cartesian 4D flow MRI to conventional liver navigator (RNAV) and self-gating (SG).
Methods
Pseudo-spiral compressed sensing (CS) accelerated 4D flow MRI5,6 of the heart or the aorta were scanned in Ntotal=14 subjects on a 3T MR system (Philips Ingenia ElitionX; Philips Medical Systems, Best, The Netherlands) which was equipped with a built-in-the-bore camera of type IDS uEye (IDS, Obersulm, Germany). The subject cohort Ntotal was divided into four sub-groups N1A=14, N1B=7, N2=6, and N3=6 depending on the performed scan-exam and analysis used. The scanner software was modified to both continuously sample the k-space in a pseudo-spiral Cartesian fashion, which also enabled SG due to repetitive k-space center sampling (k0/0), and to acquire the RNAV with a predefined frequency without ECG-synchronization, which led to different RNAV sample points over the cardiac cycle. 4D flow parameters: TE/TR/flip angle= 2.1ms/3.9ms/8°, spatial resolution= 2.5x2.5x2.5mm3, cardiac frames= 30, VENC= 150cm/s, scan time= 5:18min (aorta) or 6:58min (heart). 4D flow scans of the heart were acquired two times, one with RNAV sampling (4D flow[1]RNAV/VitalEye) and one without (4D flow[2]VitalEye), but always with VitalEye. As a reference, 2D flow scans were acquired at three ROI in the ascending aorta (AAo) and two in the descending aorta (DAo1, DAo2).4D flow data were processed offline using ReconFrame (Gyrotools, Zurich, Switzerland) in MATLAB (The MathWorks Inc., Natick, MA, USA) together with the Berkeley Advanced Reconstruction Toolbox7 (BART) for CS reconstruction with a sparsifying total variation transform in time. The SG signal was extracted in four steps8: Fourier transforms of k0/0 along the readout direction, singular value decomposition per coil, bandpass filtering, and coil clustering. Each respiratory signal was extracted from the raw data. VitalEye was sampled with a frequency of $$$f$$$VitalEye=20.0 Hz, RNAV with $$$f$$$RNAV=2.0 Hz, and SG with $$$f$$$SG=2.3±0.2 Hz. After phase-binning with expiratory-phase defined by a 60% acceptance rate, the final undersampling/acceleration was R = 9.26±0.02 (aorta) to 10.45±0.01 (heart).
Three different analyses were performed in MATLAB to compare the respiratory navigation performance:
- Cross-correlation between VitalEye vs RNAV (N1A =14) and VitalEye vs RNAV vs SG (N1B =7). Cross-correlation $$$C$$$ of two respiratory signals or their phases $$$g$$$ and $$$h$$$ with delay $$$\tau$$$ is defined: $$C = (g\star h)(\tau)=\int_{-\infty}^{\infty} \overline{g(t)}h(t+\tau) dt$$
- Peak flow rate difference between 4D flowRNAV/VitalEye/SG vs 2D flow MRI (N2=6) in three ROI in the form of Bland-Altman and correlation plots. All flow analyses were done with Segment9.
- Image quality based on the signal-to-noise ratio $$$SNR=\frac{\overline{S}}{\sigma_{N}}$$$ as well as the diaphragm sharpness $$$S$$$ defined by a sigmoid fit width over a line profile. Analyzed were two heart scans 4D flow[1]RNAV/VitalEye binned with either RNAV or VitalEye signal, and a 4D flow[2]VitalEye binned with VitalEye signal to investigate if the RNAV sampling introduces image distortions (N2=6).
