1243
Radiomics analysis for Characterizing Ovarian Tumor Based on a DCE-MRI Pharmacokinetic Protocol1Shanxi Medical University Second Affiliated Hospital, Taiyuan, China, 2GE Healthcare, Beijing, China., Beijing, China, 3GE Healthcare, MR Research China, Beijing, China, Beijing, China
Synopsis
DCE-MRI and its subsequently derived pharmacokinetic parameters have been adopted to explore tumor angiogenesis and vascular permeability changes inside tumors and improve the diagnostic accuracy of ovarian tumors. Radiomics can convert medical images to mineable high-dimensional quantitative imaging features based on automatic feature extraction algorithms. In this study, we present a radiomics model based on a DCE-MRI PK protocol and establish an effective and noninvasive 3-class classification prediction model for the discrimination among benign, borderline and malignant ovarian tumors.
Purpose
To evaluate the efficiency of predictive models constructed from radiomics features extracted from a DCE-MRI pharmacokinetic (PK) protocol in discriminating among benign, borderline and malignant ovarian tumors.Introduction
Ovarian tumors comprise a remarkably heterogeneous group of benign, borderline and malignant lesions and exhibit extensive morphological characteristics. The preoperative characterization of ovarian lesions is of great importance for planning optimal therapeutic procedures and helping to improve patient prognosis. As an advanced technique, dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) and its subsequently derived pharmacokinetic (PK) parameters have been adopted to explore tumor angiogenesis and vascular permeability changes inside tumors and improve the diagnostic accuracy of ovarian tumors[1]. However, the overlapping characteristics between benign and borderline tumors with complex appearances and malignant ovarian masses limit the diagnostic accuracy of DCE-MRI. Radiomics can convert medical images to mineable high-dimensional quantitative imaging features based on automatic feature extraction algorithms[2]. In this study, we present a radiomics model based on a DCE-MRI PK protocol and establish an effective and noninvasive prediction model for the discrimination among benign, borderline and malignant ovarian tumors.Material and Methods
Eighty-two patients with 104 ovarian lesions (33 benign, 18 borderline, and 53 malignant) were evaluated using preoperative DCE-MRI. Prior to DCE-MRI, T1 mapping was performed using a total of 4 flip angles (FAs) (3°, 6°, 9°, and 12°) and three-dimensional spoiled gradient recalled echo sequences. DCE-MRI was performed using a 3D liver acquisition with volume acceleration (LAVA) sequence, and the parameters were as follows: repetition time (TR)/echo time (TE) of 6.5/3.5 ms, field of view (FOV) of 340 × 340 mm2, and slice thickness of 6 mm. A dynamic scan with 50 consecutive phases was performed with the following parameters: number of effective excitations, 0.7; temporal resolution, 6 s; bandwidth, 125 