1214
Evaluate Myocardial Circumferential Kinetic Energy for Patients with Repaired Tetralogy of Fallot
Shi-Ying Ke1, Meng-Chu Chang1, Ming-Ting Wu2, Ken-Pen Weng3,4, and Hsu-Hsia Peng1
1Department of Biomedical Engineering and Environmental Sciences, National TsingHua University, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 4Department of Pediatrics, National Yang-Ming University, Taipei, Taiwan
1Department of Biomedical Engineering and Environmental Sciences, National TsingHua University, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 4Department of Pediatrics, National Yang-Ming University, Taipei, Taiwan
Synopsis
This study aims to evaluate biventricular myocardial circumferential kinetic energy (KEØ) for assessment of regional myocardial function in repaired tetralogy of Fallot (rTOF) patients with preserved global cardiac function. The tissue phase mapping (TPM) was acquired in the basal, mid, and apical slices in the left and right ventricles. We found the altered KE values and abnormal distribution of three-directional %KE in rTOF patients. In conclusion, the altered myocardial KEØ may provide useful information for assessment of regional myocardial function in rTOF patients with preserved global cardiac function.
Introduction
Patients with repaired tetralogy of Fallot (rTOF) is the most common form of cyanotic congenital heart.1 The kinetic energy (KE) plays an important role in pumping blood.2 and patients with atheromatous coronary artery disease were reported to consume much of the internal energy as heat energy, leading to cardiac inefficiency.3 A recent study claimed that evaluating the intraventricular KE without taking the myocardial KE into account may ignore the role of myocardium in generating energy to intraventricular blood flow.4 The myocardial deformation is more superior to predict patient outcome than conventional ventricular function in rTOF patients.5 The correlation between myocardial KE and right ventricular (RV) pressure overload may illustrate a compensatory mechanism of myocardial remodeling in rTOF patients.6 The longitudinal deformation is more sensitive to cardiac related pathologies and circumferential deformation is affected relatively late in the disease process.7 However, the myocardial circumferential KE (KEØ) in rTOF has not been discussed thoroughly. This study aims to evaluate biventricular myocardial KEØ for assessment of regional myocardial function in rTOF patients with preserved global cardiac functionMethod
This study recruited 48 rTOF patients (22.2±4.0 y/o; male/female=29/19) and 46 age-matched normal controls without known cardiovascular diseases (21.7±1.2 y/o; male/female=28/18). Images were acquired at a 3-T clinical MR scanner (Tim Trio or Skyra, Siemens, Erlangen, Germany) with prospective ECG triggering and navigator-echo to synchronize with cardiac and respiratory motion. All subjects were imaged using 2D dark-blood fast low-angle shot sequence for tissue phase mapping (TPM) acquisitions with TR/TE=6.5/4.2 ms, pixel size=1.17x1.17 mm2, slice thickness=6 mm, flip angle=7°, acceleration factor=5, Venc=15 and 25 cm/s for in-plane and through-plane motions, respectively, and temporal resolution=26 ms. In Figure 1, the region-of-interest were determined manually in LV and RV with a self-developed program for computing radial (vr), circumferential (vØ), and longitudinal (vz) velocities. Each time frame was normalized to the individual period of end systolic time and was presented as the percentage of the end-systole (%ES). The voxel-wise KE was calculated as:$$ KE=\frac{1}{2}×ρ ×V×v^2$$where ρ is myocardial density with a value of 1050 kg/m3, Vdenotes voxel volume, and v represents the voxel velocity. We computed three-directional components of KE (KEr, KEØ, and KEz). The difference of KE between peak rapid ejection and peak reduced ejection was defined as peak difference (PD).The rotation angle was defined as the circumferential movement of each slice $$Rotation Angle = \frac{V_{\phi(t,s)}}{100}\times\frac{360°}{2\pi\times R_{ave(s)}}$$where $$$V_{\phi(t,s)}$$$ indicates the segmental averaged $$$V_{\phi}$$$ in slice s at time t, TR is the repetition time and $$$R_{ave(s)}$$$ is the LV temporal averaged radius in slice s. The net rotation was computed as the difference of rotation angles between base and apex during 0-200 %ES. Two-tailed Student t test and Spearman correlation were performed when appropriate. P<0.05 was considered as statistical significance.Results
