1192
Trigeminal nerve tractography with accelerated simultaneous multislice readout-segmented echo planar diffusion tensor imaging1Department of Diagnostic Radiology, Singapore General Hospital, Singapore, Singapore, 2Department of Neurology, National Neuroscience Institute – Outram Campus, Singapore, Singapore, 3Duke-NUS Medical School, Singapore, Singapore
Synopsis
The impact of simultaneous multi-slice imaging (SMS) with short repetition time (TR) accelerated acquisition on diffusion tensor imaging (DTI) combined with readout-segmented echo planar imaging (RESOLVE) on the intra-cranial nerves is unexplored. Compared to non-SMS RESOLVE-DTI, two SMS RESOLVE-DTI protocols showed higher pontine signal-to-noise ratio (SNR). Consistent measures of different DTI metrics of cisternal trigeminal nerves across the three RESOLVE-DTI protocols and significant positive correlations of mean DTI metrics in pairwise comparison across these suggest that SMS RESOLVE-DTI allows fast and reliable evaluation of the microstructural integrity of the cisternal trigeminal nerve, with possible utility in trigeminal neuralgia.
Introduction
Diffusion tensor imaging (DTI) tractography of the cranial nerves is challenging due to high susceptibility and geometrical distortions at the skull base.1 Readout-segmented echo planar imaging (RESOLVE) improves this2, but increased scan time limits its clinical application. Simultaneous multi-slice imaging (SMS) with short repetition time (TR) accelerates DTI acquisition3; however, its impact when combined with RESOLVE is unexplored. Our objective was to evaluate the reliability and reproducibility of trigeminal nerve tractography using SMS with RESOLVE-DTI.Methods
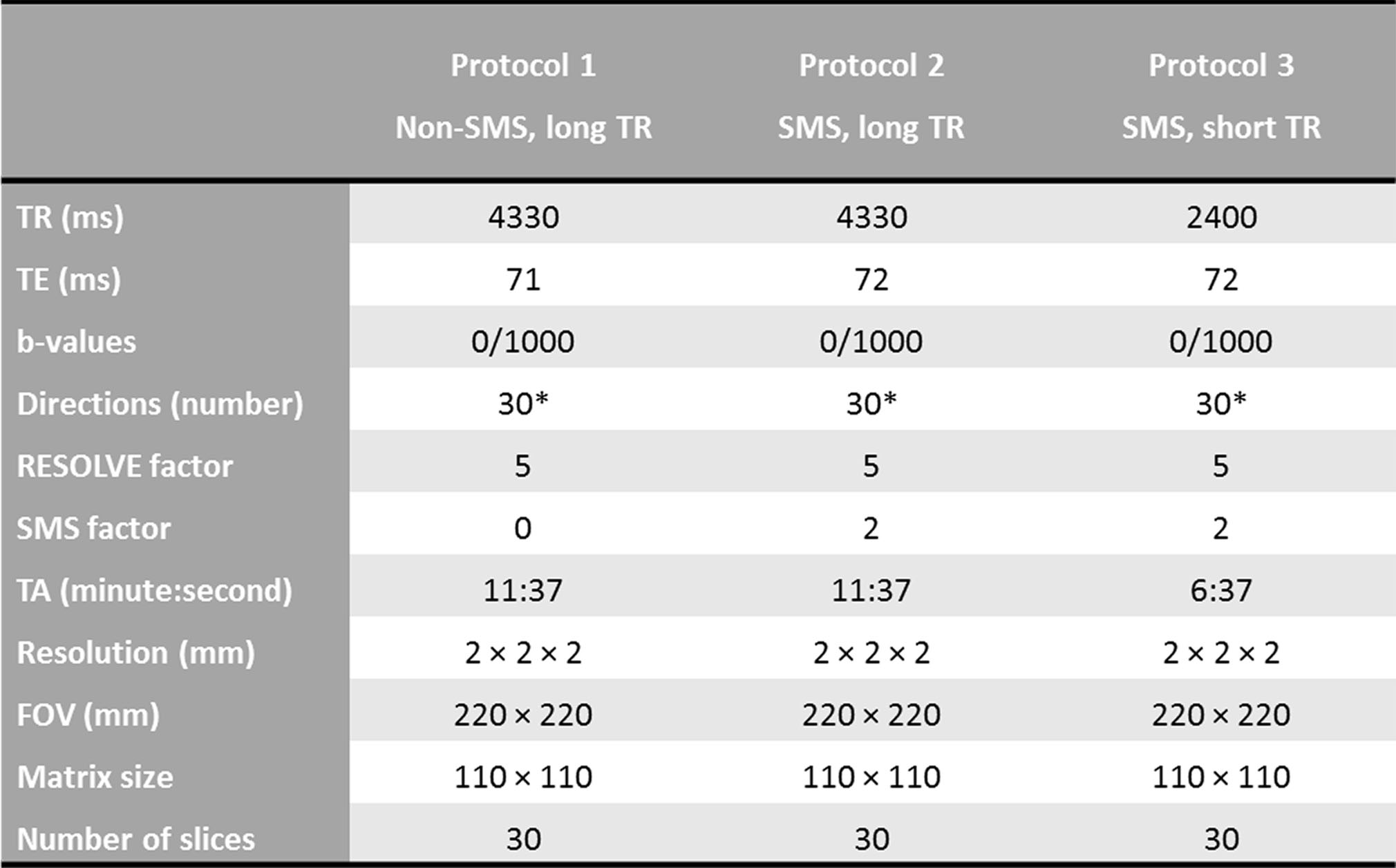
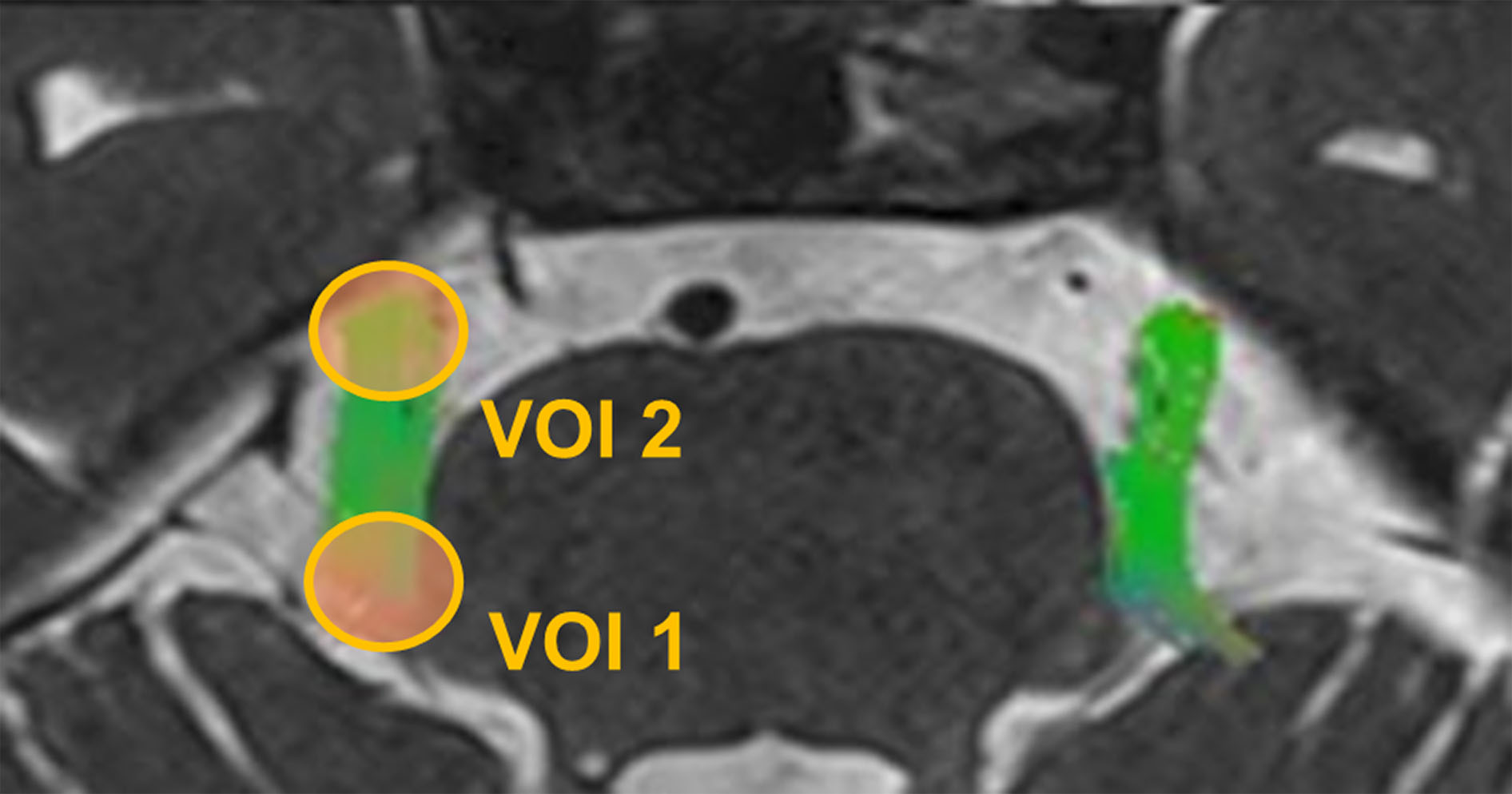
Eight healthy controls (HC) and six patients with unilateral trigeminal neuralgia (TN) were scanned on a 3T MR scanner (Skyra, Siemens, Erlangen) using a 32-channel head coil. Axial