Hz; acceleration factor, 2; and scan time, 5 mins and 20 s. An intravenous gadodiamide (Omniscan, GE Healthcare) injection was started at the start of the fourth phase of the dynamic scan at a dose of 0.1 mmol/kg and a rate of 3 mL/s, followed by a 20 ml saline flush with a power injector. Radiomics features were extracted from 7 types of DCE-MRIs [parameters maps (Ktrans, Kep, Ve, fPV, initial area under the gadolinium contrast agent concentration time curve (IAUGC), and contrast-enhanced ratio (CER) and postC]. To fully reflect the tumor characteristics, all relevant features were incorporated into a PK model for the differential diagnosis of ovarian tumors. the features selection procedure was as follows: (1) minimum redundancy maximum relevance (mRMR), a stable feature selection method for radiomics that uses mutual information (MI) to determine the dependence between different features and classifications, was used to select the 20 most important features; and (2) a random forest analysis was used to select final important features that could be associated with ovarian tumor types. Tree-based strategies used by the random forest analysis naturally rank the features by how well they improve the purity of the node. For the 3-class classification model, 104 lesions were randomly divided into training (72 lesions) and validation (32 lesions) cohorts at a 7:3 ratio. The discrimination abilities of the radiomics signatures were built with the training cohort and tested with the independent validation cohort. The predictive performance of the model was evaluated by receiver operating characteristic (ROC) curve and calibration curve analysis and decision curve analysis (DCA).Results
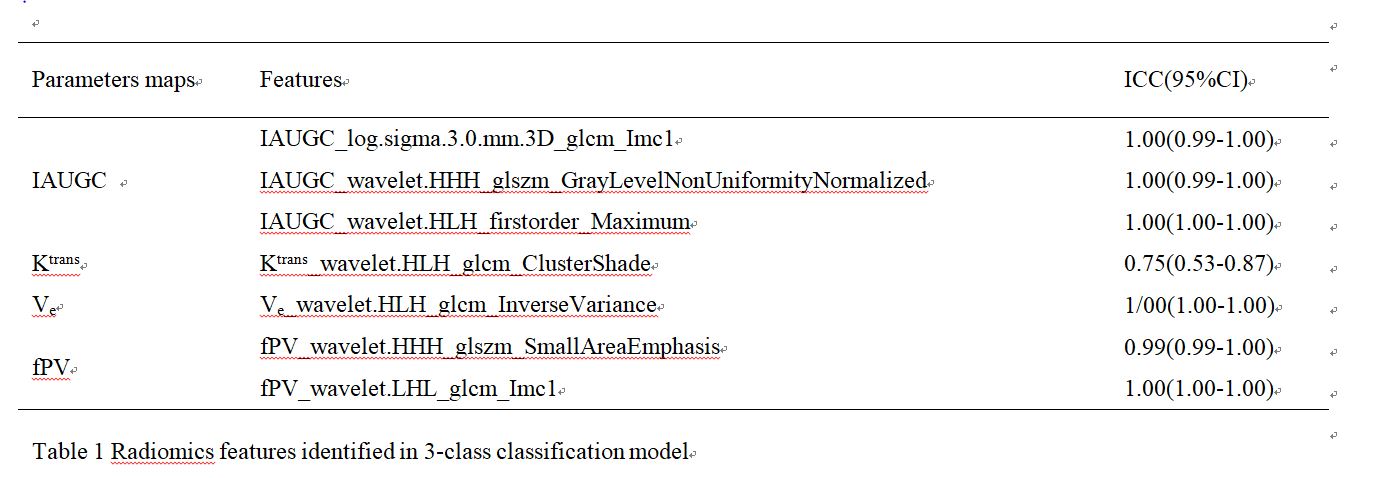
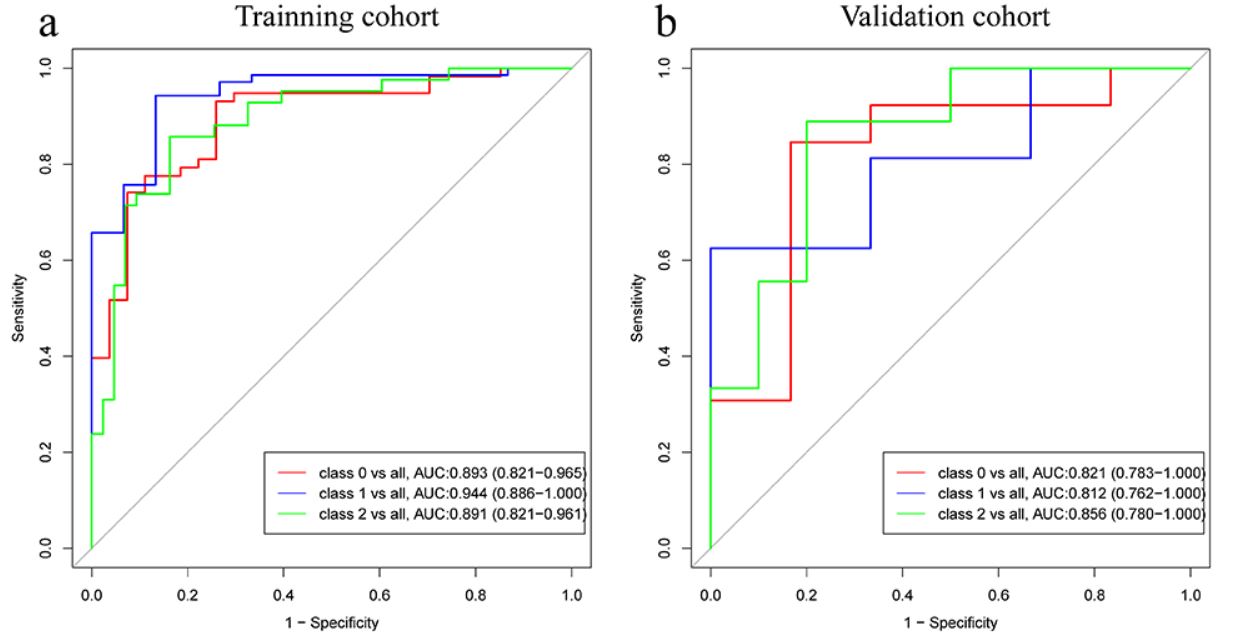
In total, eight features obtained from the DCE-MRI protocol through mRMR and random forest feature importance tool were left for further analysis (Table 1). The 3-class classification model demonstrated similar discrimination performances for the different ovarian tumor types, with AUC values of 0.893 (95% CI: 0.821–0.965), 0.944 (95% CI: 0.886–1.000), and 0.891 (95% CI: 0.821–0.961) for the benign, borderline, and malignant groups, respectively. The model was tested with the validation cohort and obtained an AUC of 0.821 (95% CI: 0.783-1.000) for the benign group, 0.812 (95% CI: 0.762-1.000) for the borderline group, and 0.856 (95% CI: 0.780-1.000) for the malignant group (Fig.1).Conclusion
Radiomics analysis based on the DCE-MRI PK protocol showed promise for discriminating among benign, borderline and malignant ovarian tumors.Acknowledgements
No acknowledgement found.References
[1] Thomassin-Naggara I, Darai E, Cuenod CA et al (2008) Dynamic contrast-enhanced magnetic resonance imaging: a useful tool for characterizing ovarian epithelial tumors. J Magn Reson Imaging 1:111-20
[2] Kumar V, Gu Y, Basu S et al (2012) Radiomics: the process and the challenges. Magn Reson Imaging 9:1234-48
Figures