Table 1 illustrates that rTOF patients were with dilated RV and preserved global RV and LV ejection fraction (RVEF and LVEF, both P>0.05). Compared to normal controls, the LV of rTOF patients exerted significantly higher KEr (P<0.05) and lower KEØ (P<0.01),whilet the RV of rTOF patients demonstrated significantly higher KEr (P<0.01) and lower KEz (P<0.001). In Figure 2, the rTOF group presented substantial lower peak KEØ than normal group at peak rapid ejection and peak reduced ejection in LV, while in RV, lower peak KEØ was presented only at peak reduced ejection. The rTOF group displayed significantly lower PD than normal group only in LV (all P <0.001). Figure 3 displays that the rTOF group presented higher %KEr and lower %KEØ (both P <0.001) in systole. In diastole, the rTOF group revealed increased %KEr and decreased %KEz (both P <0.001). The rTOF group revealed reduced rotation angles than normal group in basal, mid, and apical (all P <0.01~0.001) slices (Table 1). As shown in Figure 4, the rTOF group presented reduced peak net rotation (P <0.01). The normal group demonstrated negative correlation between peak net rotation and mean LV KEØ (R=-0.462, P <0.01) while the rTOF group exhibited a positive correlation (R=0.382, P <0.05).Discussion and Conclusions
In this study, we explored the abnormal KE values and altered distribution of three-directional %KE in rTOF patients. Since the rTOF patients were with preserved LVEF and RVEF, the abovementioned findings implied that KE-relevant indices could be an early sign to reveal the ventricular abnormality. The findings of reduced rotation angles, systolic KEØ and %KEØ in this study were consistent with the previous study using tagging MR8,yet the tissue phase mapping technique can provide higher spatial resolution for evaluating regional myocardial function.The correlation between net rotation and LV KEØ in the normal and rTOF patients, indicated the possible interaction between net rotation and LV KEØ. The negative correlations were shown between net rotation and LV KEØ in normal groups, but positive correlations in rTOF patients. This finding indicated rTOF patients had to generate more KEØ to rotation.
In conclusion, the altered myocardial KEØ may provide useful information for assessment of regional myocardial function in rTOF patients with preserved global cardiac function.
Acknowledgements
No acknowledgement found.References
- Apitz, C, Webb, G. D, et al. Tetralogy of fallot. The Lancet. 2009;374(9699):1462-1471.
- Arvidsson, P. M, Töger, J, et al. Quantification of left and right atrial kinetic energy using four-dimensional intracardiac magnetic resonance imaging flow measurements. Journal of applied physiology. 2013;114(10):1472-1481.
- Stewart, J. T, Simpson, I. A, et al. Left ventricular energetics: heat production by the human heart. Cardiovascular research. 1993;27(6):1024-1032.
- Jeong, D, Anagnostopoulos, P. V, et al. Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired tetralogy of Fallot. The Journal of thoracic and cardiovascular surgery. 2015;149(5):1339-1347.
- Orwat, S, Diller, G. P, et al. Myocardial deformation parameters predict outcome in patients with repaired tetralogy of Fallot. Heart. 2016;102(3):209-215.
- Chang, M. C, Wu, M. T, et al. Does Right Ventricular Myocardial Kinetic Energy Correlate With Pressure Overload in Repaired Tetralogy of Fallot Patients? 2017; ISMRM 25th Annual Meeting in Hawaii, The USA. Program number: 3149.
- Bansal, M., & Sengupta, P. P. Longitudinal and circumferential strain in patients with regional LV dysfunction. Current cardiology reports. 2013;15(3):339.
- Ordovas, K. G, Carlsson, M,et al.Impaired regional left ventricular
strain after repair of tetralogy of Fallot. Journal of Magnetic Resonance
Imaging. 2012;35(1):79-85.
