1310
Interaction of Aortic Flow and Myocardial Motion in Patients with Repaired Tetralogy of Fallot1Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 4Department of Pediatrics, National Yang-Ming University, Taipei, Taiwan
Synopsis
We aimed to investigate the abnormal aortic flow and its adverse interaction with regional myocardial motion in repaired tetralogy of Fallot (rTOF) patients. The rTOF patients were divided into rTOF1and rTOF2 groups according to their indexed right ventricular end-systolic volume (RVESVi). The rTOF2 group demonstrated increased aortic retrograde fraction and there was a correlation exhibited between retrograde fraction and systolic myocardial motion. In conclusion, the assessments of abnormal artic flow and altered myocardial motion were helpful in elucidating the possibly adverse interaction between the characteristics of the aorta and myocardium in rTOF patients with different degrees of RV dilatation.
Introduction
Aortopathy is associated with numerous congenital heart diseases, including patients with repaired tetralogy of Fallot (rTOF)1. The aortic wall in rTOF patients exhibited marked degeneration in the tunica media from infancy. The degeneration can be viewed as an important cause of dilated aortic root and increased stiffness2, which consequently induced aortic aneurysm, rupture, and aortic regurgitation and associated with left ventricular hypertrophy, reduced coronary artery flow, and left ventricular failure3. Previous study has reported rTOF patients had significantly higher arterial wave reflection than the controls, which increased the pulsatile load on the left ventricle and significantly contributed to decreased cardiac output4. The relationship between hemodynamic alterations and the wall characteristics was demonstrated as an adaptive process with disease progress10. Currently, the aortic flow and its correlation with regional myocardial motion in patients with rTOF have not been discussed thoroughly. The indexed right ventricular end-systolic volume (RVESVi) was reported as a suitable parameter for assessing the progression of RV dilation5. We would follow this guideline to Group patients. The purpose of this study was to investigate the abnormal aortic flow and its possible adverse interaction with regional myocardial motion in rTOF patients with different degrees of RV dilatation.Methods
This study recruited 39 rTOF patients (male/female=25/14, 23 ±4 y/o) and 38 age-matched normal subjects (male/female=23/15, 22 ±2 y/o) without known cardiovascular diseases. The rTOF patients were divided into rTOF1 (n=12, male/female=7/5, 24±4 y/o) and rTOF2 groups (n=27, male/female=18/9, 23±4 y/o) according to their RVESVi5.Images were acquired in a 3-T clinical MR scanner (Tim Trio or Skyra, Siemens, Erlangen, Germany) with prospective ECG triggering and navigator-echo to synchronize with cardiac and respiratory motion. 4D flow was acquired with TR/TE=10.8/2.9 ms, voxel size=3.2x1.4x3.5 mm3, flip angle=7°, Venc=150 cm/s, acceleration factor=5, and temporal resolution=41.6 ms. For myocardial motion velocity, all subjects were imaged in base, mid, and apex with parameters of TR/TE=6.5/4.2 ms, voxel size=1.2x1.2x6 mm3, flip angle=7°, acceleration factor=5, Venc=15 and 25 cm/s for in-plane and through-plane motions, respectively, and temporal resolution=26 ms.
Fourteen 2D planes were determined perpendicular to the long axis of the aorta for calculating aortic hemodynamics (Figure 1). The retrograde flow fraction was calculated as the ratio of retrograde and antegrade flow volume. Aortic distensibility was defined as6:
distensibility =(AoS − AoD)/(AoD) × (SBP − DBP)
where AoS and AoD are systolic and diastolic aortic diameters, respectively, and SBP and DBP are systolic and diastolic blood pressure, respectively, in the aorta. Biventricular peak systolic and diastolic myocardial motion velocity in radial (Vr) and longitudinal (Vz) directions and the corresponding time-to-peak (TTPr, TTPz) were also quantified. The ANOVA and Pearson correlation were performed when appropriate. P<0.05 was considered as statistical significance.
