1196
Initial technical developments of local RF coil for sub-millimeter cardiovascular MRI.1IHU Liryc, Electrophysiology and Heart Modeling Institute, Fondation Bordeaux Université, Pessac, France, 2Univ. Bordeaux, Centre de recherche Cardio-Thoracique de Bordeaux, U1045, Bordeaux, France, 3Siemens Healthcare SAS, Saint-Denis, France, 4INSERM, Centre de recherche Cardio-Thoracique de Bordeaux, U1045, Bordeaux, France, 5IR4M, UMR8081, Université Paris-Sud/CNRS, Université Paris-Saclay, Orsay, France
Synopsis
In the context of cardiovascular diseases, precise determination of the extent and locations of the arrhythmogenic substrate could significantly improve diagnosis and treatment for both atrial and ventricular electrical diseases. However, the current spatial resolution and signal-to-noise ratio (SNR) in clinical scanners remain insufficient to provide relevant information of small structures like atrial wall or sub-millimeter fatty infiltration in ventricle. To address this limitation in SNR, two receiver coils were implemented at 1.5T for high resolution cardiac imaging, with different active decoupling techniques (safety aspects). Images at 200 µm in-plane spatial resolution were successfully obtained on a beating heart.
Introduction
Atrial and ventricular cardiac arrhythmias constitute the main cause of death worldwide. Using ex vivo MRI and histological validation, the extent of fibrosis was shown to be highly correlated with AF occurrence, severity and duration [1]. A precise description of the arrhythmogenic substrate could significantly improve the diagnosis of cardiovascular diseases in both atria and ventricles. However, the current spatial resolution and signal-to-noise