Figures
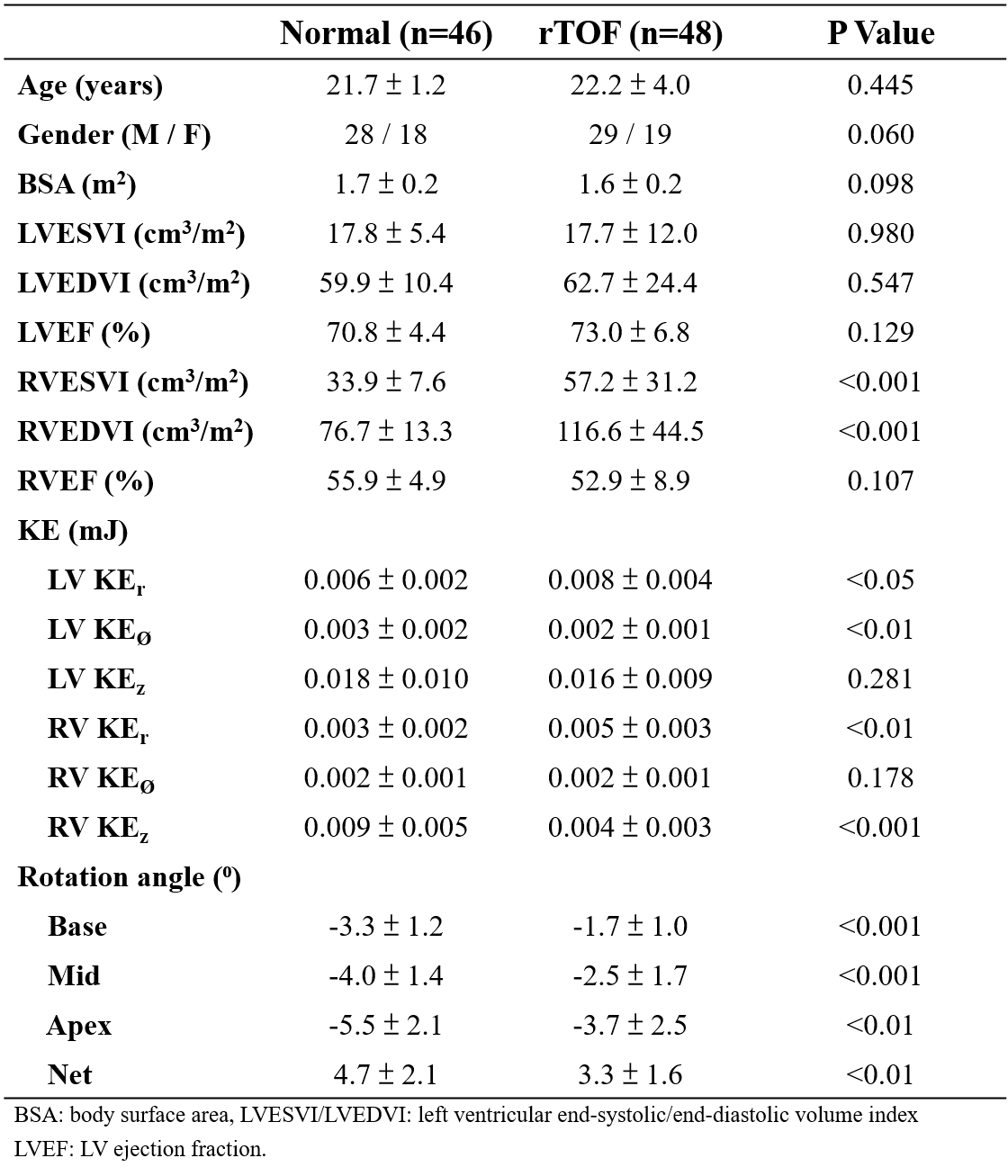
Table
1. Demographic characteristics, kinetic energy, and rotation angle of study
population.
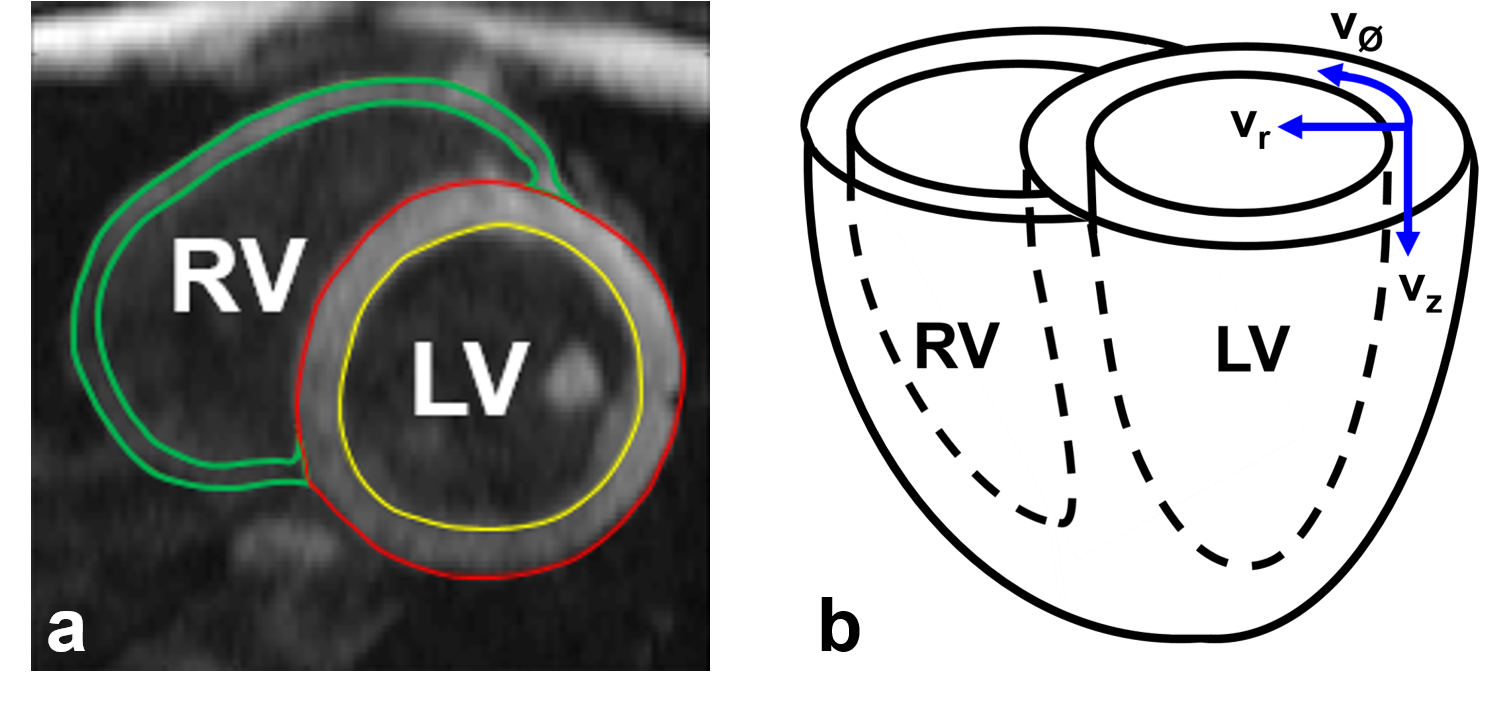
Figure
1. (a)
Manual determination of the LV and RV ROI for computing myocardial motion
velocity and kinetic
energy. (b) The illustration of myocardial radial (vr), circumferential
(vØ),
and
