1322
Impact of sub-millimeter isotropic resolution on the visualization of coronary arteries in patients undergoing accelerated whole-heart CMRA1Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom
Synopsis
The recent integration of undersampled acquisitions with image-navigators and non-rigid motion-correction have enabled free-breathing 3D whole-heart coronary MR angiography (CMRA) with sub-millimeter isotropic resolution in clinically feasible scan times in healthy subjects. The high acceleration factor and spatial resolution however must be balanced with the need for a robust and high-quality image reconstruction. We sought to assess whether this highly accelerated sub-millimeter isotropic resolution contrast-free CMRA framework could reliably improve the visualization of coronary arteries in comparison to lower resolution (and lower acceleration factor) CMRA in patients with suspected coronary artery disease who underwent CT coronary angiography.
INTRODUCTION
CT coronary angiography (CTCA) is the clinical gold standard for the non-invasive assessment of coronary artery stenosis mainly due to its fast scan time and high sub-millimeter isotropic spatial resolution. The recent integration of undersampled acquisitions with image-navigators and non-rigid motion-correction have enabled free-breathing 3D whole-heart coronary MR angiography (CMRA) with sub-millimeter isotropic resolution (0.9mm3) in a clinically feasible scan time of ~8min in healthy subjects.1 The high acceleration factor and spatial resolution however has to be balanced with the need for a robust and high quality reconstruction.2 Here we sought to assess whether this highly accelerated sub-millimeter isotropic resolution contrast-free CMRA framework could reliably improve the visualization of coronary arteries in comparison to lower resolution CMRA in patients with suspected coronary artery disease (CAD). A lower acceleration factor was considered for the lower spatial resolution CMRA to obtain similar scan times, and thus similar respiratory motion artefacts, as compared to the sub-millimeter scan. CMRA was performed with acceleration factors of 5x (0.9mm3 resolution) and 2.5x (1.2mm3 resolution) in fifteen patients that underwent CTCA and quantitative image analysis was performed in terms of vessel sharpness and visible vessel length.METHODS
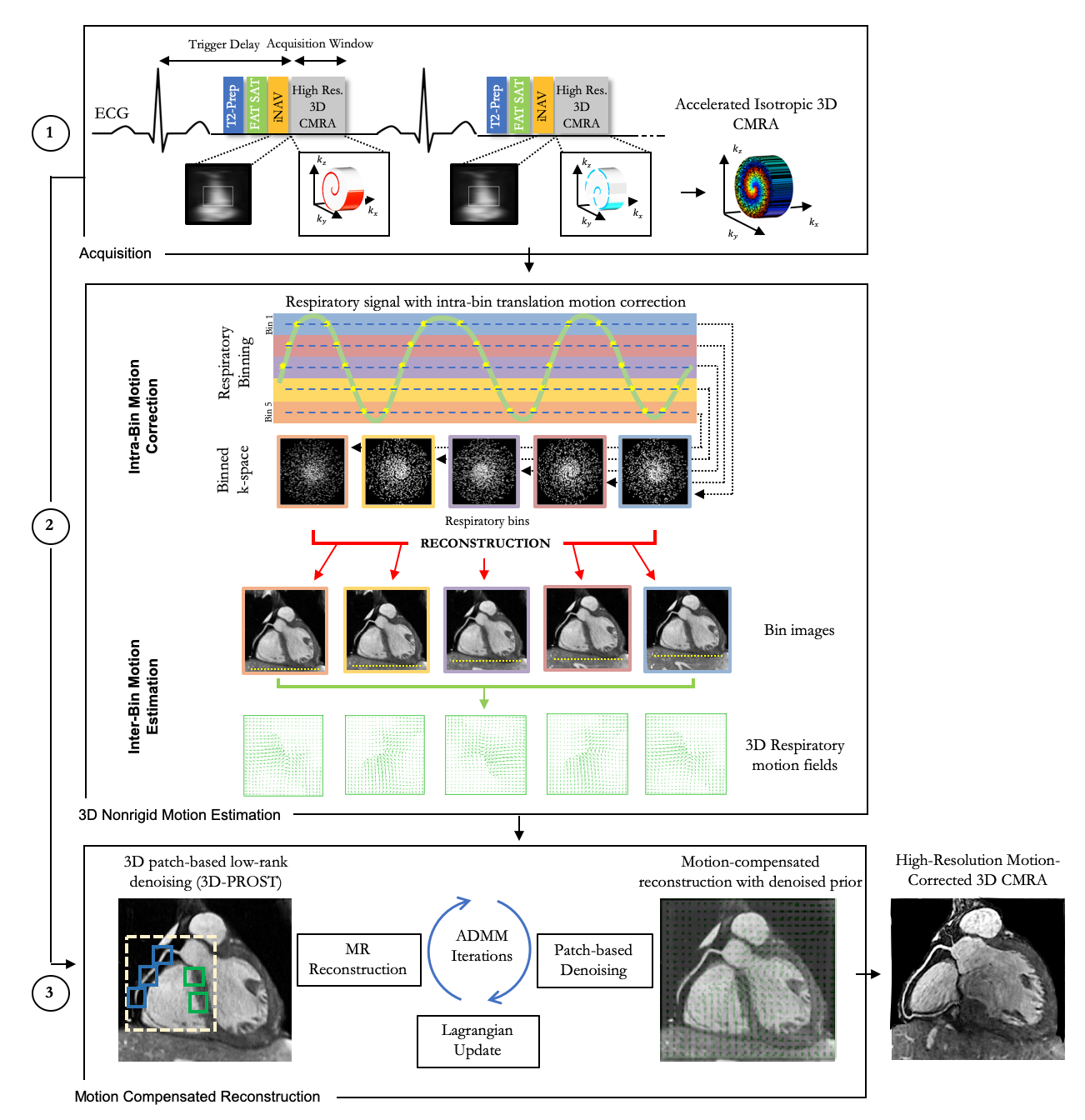
Imaging: Fifteen patients (3 females, mean age 55±8 years, range 41-71 years old) with suspected CAD undergoing a clinically indicated CTCA were recruited for subsequent free-breathing contrast-free whole-heart CMRA. Accelerated whole-heart CMRA acquisitions were performed on a 1.5T scanner (Siemens Magnetom Aera) with an undersampled variable-density Cartesian trajectory with spiral-like order.2,3 A 2D image-navigator (iNAV) preceded each spiral-like arm acquisition to enable beat-to-beat 2D translational