1186
2D ungated PC-MRI for the exploration of small vessels in head and neck vascularisation1CHU AMIENS-PICARDIE, AMIENS, France
Synopsis
2D ungated PC-MRI could be accurate enough to assess cervicofacial vascularization where vessels are often less than 4 mm in diameter but hey are sensitive to the pulsatile flow and their accuracy and precision should be evaluate. We have designed a phantom model to determine the better MRI parameters for pulsatile flow in pipes of one millimeter of diameter. 108 sequences have been tested and 2 were selected as accurate and precise even in case of high pulsatility. The duration of the acquisition was 15 second. 2D ungated sequences should be suitable for daily clinical practice in small vessels evaluation.
INTRODUCTION
Knowledge of the facial vascularization is really important for maxillo-facial surgeons. However, there is no examination to ensure both morphological and functional evaluation. 2D or 3D cine PC-MRI could be an option but remain time-consuming1. New fast MRI techniques, as EPI or k-t Blast, despite their evolution have a lack of accuracy and precision for smaller vessels under 4 mm of diameter. Furthermore 2D ungated PC-MRI sequences are a very interesting option for facial investigation because they are quick and seem accurate enough so the entire facial vascularization could be studied in less of thirty minutes. However their accuracy and precision for such small vessel and their sensibility to pulsatile flow should be determined because this type of sequences are very sensitive to pulsatility2,3,4. The objective of this phantom study was to evaluate accuracy and precision of 2D ungated PC MRI sequences with pulsatile flow for vessel of one millimetre of diameter.METHODS
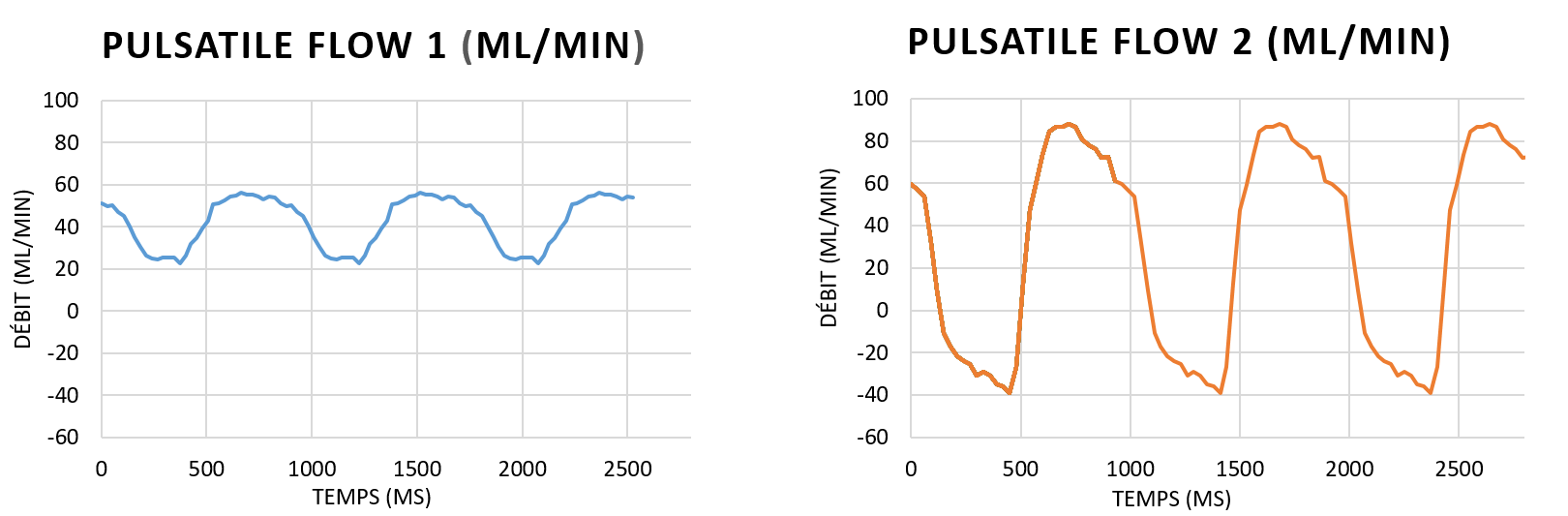
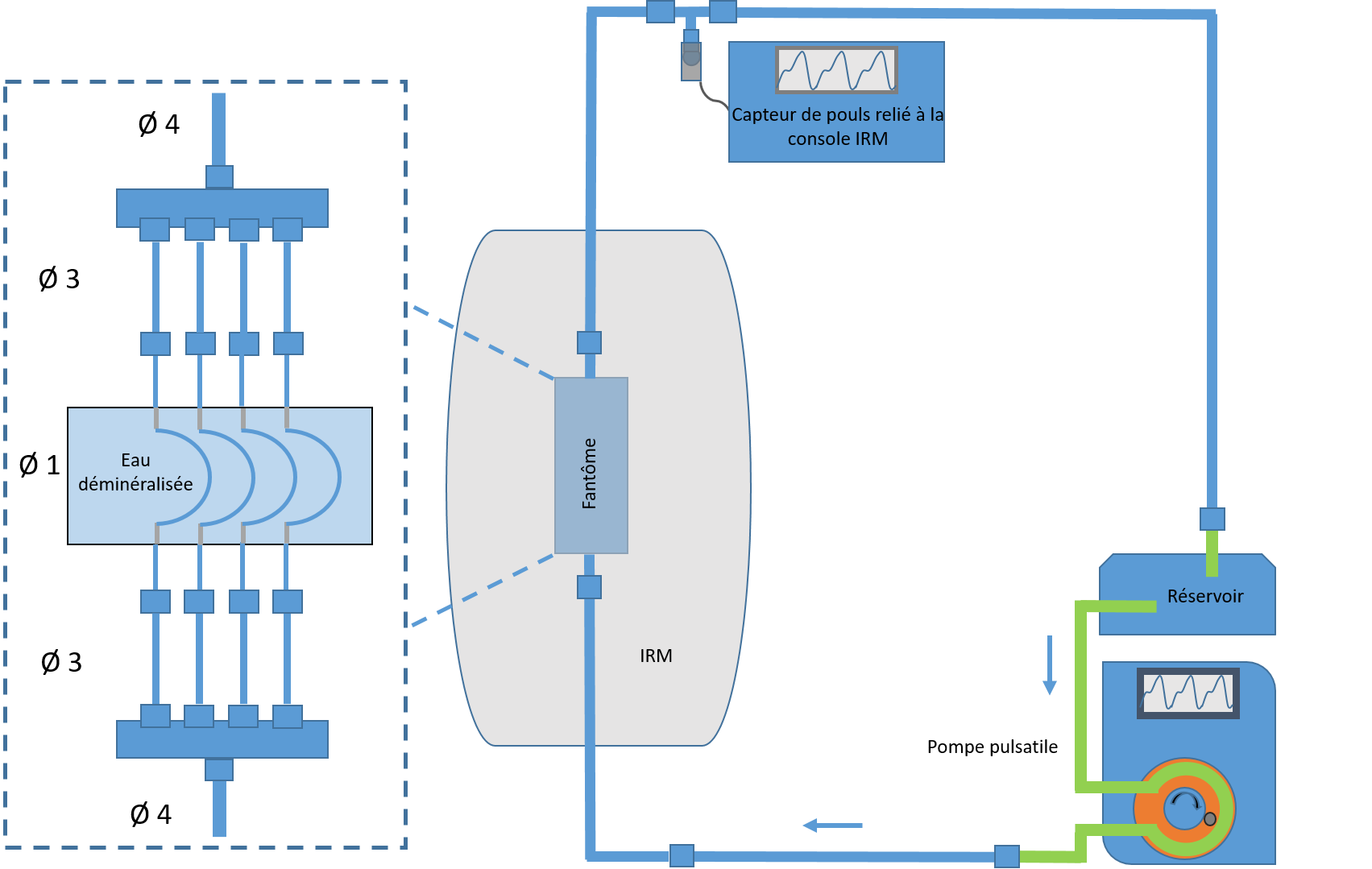
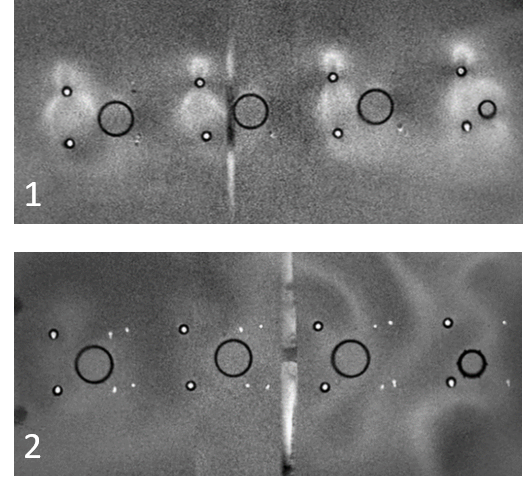
A phantom composed by four plastic pipes folded on themselves and of one millimetre of diameter was designed [Fig.1]. They were connected to a circuit with a pomp which was delivering a pulsatile flow of 50 ml/min. The fluid circulating was demineralized water. Two different pulsed flows were tested: the first one was weakly pulsatile with a monophasic curve and a resistance index of resistance of 0,78 (the same as facial vessels), the second one was stronger pulsatile