longitudinal (vz)
motion directions.
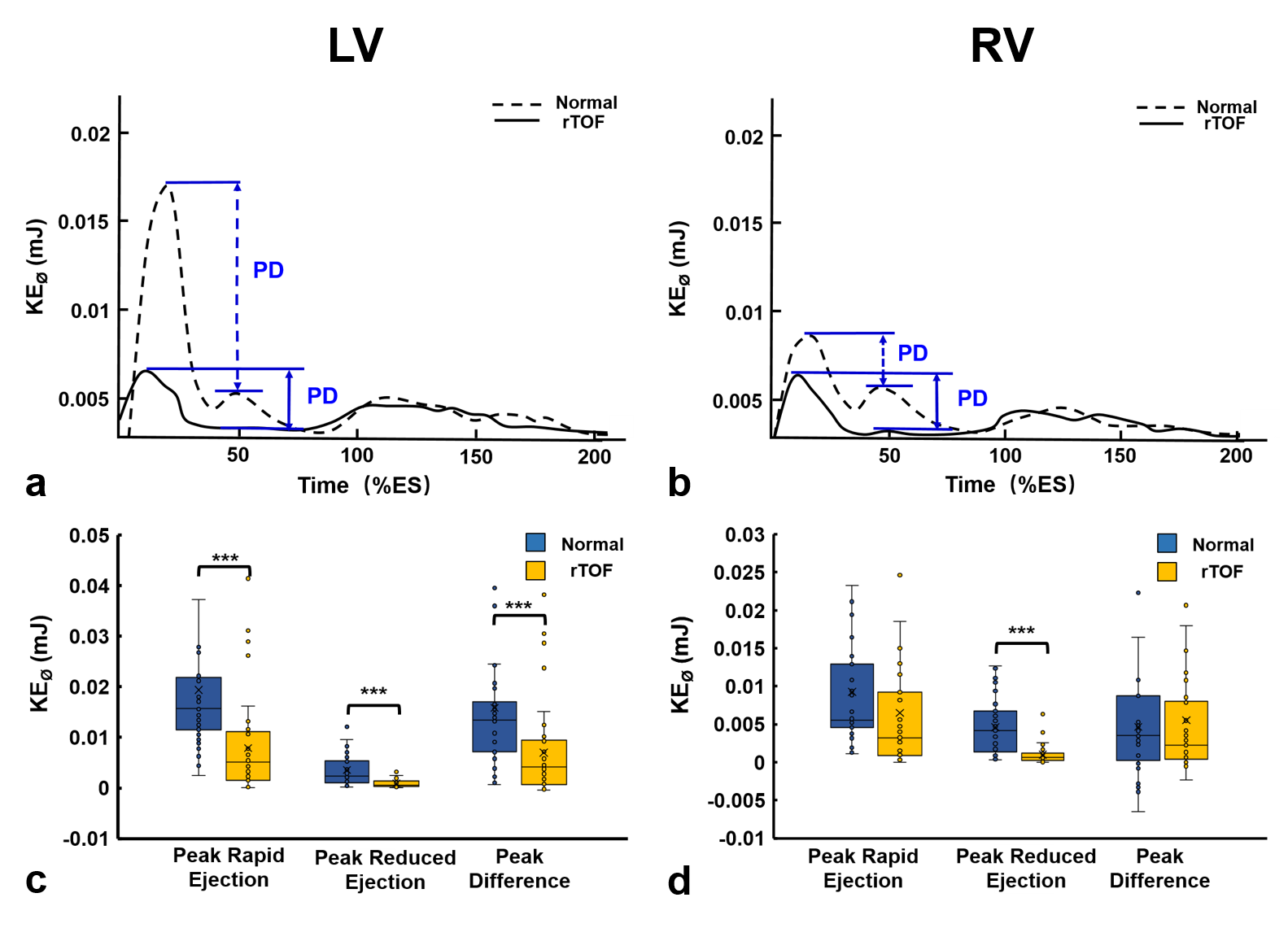
Figure
2. The
time courses of KEØ in LV
(a) and RV (b) of normal and rTOF groups. (c)
Compared to normal group, rTOF group presented lower peak
KEØ in
the LV at peak rapid ejection and peak reduced ejection phase and lower peak
difference (PD) in-between. In RV, rTOF group demonstrated lower peak