three-dimensional T2 SPACE sequence (TR/TE = 1000 ms/131 ms, flip angle = 120o, FOV = 160 x 160 mm2, matrix size = 320 x 316, slice thickness/gap/number = 0.5 mm/0 mm/64) and RESOLVE-DTI over the trigeminal nerves were obtained. Three different RESOLVE-DTI protocols were used (Table 1): non-SMS (TR = 4330 ms), SMS with identical TR (4330 ms), and SMS with short TR (2400 ms). The trigeminal nerves were tracked using deterministic tractography by placing two spherical volume of interest (VOI) seeds (Fig. 1). DTI metrics viz, fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), axial diffusivity (AD) were sampled along the coordinates of the trigeminal streamlines in the native space. We acquired three b0 images in each RESOLVE-DTI protocol, from which the difference image was derived from the latter two. To assess difference in image quality across the three RESOLVE-DTI protocols, voxel-wise quantitative signal-to-noise ratio (SNR) analysis was conducted using the following equation4:$$SNR=\frac{|SI|}{σ}\times\sqrt{2}$$
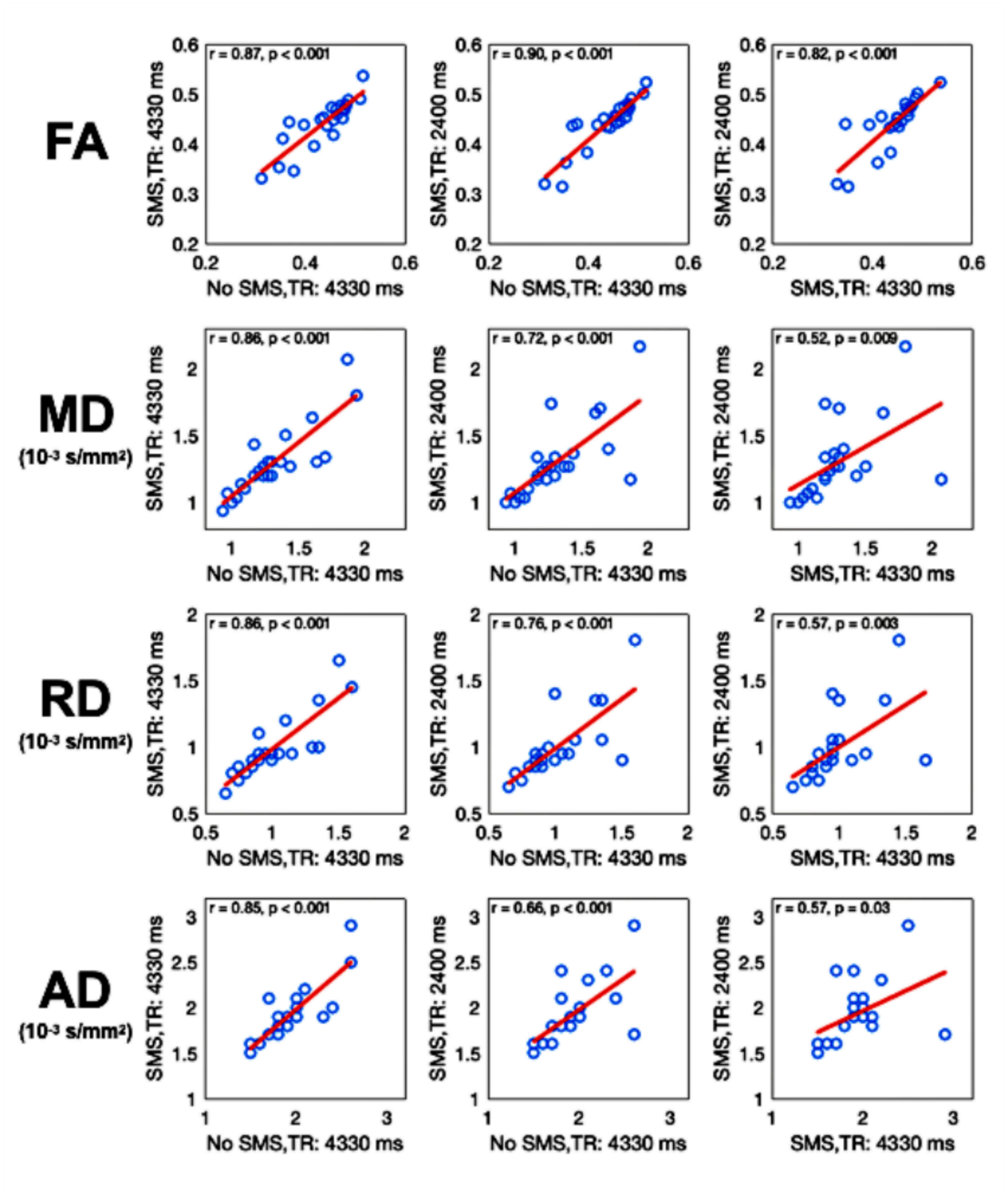
where SI is signal intensity of the first b0 image in a protocol, σ is the standard deviation of the difference image representing the noise component, and a correction factor.4 Pontine SNRs were compared across the three protocols using one-way analysis of variance (ANOVA) (Fig. 2A). Intra-rater and inter-rater intraclass correlation coefficients (ICCs) were employed to evaluate if the trigeminal nerve tractography was accurately and consistently produced by two MR technologists. Finally, two approaches were used to systematically evaluate the reliability and reproducibility of the DTI metrics of the trigeminal nerve streamlines: 1) one-way ANOVA for differences in mean FA, MD, AD and RD of the trigeminal streamlines amongst the three RESOLVE-DTI protocols; 2) Pearson’s correlation analysis for linear relationships between DTI metrics for each pair of the three RESOLVE-DTI protocols.