ratio (SNR) in clinical scanners remain insufficient to provide relevant information, particularly for imaging small structures like the atrial wall (thickness ranging 2 to 5mm) or in presence of sub-millimeter fatty infiltrations in ventricles. To address the intrinsic limitation in SNR, several research groups proposed to use a local RF coil positioned close to the region of interest [2–4]. In this study, we developed small receiver coils interfaced with a clinical 1.5T MRI, using two active decoupling techniques based on electrical or optical approaches. Gains in SNR and spatial selectivity compared to conventional multi-element cardiac coils were measured on a phantom. 3D high-resolution images were obtained with the developed instrumentation on an ex vivo cardiac sample from sheep. Finally, preliminary results of high resolution MRI on ex vivo beating heart from pig are presented. Since in the context of arrhythmia, triggering on electrical activity is difficult, we also implemented a pressure sensor to trigger the acquisition on the mechanical status of the selected cardiac chamber to be imaged.Methods
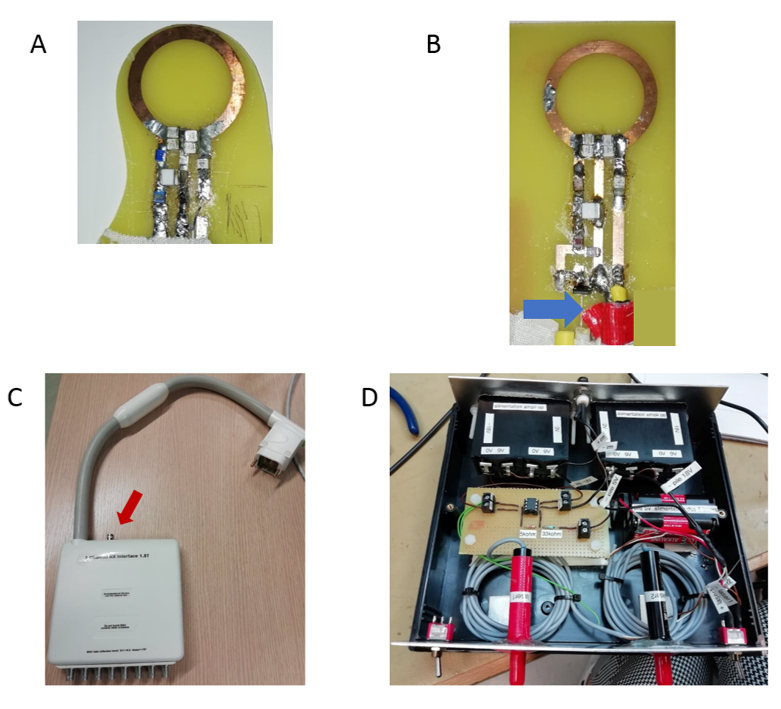
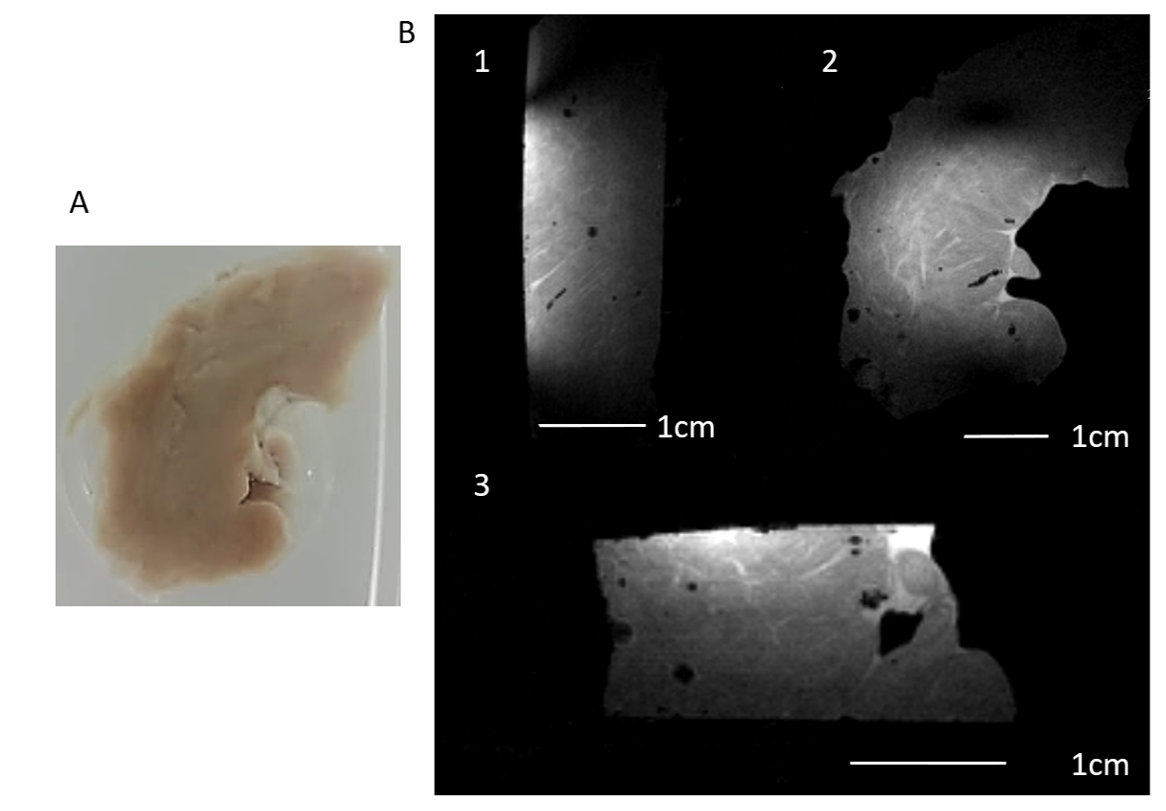
Two receive-only loop coils (2-cm in diameter) were built (35 µm-thick copper on a FR4 substrate). These coils were matched to 50 Ω and tuned to 63.6 MHz using capacitors and connected to an Aera 1.5T MR (Siemens Healthcare, Erlangen, Germany) with a dedicated interface box (figure 1.C). One coil was decoupled using conventional PIN diode driven by Direct Current (DC) while the second one was detuned using a photodiode (figures 1.A and 1.B) activated through a laser fiber driven by an homemade