Results
The results of the cross-correlation (Figure 1), the peak flow rate difference (Figure 2) as well as the image quality measurements (Figure 3) are listed in Tables 1.1-1.3 (Figure 4). It can be seen that RNAV and VitalEye show a high correlation, especially for the respiratory phase or the eventual binning, respectively, are almost identical to $$$C$$$PhaseRNAV/VitalEye=0.97±0.01. A moderate correlation can be seen when comparing SG to VitalEye or RNAV of $$$C$$$PhaseRNAV/SG=0.85±0.03 and $$$C$$$PhaseVitalEye/SG=0.85±0.03. The peak flow rate comparison to 2D flow MRI showed the least error for 4D flowVitalEye of 6.1% followed by 4D flowRNAV of 6.7% and 4D flowSG of 6.8%. The image quality measurements showed equal $$$SNR$$$ and $$$S$$$ values.Discussion
The comparison between the three respiratory signals revealed that there is no significant difference in terms of respiratory signal monitoring, flow rate error, and image quality. However, each technique has its (dis-)advantages. The major advantage for the RNAV is that the signal is a displacement measurement in millimeter in contrast to VitalEye and SG, which signal units are arbitrary. Therefore, the RNAV binning might improve if absolute binning is used instead of phase binning as in this study. The major advantage of VitalEye is the high sampling frequency of 20.0 Hz, which allows sampling of any occurring respiration rate with Nyquist frequency – even those for infants of up to 1.5 Hz. Additionally, the external setup does not change or interfere with the MRI sequence. In contrast, scan time is sacrificed for RNAV or the sampling pattern needs to be adopted for SG.Conclusion
The novel camera-based respiratory navigation sensor (VitalEye) performed as good as conventional liver navigator and self-gating in retrospective respiratory binned Cartesian 4D flow MRI. Respiratory signal, flow rate error, and image quality showed no significant difference, but VitalEye has the advantage of a 10-times higher sampling frequency.Acknowledgements
This work has been supported by the Netherlands Organization for Scientific Research – NWO (HTSM2014).
We thank Martin Bührer for his quick replies and technical assistance whenever needed.
References
- Kruger MG, Springer RPW, Kersten GM, Bril RJ. Towards Contact-less Vital Sign Monitoring using a COTS Resource-Constrained Multi-Core System-an Experience report. In: 2019 IEEE 22nd International Symposium on Real-Time Distributed Computing (ISORC). ; 2019:77-78.
- Harder F, Lohöfer FK, Kaissis GA, et al. Camera-based respiratory triggering improves the image quality of 3D magnetic resonance cholangiopancreatography. Eur J Radiol. 2019. doi:10.1016/j.ejrad.2019.108675
- Dyverfeldt P, Bissell M, Barker AJ, et al. 4D flow cardiovascular magnetic resonance consensus statement. J Cardiovasc Magn Reson. 2015:1-19. doi:10.1186/s12968-015-0174-5
- Uribe S, Beerbaum P, Sørensen TS, Rasmusson A, Razavi R, Schaeffter T. Four-dimensional (4D) flow of the whole heart and great vessels using real-time respiratory self-gating. Magn Reson Med. 2009. doi:10.1002/mrm.22090
- Gottwald LM, Peper ES, Zang Q, et al. Compressed Sensing accelerated 4D flow MRI using a pseudo spiral Cartesian sampling technique with random undersampling in time. Proc Intl Soc Mag Reson Med 25. 2017:1263.
- Peper* ES, Gottwald* LM, Zhang Q, et al. Highly accelerated carotid 4D flow MRI using Pseudo-Spiral Cartesian acquisition and a Total Variation constrained Compressed Sensing reconstruction. In: Journal of Cardiovascular Magnetic Resonance. ; 2019:IN PRESS.
- Uecker M, Ong F, Tamir JI, et al. Berkeley Advanced Reconstruction Toolbox. Proc Intl Soc Mag Reson Med. 2015;23(1):2486.