Results
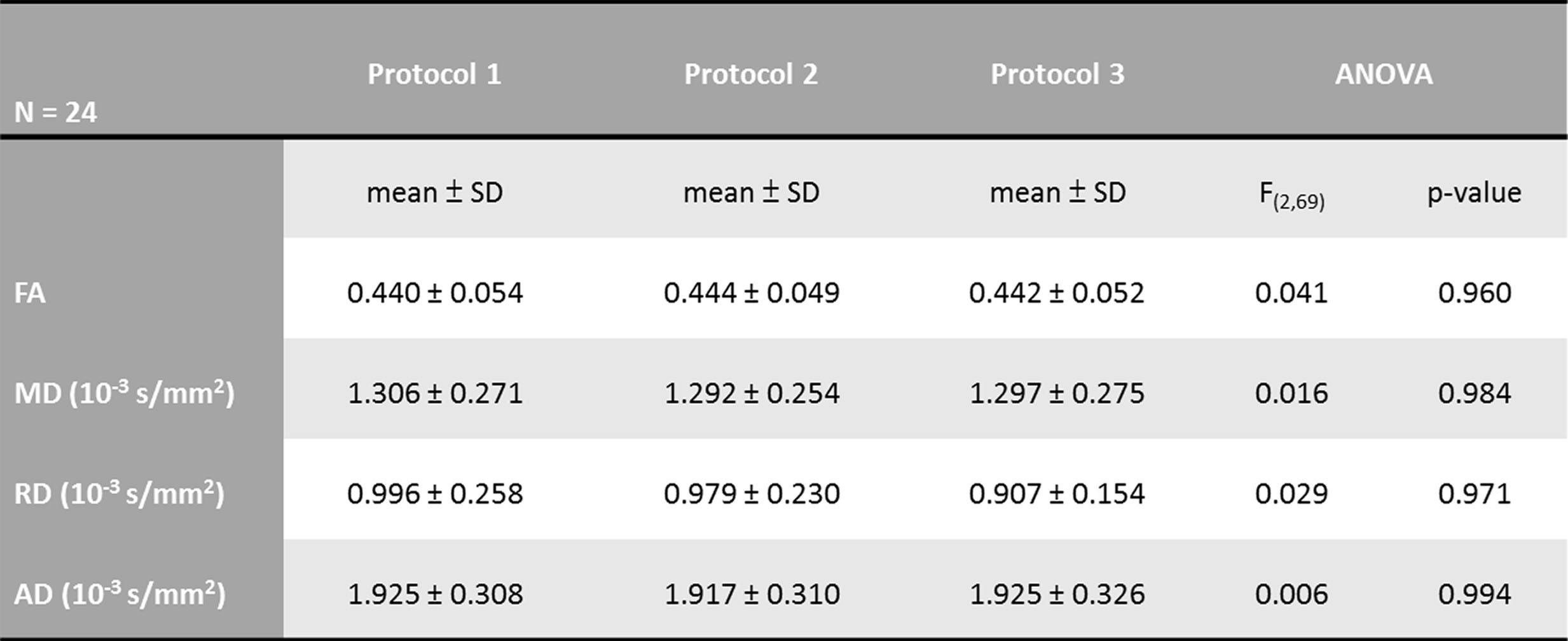
Of the 28 trigeminal nerves in all 14 participants, tractography was successful for 24 trigeminal nerves on all three RESOLVE-DTI protocols. Reliability of the tractography based on mean FA values within and between raters were good (intra-rater ICCs of HC: 0.926/0.956, intra-rater ICCs of TN: 0.884/0.856; inter-rater ICCs of both groups: 0.868 with 95% confidence interval of 0.729-0.937). Pontine SNR was similar for two SMS RESOLVE-DTI protocols but lower for non-SMS RESOLVE-DTI (F(2,36) = 37.22, p < 0.001, Fig. 2B). Post-hoc analysis revealed that the main effect was contributed by lower SNR in protocol 1 as compared to protocols 2 (p < 0.001) and 3 (p < 0.001). Mean values of various diffusion metrics (e.g., FA, MD, RD, AD) of the trigeminal nerves were consistently measured by the three protocols (Table 2). Furthermore, there were significant positive correlations of mean DTI metrics between each pair of the three protocols (p < 0.05, Fig. 3).Discussion
SMS RESOLVE-DTI with short TR showed significant acquisition time savings of 43% with an SMS factor of 2 and robust trigeminal nerve tractography. Compared to non-SMS RESOLVE-DTI, both SMS RESOLVE-DTI protocols showed more than two-fold increases in mean pontine SNR (Fig. 2B) and similar qualitative findings (Fig. 2C). Our DTI metrics along the trigeminal nerve streamlines were robust, with each DTI metric consistently measured and highly correlated across all three RESOLVE-DTI protocols. The reduced scan time arising from the blipped Controlled Aliasing in Parallel Imaging Result in High Acceleration (CAIPIRINHA) unaliasing technique implemented within SMS reduced the g-factor of reconstruction5 without significant loss in image quality. Our findings were similar to previous SMS RESOLVE-DTI studies on different organs,2,6,7 showing decreased scan time without a significant reduction in SNR and lack of significant change in our DTI metrics between non-SMS and SMS protocols. Higher pontine SNR in our SMS protocols might be enhanced by the CAIPIRINHA acquisition, providing more spin excitations and faster data acquisition within one TR.3Conclusion
We showed high reliability and reproducibility of trigeminal nerve tractography using two-fold-accelerated SMS RESOLVE-DTI, with improved image quality and robust quantitative DTI metrics, and potential clinical utility in trigeminal neuralgia.Summary of main findings