electrical-to-optical (25mW modulated laser diode, Laser Components, Germany, λ = 650 nm) conversion circuit (figure 1.D) [5]. The reflection coefficient modulus |S11| and Q factor were measured using a Vector Network Analyzer (VNA) when coils were loaded with a quality assurance phantom. SNR maps were measured on this phantom for both coils and compared to values obtained with the clinical 18 elements cardiac coil. Imaging parameters were: 2D Gradient Echo (GRE), TR/TE = 1041/4.41ms, TA = 50s, FA = 15°, pixel size = 1*1mm², thickness = 2.5mm, FOV = 200*200mm², BW = 293Hz/Px.3D 200µm isotropic resolution images were obtained using the galvanic detuned coil on an ex vivo sample of sheep septum fixed into formalin mixed with gadolinium (figure 3.A). Imaging parameters were: 3D GRE, TR/TE = 40/22ms, TA = 15min, FA = 33°, pixel size = 200µm3 isotropic, FOV = 80*50*22.4mm3, BW = 172Hz/Px.
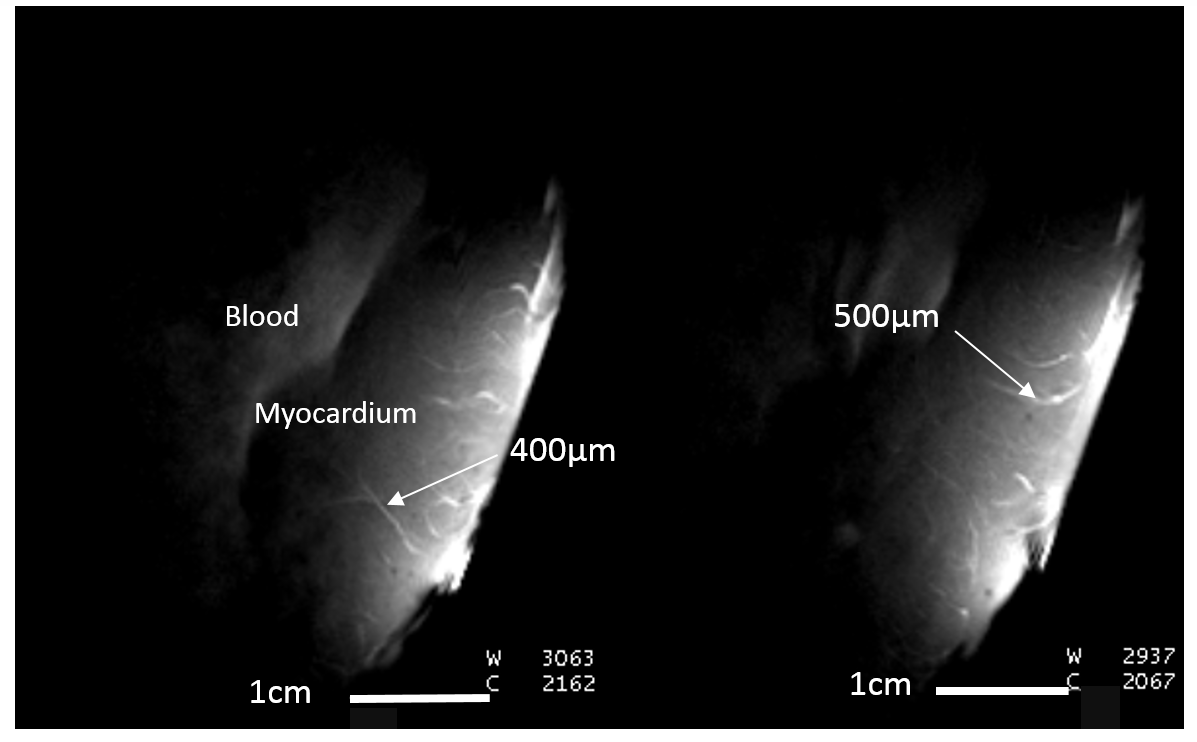
Beating heart (N=3, protocol approved by ethic committee) perfused in Langendorf mode [6] were imaged with the implemented coil for testing high resolution imaging in presence of motion. The local coil was placed in contact with the left ventricle wall using a home-made holder. Left intraventricular pressure was recorded using a small tubing inserted into the left ventricle connected to a recording system (Labchart, ADInstruments, Sydney, Australia). From these readings, a threshold was defined to generate a TTL signal that trigged MRI acquisitions on the diastolic phase. High resolution GRE images with reduced FOV were acquired with the following parameters: TR/TE = 162/25ms, A = 2min56’, FA = 60°, pixel size = 200*200µm², thickness = 2.5mm, FOV = 70*70mm², BW = 131Hz/Px.