KEØ at peak reduced ejection (d). PD:
Peak difference (peak rapid ejection-peak reduced ejection). *P <
0.05, ***P
< 0.001.
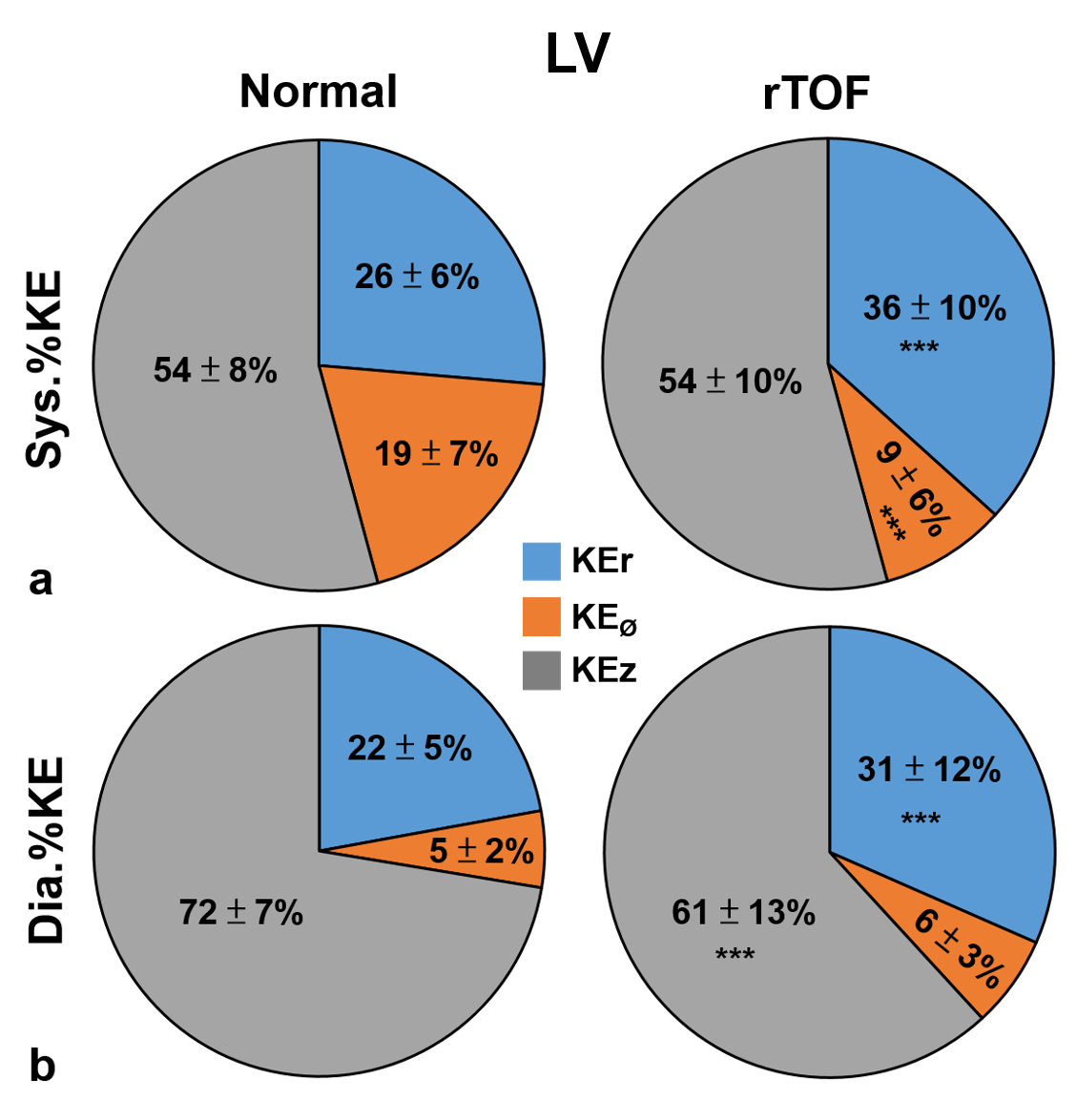
Figure
3.
The
proportions of myocardial KE of LV in radial (KEr), circumferential (KEØ), and
longitudinal (KEz) directions during systolic (a)
and diastolic (b) periods. ***P
< 0.001
compared to normal group.