- Walheim J, Dillinger H, Kozerke S. Multipoint 5D flow cardiovascular magnetic resonance - accelerated cardiac- and respiratory-motion resolved mapping of mean and turbulent velocities. J Cardiovasc Magn Reson. 2019;21(1):42. doi:10.1186/s12968-019-0549-0
- Heiberg E, Sjögren J, Ugander M, Carlsson M, Engblom H, Arheden H. Design and validation of Segment - freely available software for cardiovascular image analysis. BMC Med Imaging. 2010. doi:10.1186/1471-2342-10-1
Figures
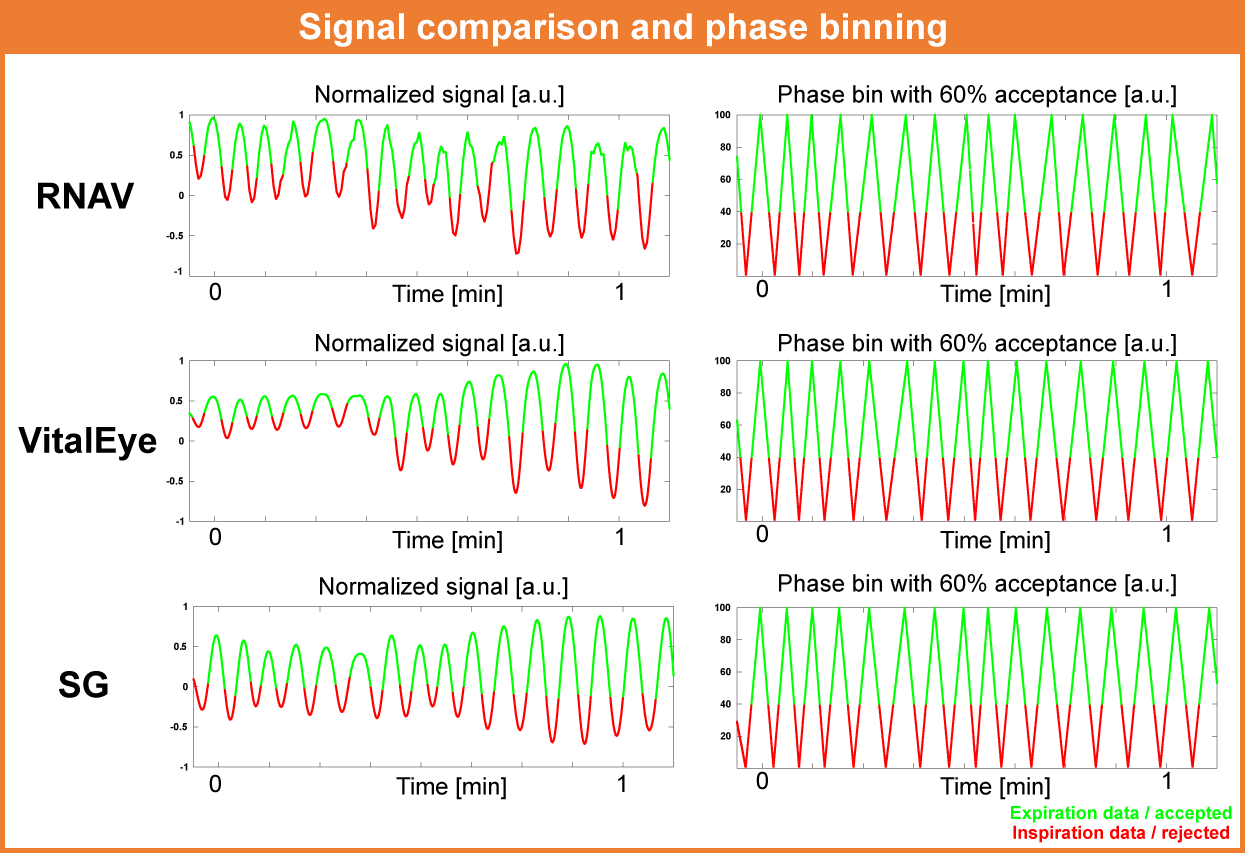
Figure 1:
Signal comparison and corresponding phase-binning of the three different respiratory sensors RNAV, VitalEye, and SG.
The signals have been normalized between -1 and 1, and the phase divided into inspiration (red) and expiration (green).
