1187
Multi-parametric diffusion tensor imaging for early detection of dysthyroid optic neuropathy during thyroid-associated ophthalmopathy1Radiology, Guangdong Second Provincial General Hospital, Guangzhou, China, 2Radiology, The Affiliated Tongji Hospital, Tongji Medical College, Huazhong University of Science & Technology, Wuhan, China
Synopsis
Dysthyroid optic neuropathy (DON) is the most serious complication of Thyroid-Associated Ophthalmopathy(TAO). Untimely and ineffective treatment of could lead to permanent blindness. Early detection is the principle factor for timely intervention. Diffusion tensor imaging(DTI) is a noninvasive tool to reveal microstructural or non-overt damage and quantify pathological processes of nerve fiber bundle. We applied the multi-parametric of optic nerve to identify the DON from TAO. The result reveals that DTI can be considered a useful and noninvasive tool to differentiate DON from TAO with higher accuracy.
Introduction:
Dysthyroid optic neuropathy (DON), the most severe and vexing complication of TAO, can lead to irreversible blindness if treated untimely and ineffectively. In clinical practice, overwhelming majority of TAO patients may be unaware of the danger until the onset of pronounced visual loss. Thus, early diagnosis is critical for timely intervention of DON. Many examinations have been used auxiliary to diagnose DON. The ophthalmologic psychophysical tests are subjective and require the full cooperation of an alert and motivated patient. The electro-physiological tests, such as