Two-fold-accelerated SMS RESOLVE-DTI acquisition showed significant acquisition time savings of 43%, improved image quality and robust trigeminal nerve tractography.Acknowledgements
This study was funded by the National Medical Research Council, Singapore, and the National Neuroscience Institute (NNI), Singapore, through the Pilot Studies Research Grant (grant number: NCG PV05). We express our appreciation to Siemens Healthineers Singapore, referring neurologists from the National Neuroscience Institute and team of MR Radiographers, physicists and research assistants in the Department of Diagnostic Radiology, Singapore General Hospital for their kind assistance and excellent support in this study.References
1. Skare S, Newbould RD, Clayton DB, et al. Clinical multishot DW-EPI through parallel imaging with considerations of susceptibility, motion, and noise. Magnetic resonance in medicine 2007;57(5):881-890. 2. Manoliu A, Ho M, Piccirelli M, et al. Simultaneous multislice readout-segmented echo planar imaging for accelerated diffusion tensor imaging of the mandibular nerve: A feasibility study. Journal of magnetic resonance imaging : JMRI 2017;46(3):663-677.
3. Barth M, Breuer F, Koopmans PJ, et al. Simultaneous multislice (SMS) imaging techniques. Magnetic resonance in medicine 2016;75(1):63-81.
4. Reeder SB, Wintersperger BJ, Dietrich O, et al. Practical approaches to the evaluation of signal-to-noise ratio performance with parallel imaging: application with cardiac imaging and a 32-channel cardiac coil. Magnetic resonance in medicine 2005;54(3):748-754.
5. Setsompop K, Gagoski BA, Polimeni JR, et al. Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty. Magnetic resonance in medicine 2012;67(5):1210-1224.
6. Filli L, Piccirelli M, Kenkel D, et al. Accelerated magnetic resonance diffusion tensor imaging of the median nerve using simultaneous multi-slice echo planar imaging with blipped CAIPIRINHA. European radiology 2016;26(6):1921-1928.
7. Boss A, Barth B, Filli L, Kenkel D, et al. Simultaneous multi-slice echo planar diffusion weighted imaging of the liver and the pancreas: Optimization of signal-to-noise ratio and acquisition time and application to intravoxel incoherent motion analysis. Eur J Radiol 2016;85(11):1948-1955.
Figures