1323
Rapid Whole Heart Coronary MRA with 100% respiratory gating efficiency: Fast 3D Wheel data sampling with denoising deep learning reconstruction1Department of Radiology, Tohoku University Hospital, Sendai, Miyagi, Japan, 2Canon Medical Systems Corporation, Otawara, Tochigi, Japan
Synopsis
Our proposed Whole Heart Coronary MR Angiography with 100% respiratory gating efficiency using Fast 3D Wheel data acquisition implementing denoising deep learning reconstruction allowed the rapid data acquisition consistently within 3 minutes in spite of irregular breath pattern while maintaining the image quality and contrast ratio of conventional scan. This technique will improve the ease-of-use of coronary artery imaging for practical use.
INTRODUCTION
Whole Heart Coronary MR Angiography (WHCA) is usually respiratory gated to avoid respiratory-motion related artifacts. However, irregular breathing pattern prolongs variable and unpredictable imaging times with low scan efficiency, which subsequently results in image quality degradation.1 We have developed a rapid and easy-to-use WHCA technique with 100% respiratory gating efficiency using “Fast 3D Wheel” data acquisition implementing denoising deep learning reconstruction (dDLR). The purpose of this study was to compare image quality and scan time of the proposed technique with those of a conventional WHCA.METHODS
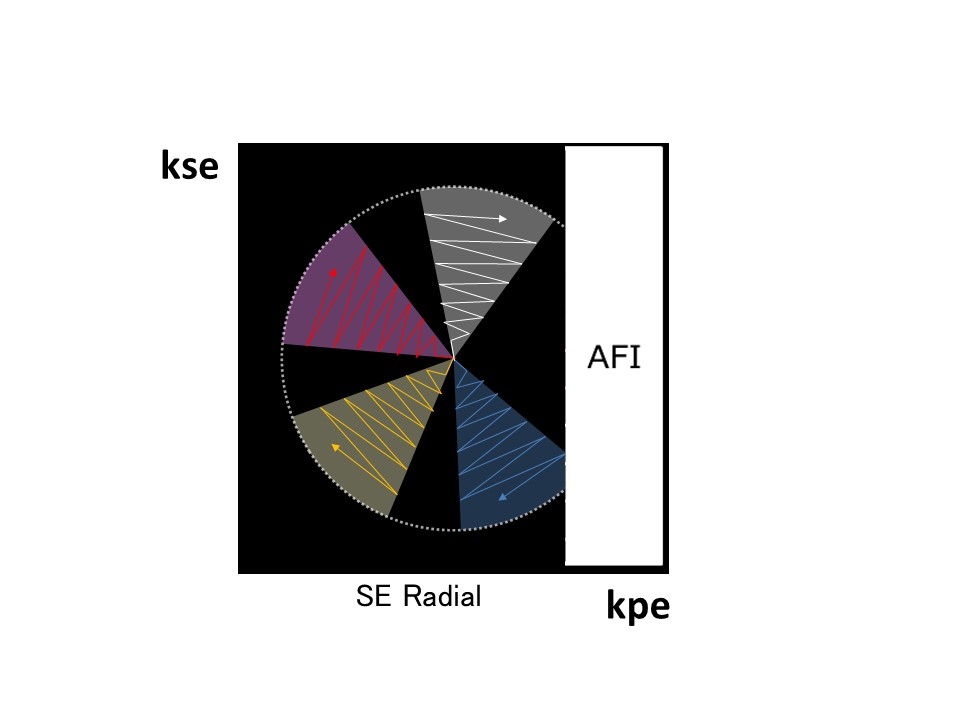
In this study, we used the “Fast 3D Wheel” data acquisition2 (Figure 1) for rapid WHCA with 100% respiratory gating efficiency. This sequence consisted of the following two scheme: 1) “Wheel” shaped data sampling from the center of k-space toward high frequency in the phase encoding and slice encoding direction, and 2) “Fast 3D” sequence which had Zigzag data acquisition every two slice encode providing twice sampling efficiency. Five healthy volunteers underwent coronary MRA on a 3T machine (Vantage Galan, Canon Medical Systems; Slew rate 100mT/m). Volunteer scans were conducted under an approved IRB protocol. The proposed WHCA was imaged with