visual evoked potentials (VEP), are readily influenced by poor patient compliance and factors unrelated to the disease such as the opaque media, incorrect refraction[1] and often render false positive results. Peripapillary optical coherence tomography(OCT) can reflect the structural changes of optic nerve, but it is limited to the retinal. In short, existing methods cannot effectively detect the DON. In short, the ophthalmic signs or symptoms-based evaluations are neither invariably present nor specific for diagnosis. Therefore, identification of typical presenting features is vital for prevention the risk of permanent visual compromise. Muscle indices measured on conventional MRI or CT are frequently used to detect DON[2], however, this method was established on the undetermined pathology mechanism-the compression from enlarged EOMs. Furthermore, it is an indirect sign and limited to the intra-orbital part of optic nerve, fail to directly demonstrate the impairment of optic nerve and cannot accurately assess the underlying pathophysiology preceding the irreversible structural damage. Diffusion-tensor imaging (DTI) can sensitively detect the microstructural alterations in nerves[3] by quantifying microscopic motion of the water molecules within nerve fibers. It has been widely employed on human’s visual pathway related disease, including glaucoma, multiple sclerosis,optic neuritis to evaluate the nerve fibers. So far, DTI was just applied to assess the optic nerve in TAO patients without DON[4]. Therefore, we aimed to assess the axonal architecture of the optic nerve on DTI and use it to identify TAO patients with and without neuropathy. Thereby, providing data-based evidence for early detect DON.Methods:
This single-center retrospective study was approved by local institutional review board, and the requirement for informed consent was obtained. 56 TAO patients and 23 DON patients were included in the study. Clinical features of 79 patients and DTI parameters of the optic nerve of 158 orbits were analyzed. The area under receiver(AUC) operating characteristic curve was employed to evaluate the diagnostic performance of DTI parameters. The correlations between these DTI parameters and the clinical features were determined.Results:
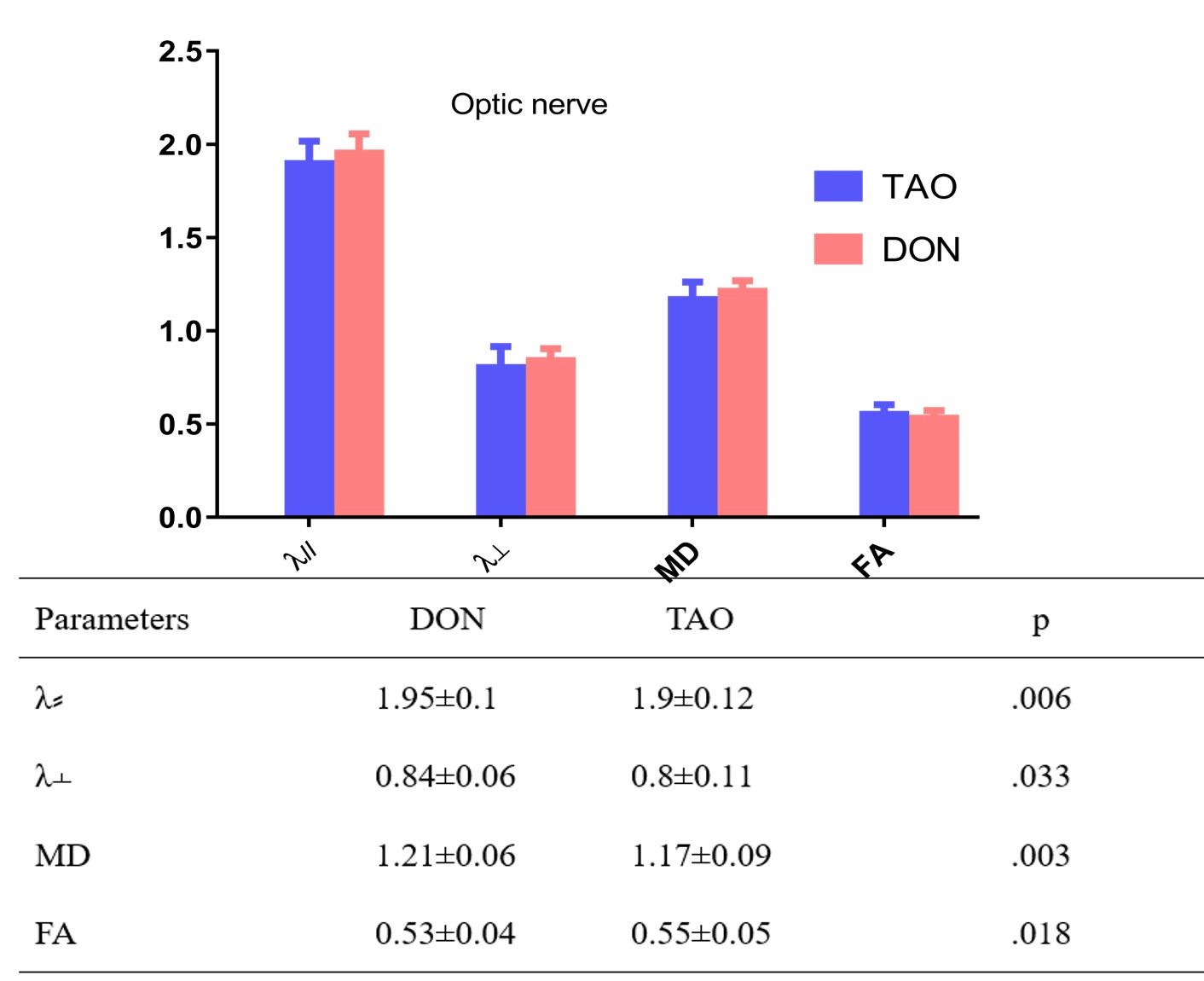
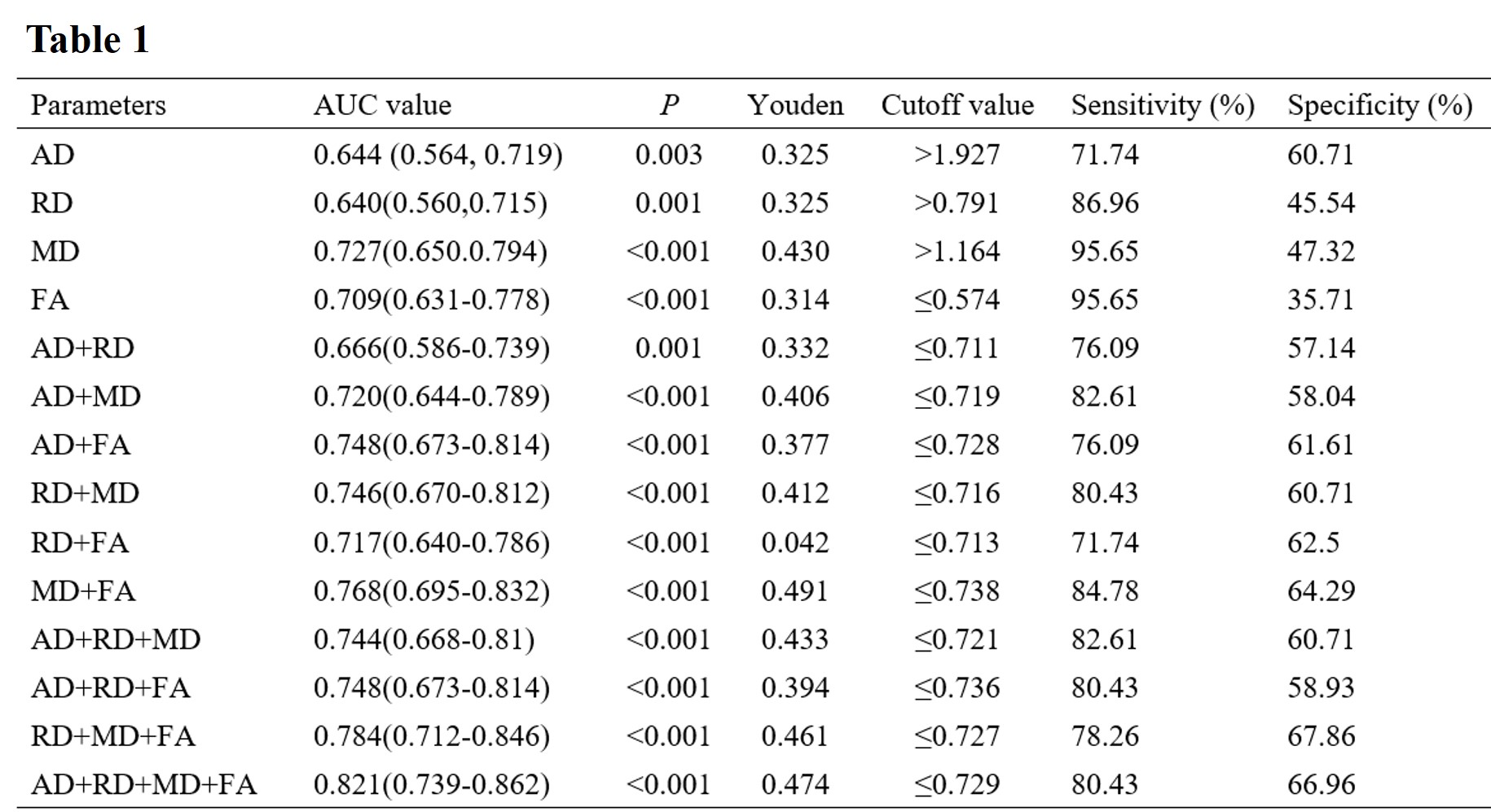
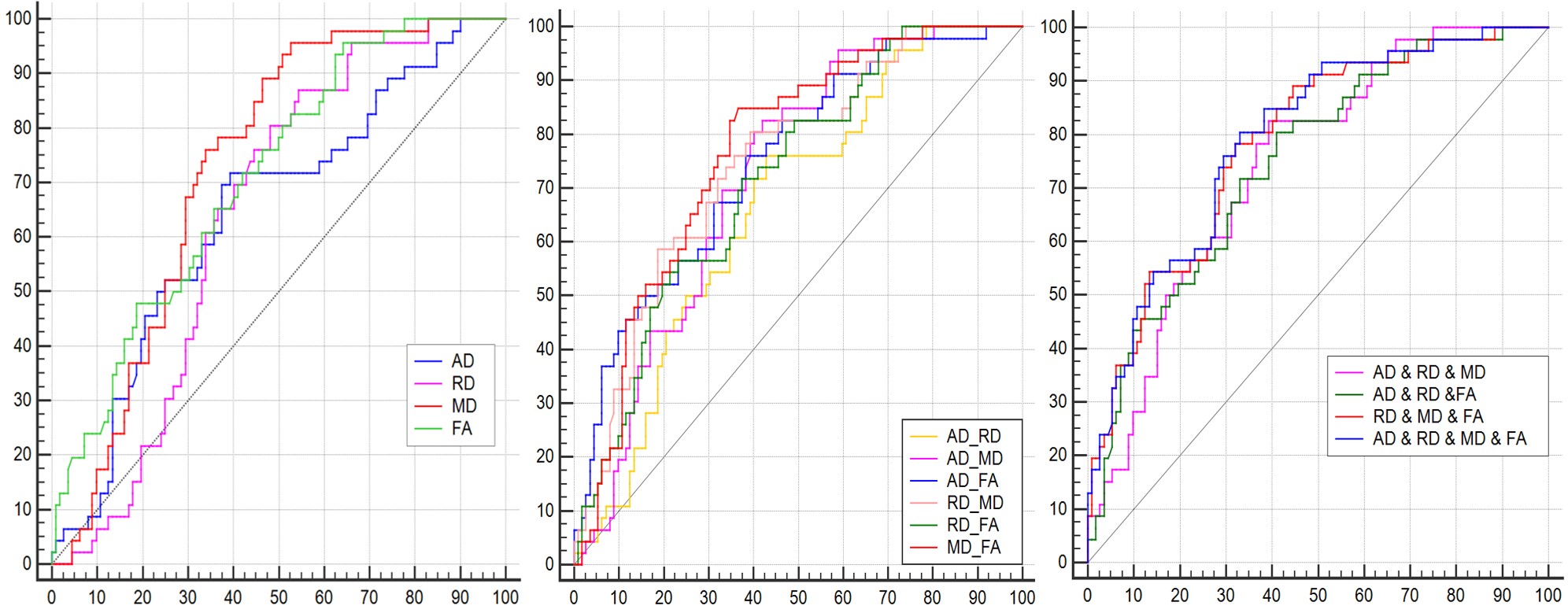
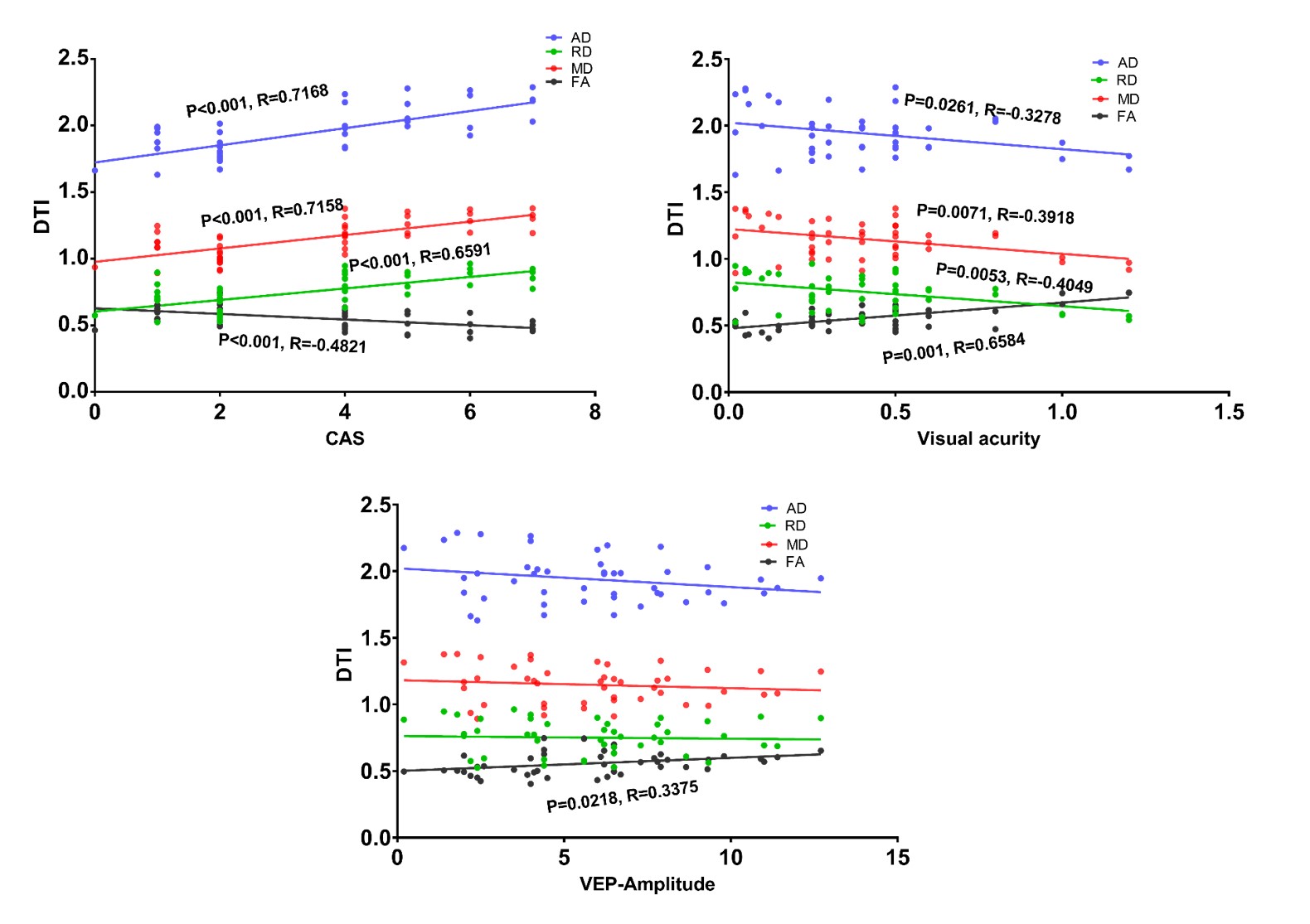
Compared to patients without TAO, DON patients showed higher levels of serologic TGAb, higher CAS, decreased visual accuracy and delayed latency time. As shown in Fig.1, the DON group displayed significantly higher λ⸗, λ﬩, MD and lower FA values than that of TAO(p<0.05, respectively). For identify DON from TAO, the MD and FA have the higher AUC(AUC=0.727,0.709,respectively), combination of the DTI parameters have added diagnostic performance, especially the combination of the four parameters generated the highest AUC (0.821) and corresponding sensitivity and specificity were 80.43% and 66.96%, respectively (Table 1 and Fig 2). There was significant correlation of the CAS, VA with all DTI parameters. The VEP amplitude also correlated with the FA of optic nerve (Fig 3).Discussion