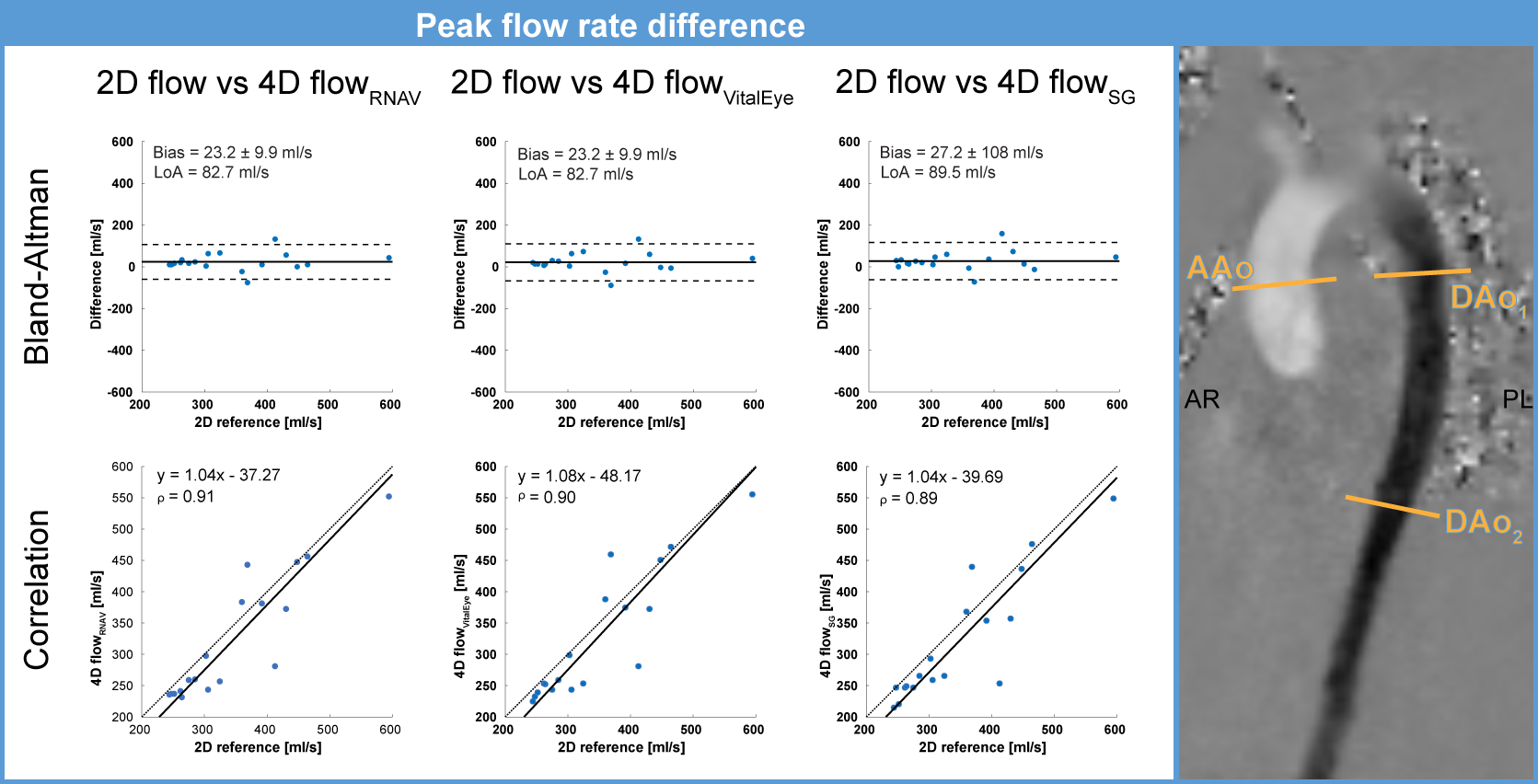
Figure 2:
4D flowRNAV/VitalEye/SG peak flow rate difference to 2D flow MRI at three ROI ascending aorta (AAo) and two descending aorta (DAo1,DAo2) for six aorta scans (N2=6) in the form of Bland-Altman and correlation plots.