and bin-to-bin 3D non-rigid respiratory motion correction of the heart with 100% scan efficiency (no respiratory gating).4 Scan parameters included: TR/TE=3.7/1.6 ms, bandwidth = 890Hz/px, FOV=320x320x86-130mm3, flip angle (FA) = 90°, T2-preparation duration = 40 ms, SPIR (Spectral Presaturation with Inversion Recovery) fat-saturation FA = 130°, 14 linear ramp-up pulses for iNAV, subject specific mid-diastolic trigger delay and acquisition window (range: 73-103 ms). Two CMRA datasets were acquired in each patient with identical parameters, but one with 0.9mm3 isotropic resolution (5x acceleration), and the other with 1.2mm3 isotropic resolution (2.5x acceleration). The patients underwent a clinically indicated CTCA with a third-generation dual source CT 192x2-sections (SOMATOM Force, Siemens Healthcare, Forchleim, Germany) which included sublingual glyceryl trinitrate and intravenous beta-blocker (metoprolol). CTCA images were reconstructed to 0.6mm3 isotropic resolution.Reconstruction & Analysis: Non-rigid 3D motion fields were estimated using respiratory binning and soft-gating reconstruction5 and incorporated into a non-rigid motion-compensated reconstruction with patch-based low-rank regularization (NR-PROST).1,2 The 3D CMRA data was reconstructed to 0.6mm3 isotropic resolution. 3D curved planar reformations were conducted (Horos software, v3.3.4) for CMRA and CTCA volumes. Vessel sharpness and visible length of the left and right coronary arteries (LAD/RCA) were measured and compared using SoapBubble software.6