Results
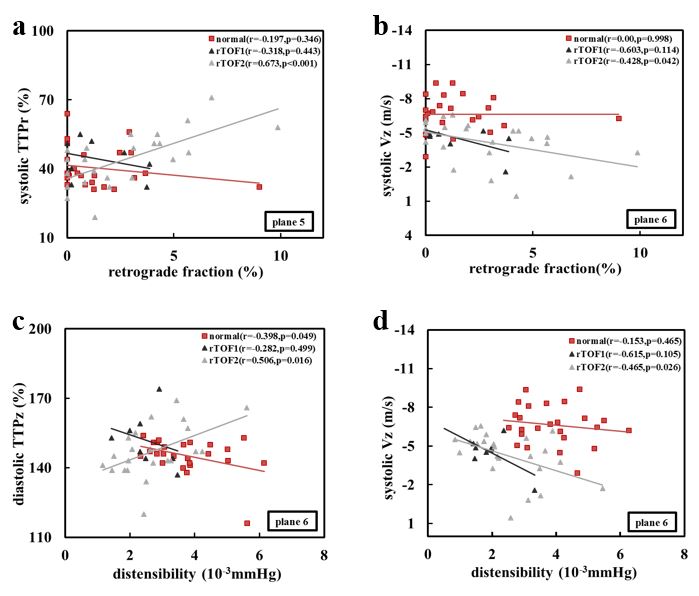
The normal subjects were with RVESVi of 33.7±7.6 cm3/m2. According to this RVESVi, the rTOF patients were divided into rTOF1 with normal RVESVi and rTOF2 with significantly larger RVESVi (31.8±6.3 vs. 74.6±30.6 cm3/m2, P<0.001). Table 1 illustrates the demographics of normal, rTOF1, and rTOF2 groups. Only the rTOF2 group presented dilated RV. In Figure 2, only the rTOF2 group demonstrated significantly higher aortic retrograde fraction in the ascending and descending aorta (P<0.05~0.01). Considering the aortic distensibility, both the two rTOF subgroups exhibited significantly decreased values compared to the normal group almost in all 14 planes (P<0.05~0.01). Solely in the rTOF2 group, the retrograde fraction correlated with systolic TTPr at plane 5 (r=0.673, p<0.001) and with systolic Vz at plane 6 (r=-0.428, p=0.042), as shown in Figures 3. Similarly, only in the rTOF2 group, the aortic distensibility correlated positively with diastolic TTPz at plane 6 (r=0.506, p=0.016) and negatively with systolic Vz at planes 6 (r=-0.465, p=0.026).Discussion and Conclusions
In this study, rTOF patients with dilated RV demonstrated more serious aortic retrograde fraction and there was a correlation exhibited between retrograde fraction and systolic myocardial motion. The dilatation of the ascending aorta was reported to be associated with presence of aortic regurgitation, which may have adverse impacts on the global cardiac function, i.e. LVEF, in rTOF patients7. In our study, although the aortic retrograde fraction in rTOF group was not serious, we still can observe that increased particularly have correlations with prolonged systolic TTPr and systolic Vz in base of rTOF2 group, illustrating the adverse impact of the aortic flow on LV regional myocardial motion, especially in rTOF patients with dilated RV. Although the aortic distensibility presented decreased values in two rTOF subgroups, only the rTOF2 group demonstrated its correlation with myocardial motion. The altered characteristics of the aortic wall in combination with the dilated RV in rTOF2 might jointly impair the regional myocardial motion in the LV. We speculated that because of an adaptive coupling mechanism between the aorta and LV, rTOF2 patients presented preserved global LV function even those patients were with substantial undermined myocardial motion. This correlation between distensibility and the regional myocardial motion was in contrast with the studies prior8.9. The reason for that is our patients were young. In conclusion, the assessments of abnormal aortic flow and altered myocardial motion were helpful in elucidating the possible adverse interaction between the characteristics of the aorta and myocardium in rTOF patients with different degrees of RV dilatation.Acknowledgements
No acknowledgement found.References
- Therrien J , Webb G, et al. Clinical update on adults with congenital heart disease. The Lancet. 2003; 362(9392):1305-1313.