ECG-triggered and navigator-gated under free breathing acquisition in axial sections covering the whole heart. T2 preparation and fat suppression were implemented. The width of Real time Motion Correction (RMC; navigator echo respiratory gating) was set to 30mm. Imaging parameters were TR=3.1msec, TE=1.1msec, FA=12degrees, BW=651, number of segments=2, filling ratio of Fast 3D=65%, slice thickness=1.7mm and pixel size=1.82x1.48mm2. Then, the acquired images were reconstructed using dDLR.3 Conventional WHCA was also performed using fast gradient echo sequence with the same spatial resolution and scan coverage as the proposed one. The width of RMC was set to 5mm. In main segments of the coronary artery (LMT:#5,LAD:#6,#7,LCx:#11,#13,RCA: #1,#2,#3), image quality (vessel visualization and artifact) of the proposed rapid WHCA and conventional WHCA were evaluated on segment basis using the 4-point scale (0= poor/non-diagnostic, 1= fair/moderate blurring, 2= acceptable/mild blurring, 3= good/no blurring). Contrast ratio between vessel lumen and myocardium was also measured. Images were assessed using multi-planar reconstruction and thin-slab maximum intensity projection. Scan time for the both acquisitions was measured. Statistical analysis included paired t tests for the comparison of variables between the two acquisitions. A p value < 0.05 was considered statistically significant.RESULTS
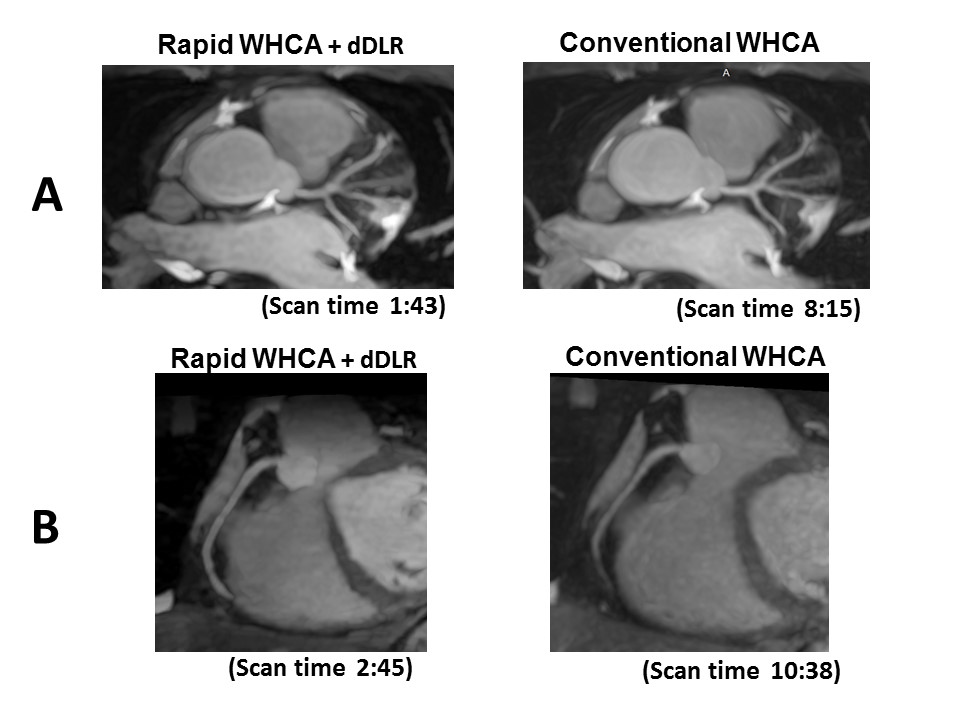
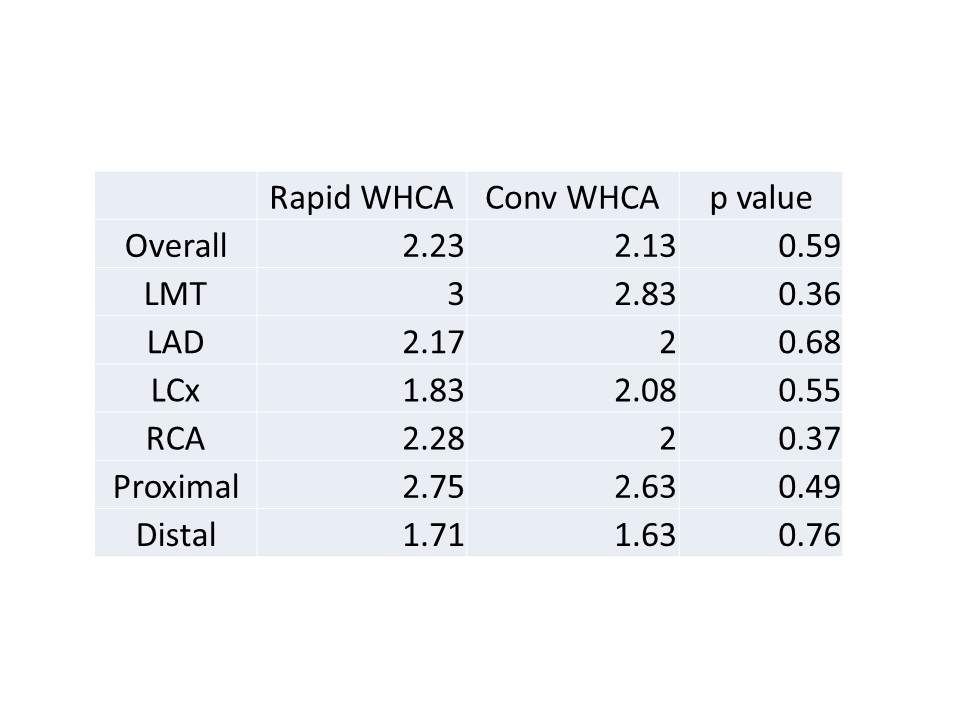
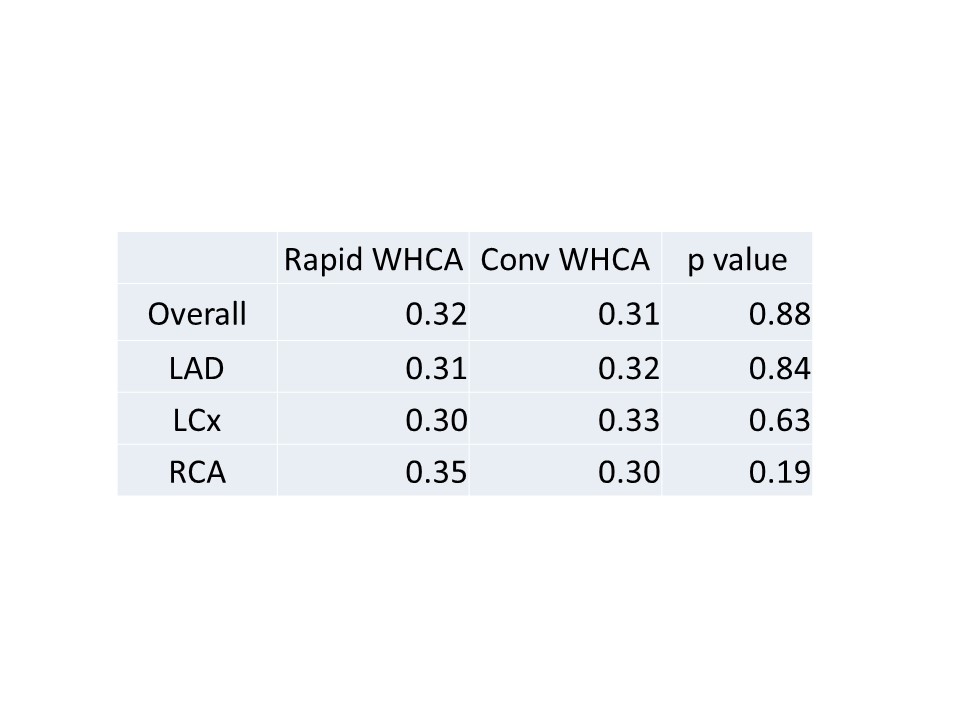
The mean scan time was 2min.32sec. (within 3 min. and 100% respiratory gating efficiency in all volunteers) in rapid WHCA and 11min. 37sec. (mean success rate of respiratory gating: 47%) in conventional WHCA. Image qualities in overall and each coronary artery (LMT/LAD/LCx/RCA) were not significantly different between both WHCAs (Table 1). The mean score in distal segments (#7, #13, #3) were significantly lower than those in proximal segments in both WHCA (p < 0.0001), however there were no significant difference between rapid and conventional WHCA (Table 1). Contrast ratio between vessel lumen and myocardium in overall and each coronary artery (LAD/LCx/RCA) was comparable between rapid and conventional WHCA (Table 2).DISCUSSION