RESULTS
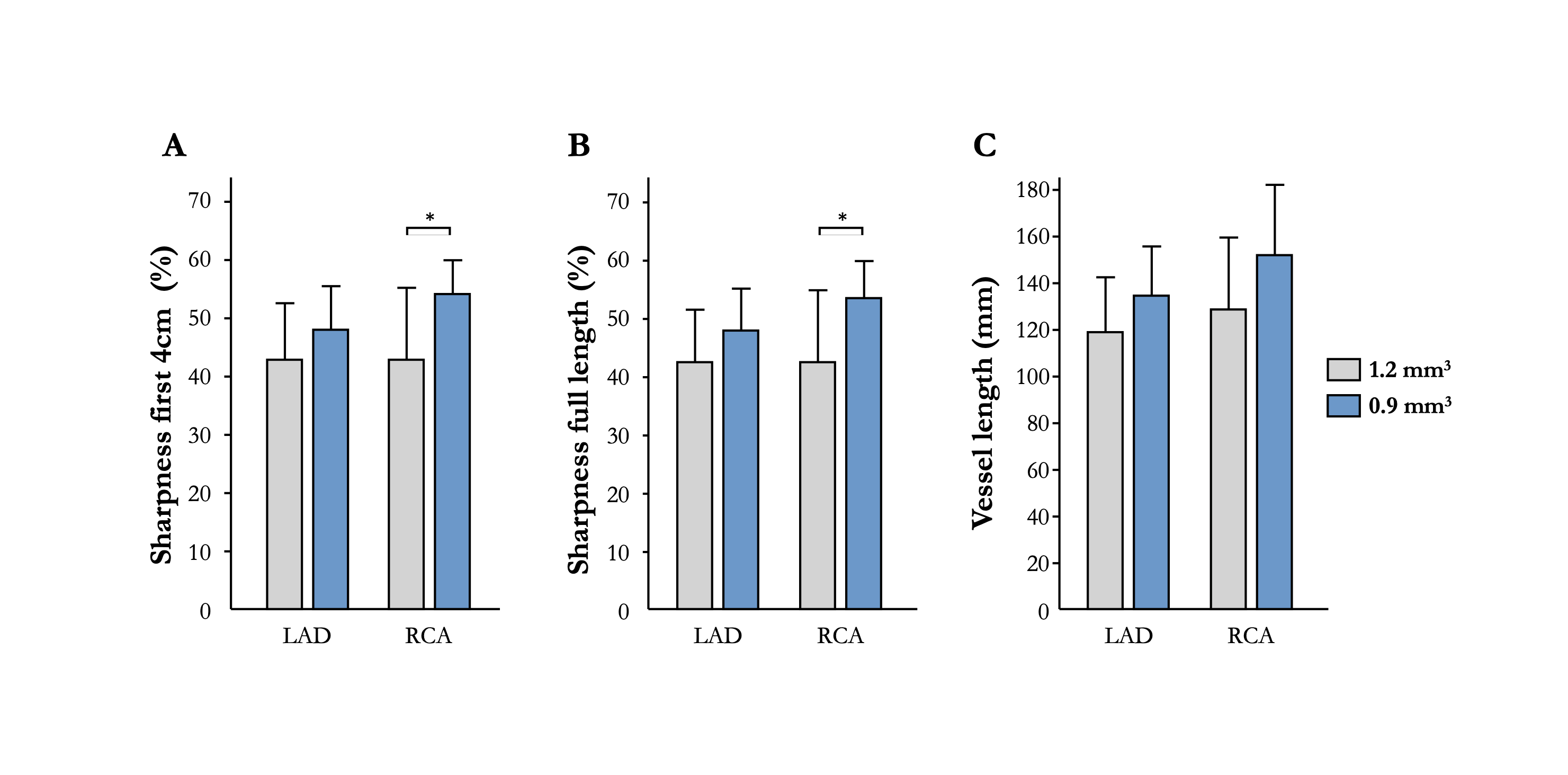
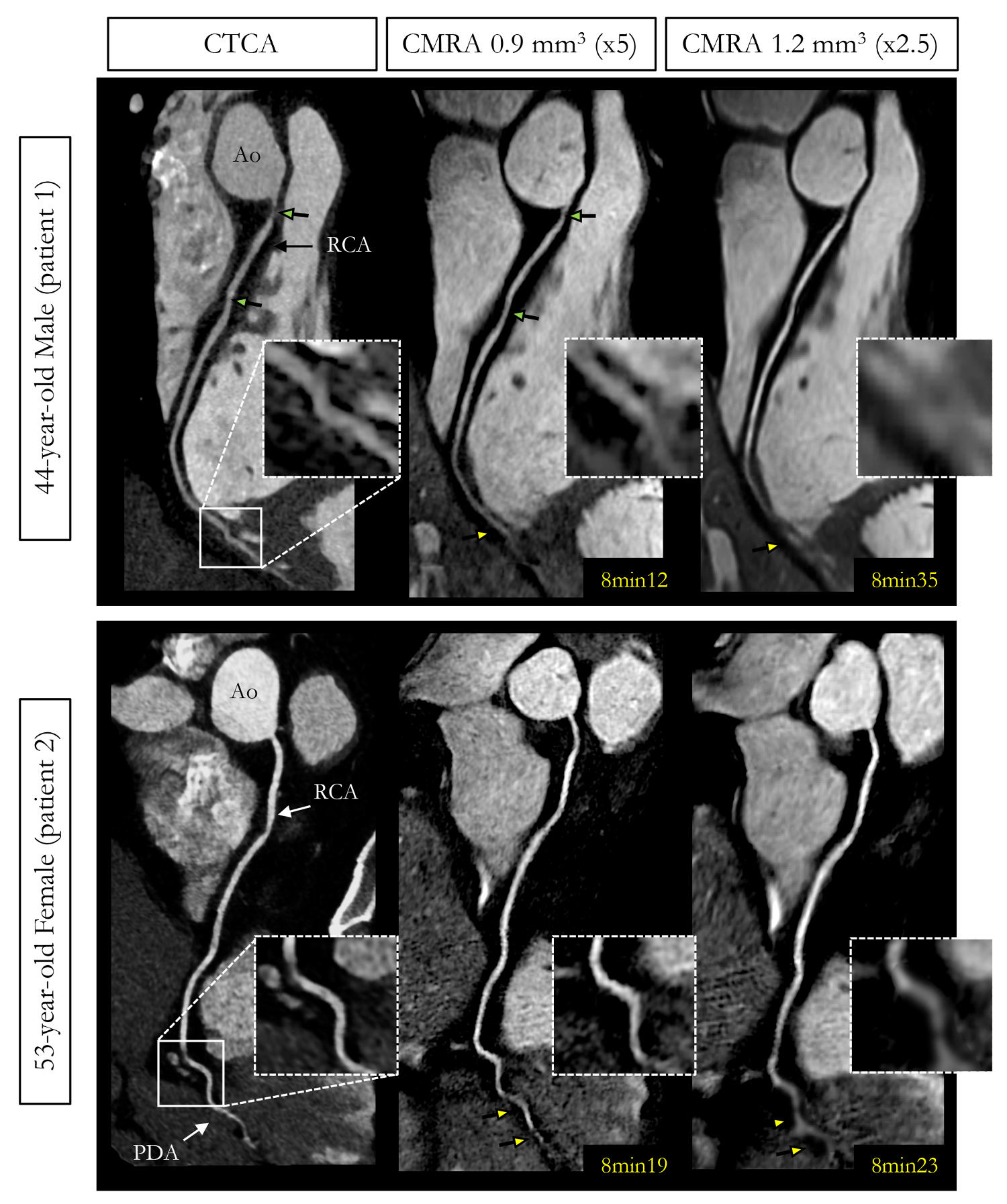
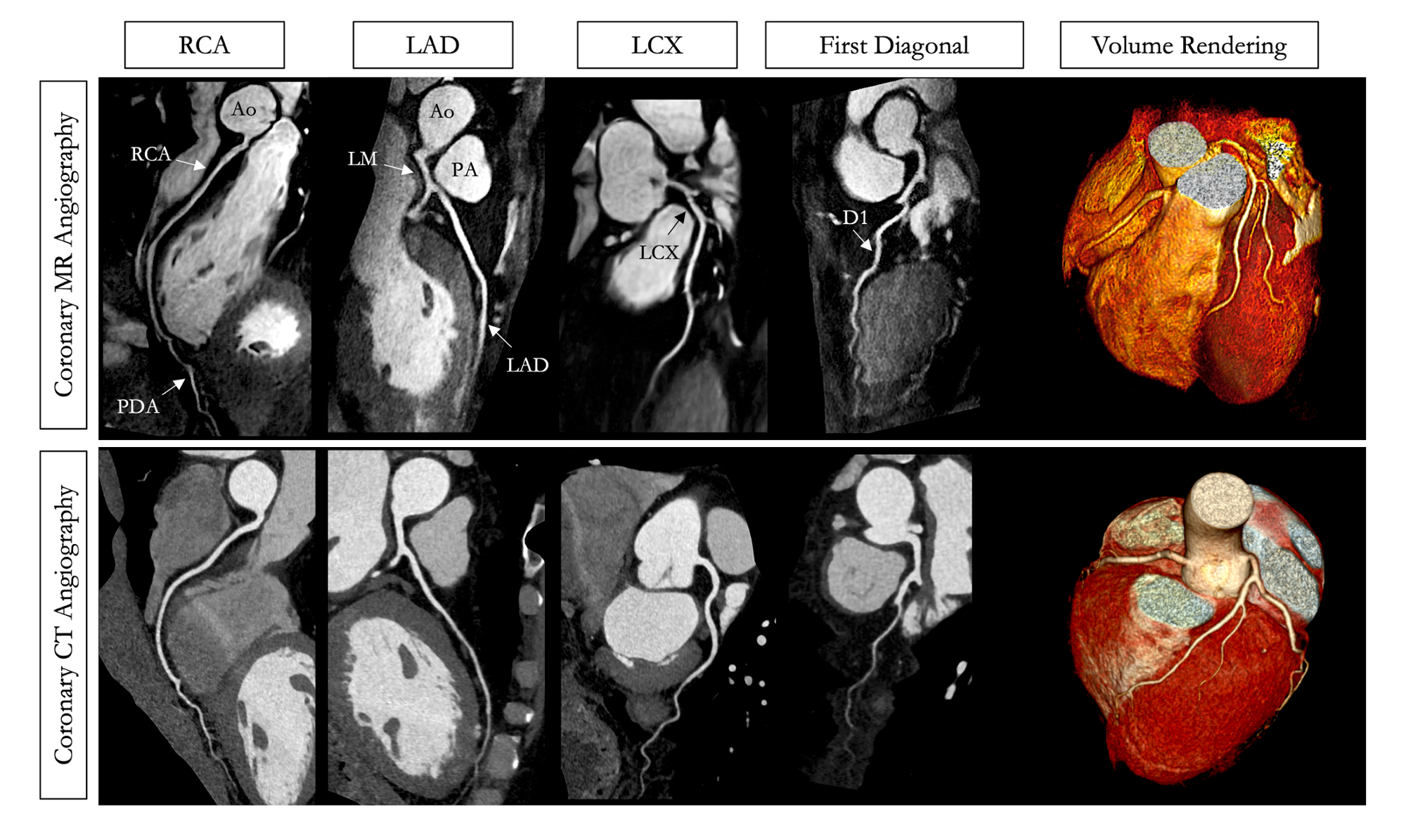
Average scan times were 7min26s±1min45s (0.9mm3) and 7min51s±1min0s (1.2mm3, P=0.50) with 100% respiratory scan efficiency. Vessel sharpness (first 4cm and full length) was improved at sub-millimeter spatial resolution for both LAD (full length: 48±7% vs. 42±9%, P=0.07, for 0.9mm3 and 1.2mm3 resolution respectively) and RCA (full length: 53±7% vs. 42±12%, P<0.05, Figure 2a-b). Visible length of the coronary arteries was also improved at sub-millimeter spatial resolution for both LAD (134±22mm vs. 119±23mm, P=0.08) and RCA (152±30mm vs. 129±31mm, P=0.05, Figure 2c). The distal portions of the coronary arteries were better visualized with 0.9mm3 isotropic resolution than with 1.2mm3 isotropic resolution (Figure 3). A representative CMRA dataset from a 53-year-old healthy male patient is shown in Figure 4. CMRA with 0.9mm3 isotropic resolution combined with NR-PROST reconstruction allows for good visualization of the LAD, RCA and left circumflex territories from the proximal to the distal segments with good image quality and visual image sharpness. CMRA images in patients show an excellent delineation of the coronary vasculature, comparable to that of CTCA (Figures 4 and 5).CONCLUSION