The three ROI are indicated on the right.
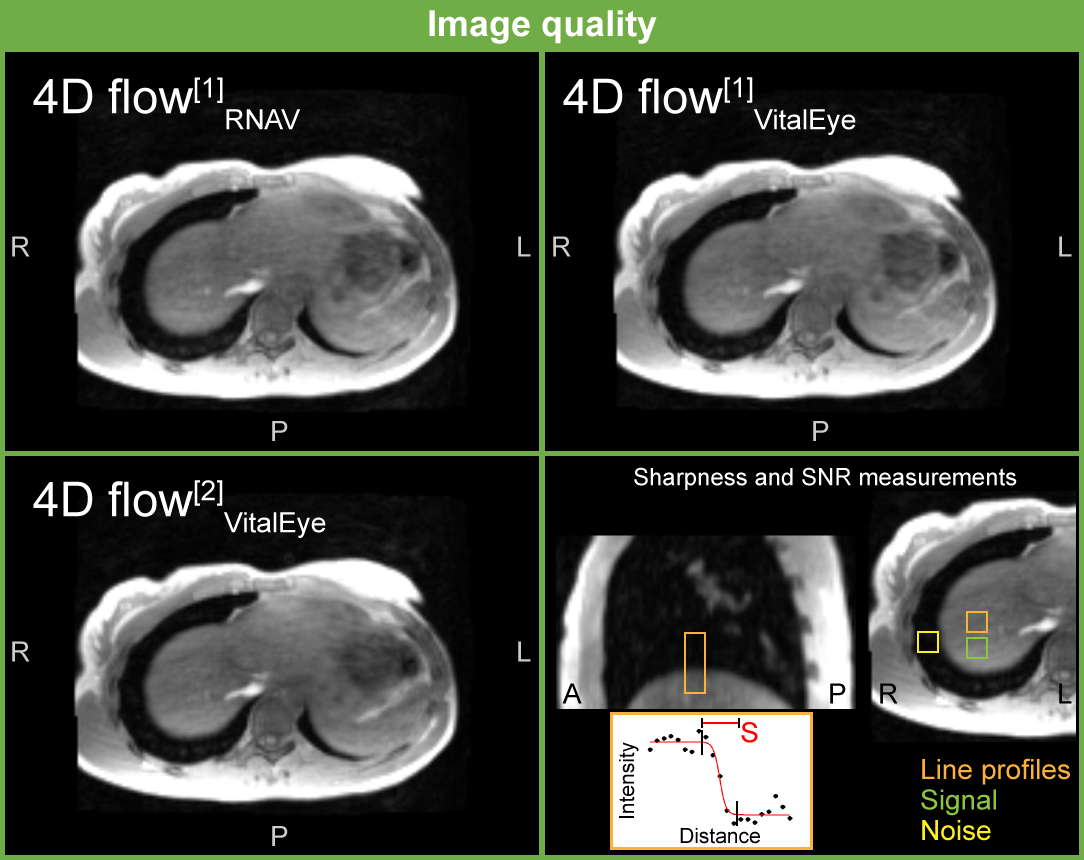
Figure 3:
Image quality comparison of an exemplary 4D flow data set on the liver/diaphragm border. 4D flow scans of the heart were acquired two times, one with RNAV sampling (4D flow[1]RNAV/VitalEye) and one without (4D flow[2]VitalEye).
Moreover, the image quality assessment based on SNR as well as diaphragm sharpness S defined by a sigmoid fit width over a line profile (bottom left).