Results
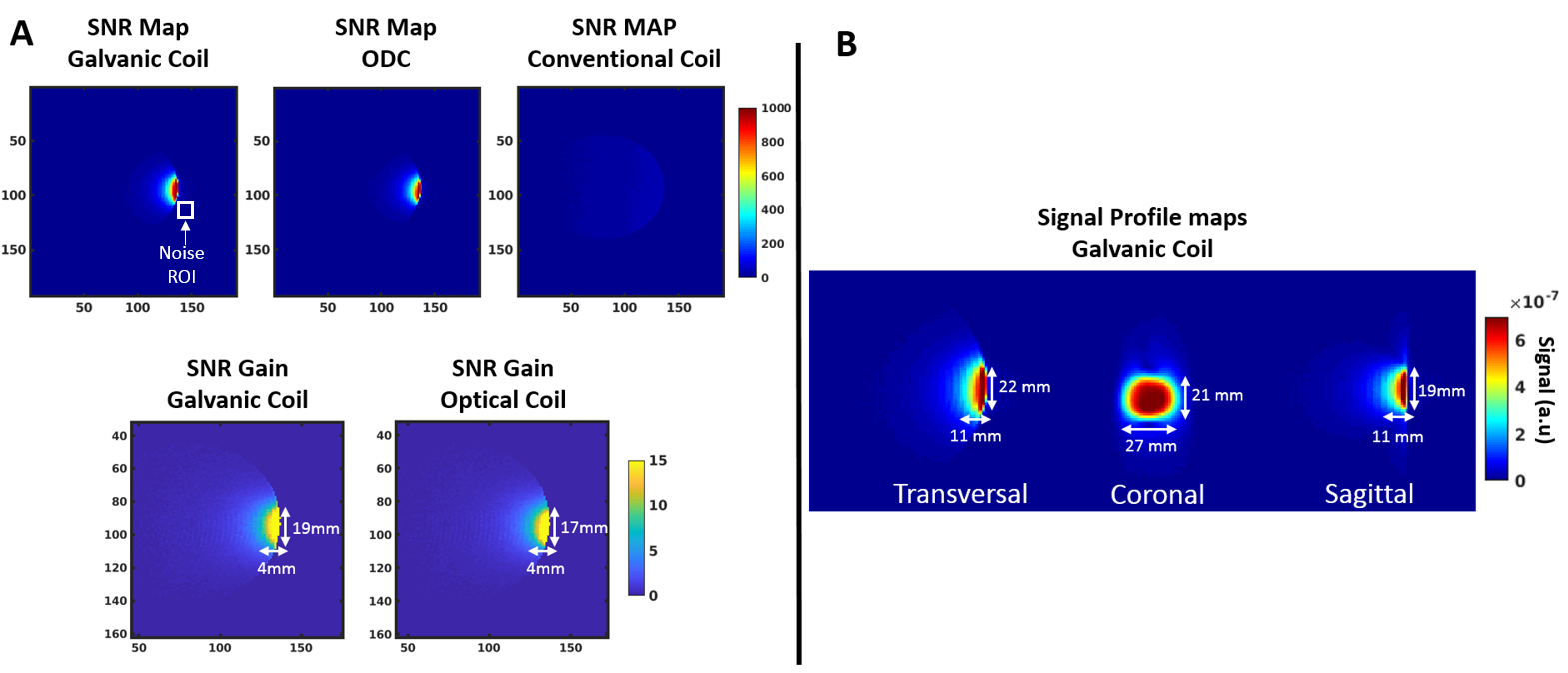
Matching of the two implemented coils was optimized to be lower than -20dB (|S11| = -23dB and -27dB for the galvanic and optical coils, respectively). Qloaded were 87 and 82 for the galvanic and optical coil, respectively. Decoupling was efficient and similar for both solutions. The measured SNR was higher than 1000 for both coils (figure 2.A). SNR gain with respect to the 18-element coil was higher than 15 for both loop coils, with similar performances whatever the detuning strategy. The signal profile was uniform over a 2*3*1cm3 (length*width*depth) region (figure 2.B) giving an adequate coverage for cardiac wall imaging (typically 2-5mm thickness for atrium and up to 15 mm for the ventricle). Successful 3D high resolution (200µm isotropic) images acquired on an excised septum revealed sub-millimeter structural details (figure 3B). On ex vivo beating heart from pig, the MRI sequences were successfully triggered on the intraventricular pressure, allowing acquisition of high-resolution images (200µm² in-plane resolution) and visualization of small vessels (figure 4).Conclusion and Discussion
The local loop coil allowed a significant increase in SNR with an achievable gain of 15 compared to a clinical chest coil. We demonstrate that optical detuning offers similar performances than conventional electrical decoupling, increasing safety in perspective of future catheter-based coil development (avoiding use of DC). We also demonstrate that intra-chamber pressure can be used to trigger the acquisition and results in high quality images. Combination of high sensitivity and limited spatial coverage using this implementation allowed to obtain images on conventional clinical MRI scanner with a higher spatial resolution than state-of-the-art cardiac imaging techniquesAcknowledgements