The good definition of the coronary vasculature suggests that highly accelerated sub-millimeter isotropic CMRA might be the preferred approach over lower resolution (lower undersampling) CMRA for the assessment of coronary stenosis in CAD patients. With the described framework, high-resolution 3D whole-heart CMRA can be acquired at sub-millimeter isotropic resolution in about 8min, with an overall image quality visually comparable to that of CTCA. More extensive clinical validation in patients with suspected coronary artery disease is now warranted.Acknowledgements
This work was supported by EPSRC (EP/P001009, EP/P007619, EP/P032311/1) and Wellcome EPSRC Centre for Medical Engineering (NS/ A000049/1).References
1. Bustin A et al., Highly accelerated whole-heart isotropic sub-millimeter CMRA with non-rigid motion correction. In: Proceedings of the 27th Annual Meeting of ISMRM Montreal Canada 2019;p.978.
2. Bustin A et al., Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction, Magn. Reson. Med. 2019;81(1):102-115.
3. Prieto C et al., Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J. Magn. Reson. Imaging 2015;41:738-746.
4. Henningsson M et al., Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn. Reson. Med. 2012;67:437-445.
5. Cruz et al., Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn. Reson. Med. 2017;77:1894-1908.
6. Etienne A et al., “Soap-Bubble” visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn. Reson. Med. 2002;48:658-666.
Figures