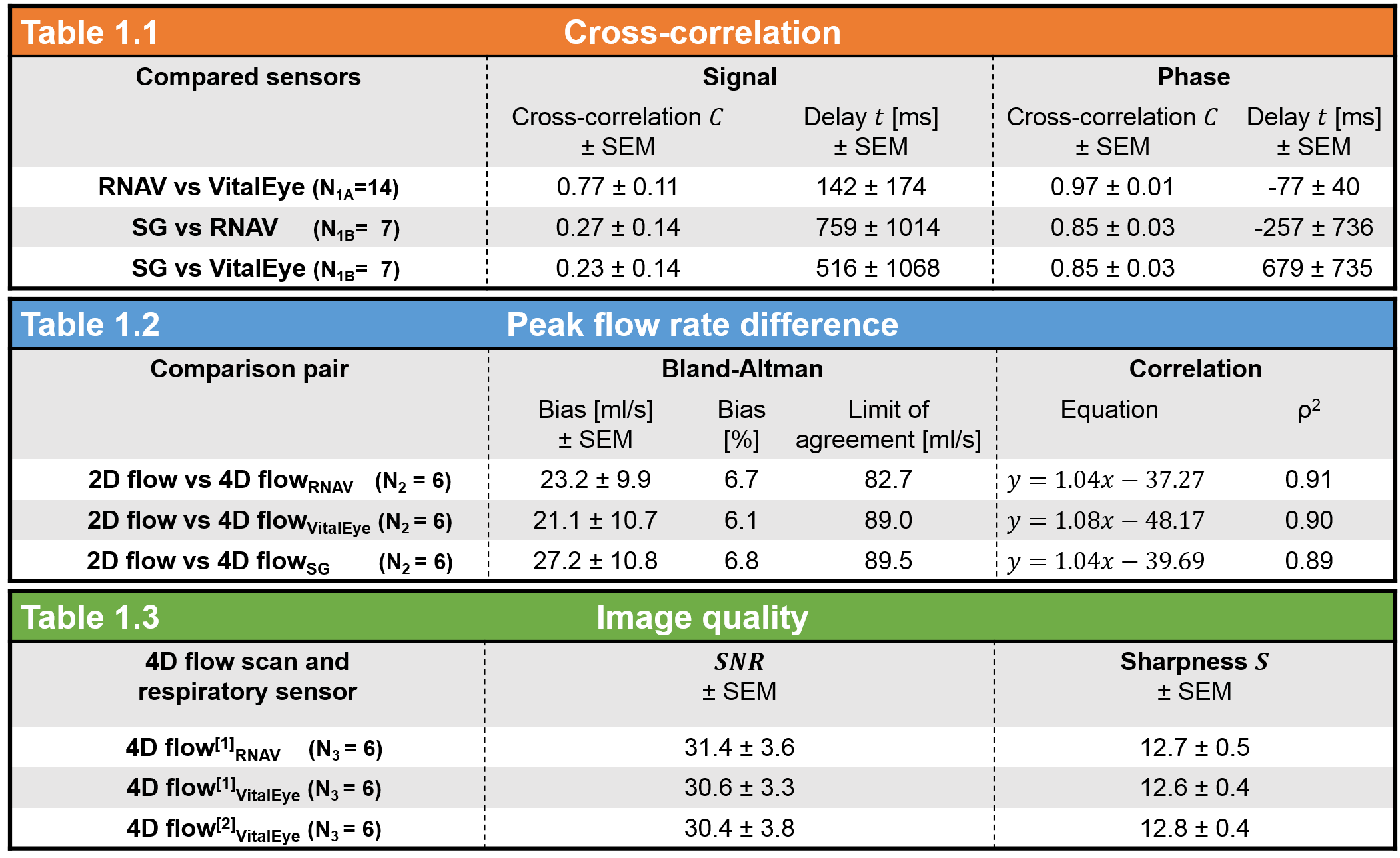
Table 1 (Figure 4):
Results of the cross-correlation, the peak flow rate difference as well as the image quality measurements.
Please note for the image quality comparison that the respiratory signal at 4D flow[1] was measured with RNAV and VitalEye, wherefore at 4D flow[2] only with VitalEye in a second scan.