This work received financial support from the French National Investments for the Future Programs: ANR-10-IAHU-04 (IHU Liryc),Laboratory of Excellence ANR-10-LABX-57(Labex TRAIL) and ANR-11-INBS-0006 (France Life Imaging, Carcoi), Siemens Healthcare.
Helmut Stark is gratefiully thanks for technical support in coil interface.
References
[1]. Oakes RS, et al. Detection and Quantification of Left Atrial Structural Remodeling With Delayed-Enhancement Magnetic Resonance Imaging in Patients With Atrial Fibrillation. Circulation 2009;119:1758–1767
[2]. Volland NA, et al. Initial feasibility testing of limited field of view magnetic resonance thermometry using a local cardiac radiofrequency coil: Limited FOV MR Thermometry with Local Coil. Magnetic Resonance in Medicine 2013;70:994–1004.
[3]. Homagk A-K, et al. An expandable catheter loop coil for intravascular MRI in larger blood vessels. Magnetic Resonance in Medicine 63:517–523.
[4]. Schmidt EJ, et al. Intra-Cardiac MRI Catheter for EP Ablation Monitoring: Preliminary Studies. ISMRM 2011
[5]. Saniour I, et al. Active optical-based detuning circuit for receiver endoluminal coil. Biomedical Physics & Engineering Express 2017;3:025002
[6]. Vaillant F, Magat J, Bour P, et al. Magnetic resonance-compatible model of isolated working heart from large animal for multimodal assessment of cardiac function, electrophysiology, and metabolism. American Journal of Physiology-Heart and Circulatory Physiology 2016.
Figures