with a resistance index of resistance of 1,09 [Fig. 2 and 3]. The measurement of total flow rate was realised manually to confirm the flow rate delivered to the circuit and a stationary flow was applied to confirm the hypothesis of flow rate conservation. Acquisitions were performed on a 3T IRM with head and neck coil. First, a 3D PCA was realised to choose the section plan. Then the following parameters were tested: resolution (0,2x0,2 mm and 0,3x0,3 mm), flip angle (10, 20 or 30°), number of signal average (NSA) (1,2 or 4) and slice thickness (1,2,3,4,5 or 6 mm), resulting in 108 different sequences. Every acquisition was repeated three times. The segmentation of the acquisitions was realised for every pipe to obtain values of mean area, mean velocity and mean flow of each tube for each sequence. 2D-cine PC-MRI were realised too, as the reference technique, for each acquisition. The accuracy (i.e. the degree of the given measurement agrees with the reference value) and precision (i.e. the level of agreement of a particular measurement with itself when it is repeated) of these measurements were analysed in relation to the reference values. The total flow rate rather than mean flow was used as reference value because it has been measured. The cut-off value chosen was 10 % around the reference value for both accuracy and precision. Furthermore, a model of logistic regression was realised for the flow measurements with the first pulsatile flow in order to analyse the better parameter configuration of the 2D ungated sequences.RESULTS
Flow conservation was established by measurements of mean entrance and exit flow in stationary flow. Of the 108 sequences performed with the first pulsatility regime, only 101 could be analysed due to the poor quality of the images. After analysing the accuracy and precision of the entrance and exit values for the total flow rate, mean velocity and mean surface area values, 11 sequences (10%) were selected and tested with stronger pulsatility. After further analysis, two sequences were selected with the floowing parameters: resolution 0.3x0.3 mm, NSA 2, slice thickness 6 mm and flip angles 20 and 30⁰ for an acquisition time of 15.6 seconds. The analysis of the weights of the logistic regression variables revealed the importance of the flip angle for all the selected parameters (p < 0.05). The NSA is particularly important for the accuracy of the values, while the slice thickness is more important for accuracy (p < 0.05).DISCUSSION