- Tan, J. L, et al. Intrinsic Histological Abnormalities of Aortic Root and Ascending Aorta in Tetralogy of Fallot: Evidence of Causative Mechanism for Aortic Dilatation and Aortopathy. Circulation. 2005; 112(7):961-968.
- Niwa K, et al. Aortopathy in Congenital Heart Disease in Adults: Aortic Dilatation with Decreased Aortic Elasticity that Impacts Negatively on Left Ventricular Function. Korean circulation journal. 2013; 43(4):215-220.
- Senzaki H , Iwamoto Y , Ishido H , et al. Arterial haemodynamics in patients after repair of tetralogy of Fallot: influence on left ventricular after load and aortic dilatation. Heart. 2008; 94(1):70-74.
- Buddhe S , Shah A , Lai W W, et al. Progression of right ventricular dilation in repaired tetralogy of fallot. Journal of Magnetic Resonance Imaging. 2015; 41(3):730-737
- Groenink M, de Roos A, Mulder BJ, Spaan JA, et al. Changes in aortic distensibility and pulse wave velocity assessed with magnetic resonance imaging following beta-blocker therapy in the Marfan syndrome. The American journal of cardiology. 1998;(82):203–208.
- Ordovas K G , Keedy A , Naeger D M, et al.
Dilatation of the ascending aorta is associated with presence of aortic
regurgitation in patients after repair of tetralogy of Fallot. The
International Journal of Cardiovascular Imaging. 2016; 32(8):1265-1272.
- Baykan A O , Mustafa Gür, Gülhan Yüksel Kalkan, et al. Assessment of myocardial performance index and its association with aortic elasticity in patients with ascending aortic aneurysm. Archives of the Turkish Society of Cardiology. 2016; 44(2):114-122.
- Li Y , Deng Y B , Bi X J , et al. Evaluation of myocardial strain and aortic elasticity in patients with bicuspid aortic valve. Journal of Huazhong University of Science and Technology. 2016; 36(5):747-751
- Lee, Suji, et al. Evaluation of Flow Pattern in the Ascending Aorta in Patients with Repaired Tetralogy of Fallot Using Four-Dimensional Flow Magnetic Resonance Imaging. Korean journal of radiology. 2019;20(9): 1334-1341.
Figures
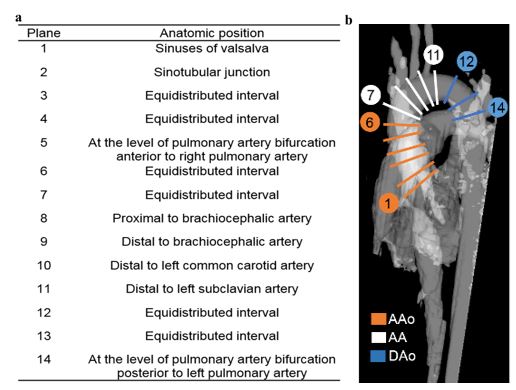
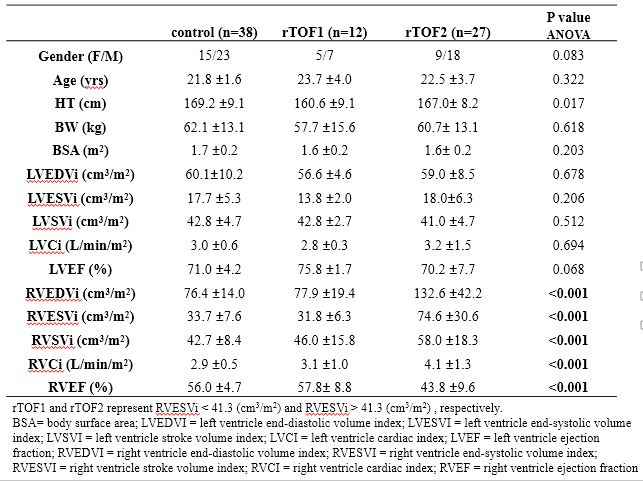
Table 1. The demographic characteristics of the study population.