DON begins in an insidious way and requires prompt diagnosis and treatment to prevent blindness. Existing diagnostic means are complex and cannot effectively and sensitively detect its occurrence until the onset of obvious and irreversible visual function.The optic nerve damage in DON have been confirmed by a cadaveric study[5]. We applied the DTI to observe the microstructural changes of optic nerve and attempted to use multiple parameters for the detection of DON. This study found that all diffusion parameters of the optic nerve changed markedly in DON patients. MD reflects the magnitude of the diffusion tensor and associates with demyelination or glia cell impairment.FA measures the orientation coherence of diffusion and fiber integrity and mirrors fiber attenuation, axonal diameter, and myelination in white matter. We conjecture that complex and diverse pathogenic mechanism including optic nerve ischemia or axonal flow inhibition from the compression of swelling extraocular muscles(EOMs), optic nerve stretching from increased soft-tissue volume, and inflammation (optic neuritis) may jointly induced the alterations of optic nerve.
With regard to the relationships between the clinical measures and DTI metrics,.The CAS represents the activity of TAO, higher scores means the disease is in inflammatory stage, increased λ⸗, λ﬩, and MD reflected the enhanced water diffusion, this suggested the inflammation-mediated optic neuritis may play a role in the neuropathy, that maybe the reason why large dose methylprednisolone is recommended as the first-line therapy for DON.