The selected sequences remain stable even under conditions where arterial pulsatility could be increased. They thus allow, without injection of contrast medium, a reliable and repeatable measurement of vascular flow. Available on all MRIs, they do not require the purchase of additional sequences from the manufacturer. In the context of primary and secondary reconstructions of the cephalic extremity by free flaps, it could allow a preoperative morphological identification of the recipient vessels and making it possible to evaluate the functional evaluation of these vessels. This application would be of fundamental interest in operated and/or irradiated patients with impaired cervico-facial vascularization, sometimes even to true "vascular deserts". This assessment could also be extended to the donor site to ensure the reliability of the pedicle vessels used for reconstruction, thus saving time and intraoperative safety.CONCLUSION
Non-synchronized MRI sequences should be considered as a new tool for visualization and quantification of cervico-facial vascularization, achievable in daily clinical practice. 2D ungated PC-MRI opens the way to a better understanding of head and neck arterial and venous blood flows, as well as to the evaluation of post-therapeutic vascular modifications.Acknowledgements
Gueules Cassées Foundation
Région Hauts-de-France
ANR-Equipex
Faire Faces Institute
CHIMERE TEAM 7516
References
1. Bettoni J, Pagé G, Salsac AV, Constans JM, Testelin S, Devauchelle B et al., Quantitative assessment of the flow distribution in the branches of the external carotid by non-injected flow MRI. Dentomaxillofac Radiol. 2018, 47-8
2. Bakker CJ, Hartkamp MJ, Mali WP, Measuring blood flow by nontriggered 2D phase-contrast MR angiography, Magn Reson Imaging, 1996.14:609-614
3. Bakker CJ, Kouwenhoven M, Hartkamp MJ, Hoogeveen RM, Mali WP, Accuracy and precision of time-averaged flow as measured by nontriggered 2D phase-contrast MR angiography, a phantom evaluation, Magn Reson Imaging, 1995, 13:959-965
4. Hangiandreou NJ, Rossman PJ, Riederer SJ, Analysis of MR phase-contrast measurements of pulsatile velocity waveforms, J Magn Reson Imaging, 1993, 3(2):387-94
Figures