In this study, we applied three techniques for the purpose of rapid acquisition without image quality degradation. (1) “Wheel” shaped data sampling which is robust for motion enabled the higher efficiency of respiratory navigator gating. (2) “Fast 3D” data acquisition and shorter TR increased the data sampling in mid-diastole of RR interval. (3) dDLR improved the SNR reduction caused by less data sampling and shorter TR. Cartesian acquisition in combination with respiratory gating and tracking is still the most widely used technique for WHCA. The relatively small acceptance window and the requirement of careful planning of the navigator beam limit its applicability in clinical practice. Our proposed WHCA allowed a rapid data acquisition consistently within 3 minutes in spite of irregular breath pattern while maintaining the image quality of conventional WHCA. Further studies are needed to put this rapid technique to practical examination, especially for diagnosis of coronary artery stenosis.CONCLUSION
This novel rapid WHCA technique provide the reduced scan time within 3 minutes with comparable image quality and contrast ratio to conventional WHCA, and will be of great help for practical use.Acknowledgements
No acknowledgement found.References
1. Sakuma H, Ichikawa Y, Chino S, et al. Detection of coronary artery stenosis with whole-heart coronary magnetic resonance angiography. J Am Coll Cardiol. 2006; 48(10):1946-50.
2. Ishi, K. Lijun Zhang, Umeda M, et al. k-space trajectory investigation for shorten imaging time of 3D Fast Advanced Spin Echo(FASE3D). The 45th Annual Meeting of the Japanese Society of Magnetic Resonance in Medicine, 2017
3. Kidoh M, Shinoda K, Kitajima M, et al. Deep Learning Based Noise Reduction for Brain MR Imaging: Tests on Phantoms and Healthy Volunteers. Magn Reson Med Sci. 2019 Sep 4. [Epub ahead of print]
Figures