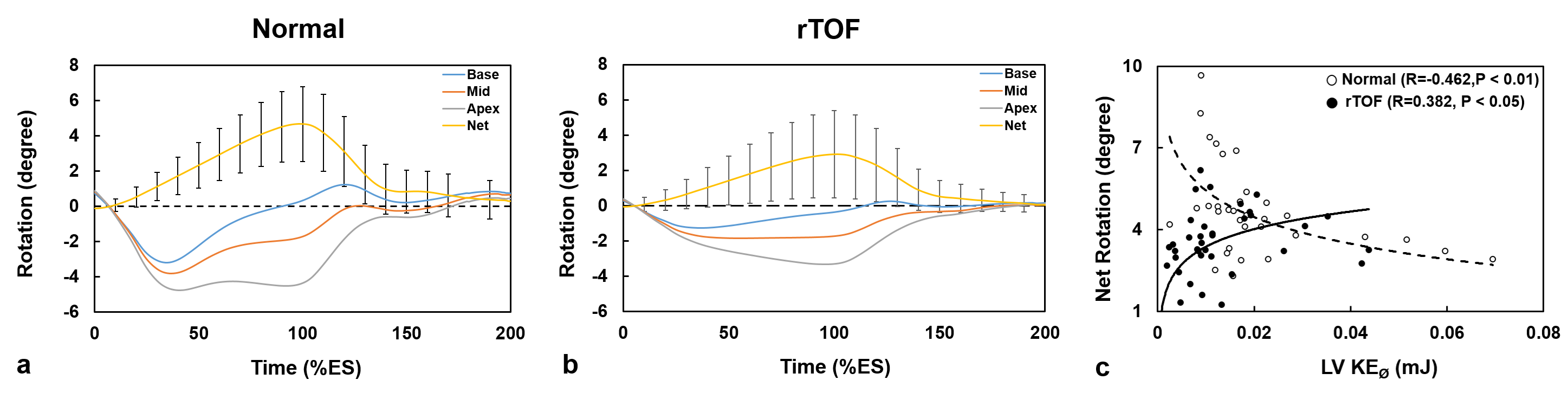
Figure 4. The
time courses of the rotation in basal, mid, and apical slice of normal (a)
and
rTOF (b)
groups. The net rotation represented the subtraction of basal rotation from
apical rotation. (c) The normal group presented negative correlation between
peak net
rotation and
mean LV
KEØ while
the rTOF
group showed positive correlation.