Conclusion
The correlation between DTI parameters of optic nerve and ophthalmic test suggests that these parameters may play a role as disease indicators. The diagnostic performance of DTI for identification DON from TAO mean the DTI may act as an imaging marker for the prediction of the DON during TAO. This study facilitates the management of DON.Acknowledgements
Thanks for the subjects inclued in this research.References
1.M.D. Tsaloumas, P.A. Good, M.A. Burdon, G.P. Misson, Flash and pattern visual evoked potentials in the diagnosis and monitoring of dysthyroid optic neuropathy, Eye (London, England) 8 ( Pt 6) (1994) 638-45.
2.L. Barrett, H.J. Glatt, R.M. Burde, M.H. Gado, Optic nerve dysfunction in thyroid eye disease: CT, Radiology 167(2) (1988) 503-7.
3.P.J. Basser, C. Pierpaoli, Microstructural and physiological features of tissues elucidated by quantitative-diffusion-tensor MRI, Journal of magnetic resonance. Series B 111(3) (1996) 209-19.
4.H. Lee, Y.H. Lee, S.I. Suh, E.K. Jeong, S. Baek, H.S. Seo, Characterizing Intraorbital Optic Nerve Changes on Diffusion Tensor Imaging in Thyroid Eye Disease Before Dysthyroid Optic Neuropathy
5.T.J. Hufnagel, W.F. Hickey, W.H. Cobbs, F.A. Jakobiec, T. Iwamoto, R.C. Eagle, Immunohistochemical and Ultrastructural Studies on the Exenterated Orbital Tissues of a Patient with Graves' Disease, Ophthalmology 91(11)
Figures