1174
Effect of non-protonated perfluorocarbon liquid-filled SatPads on spinal cord MR imaging1Department of computer engineering and software engineering, Polytechnique Montreal, Montreal, QC, Canada, 2Montreal Neurological Institute, McGill University, Montreal, QC, Canada, 3Center of Precision Rehabilitation for Spinal Pain (CPR Spine), University of Birmingham, Birmingham, United Kingdom, 4NeuroPoly Lab, Institute of Biomedical Engineering, Polytechnique Montreal, Montreal, QC, Canada, 5Functional Neuroimaging Unit, CRIUGM, Université de Montréal, Montreal, QC, Canada
Synopsis
Acquiring high-quality functional MRI data of the spinal cord is challenging due to large susceptibility artifacts and high physiological noise, causing signal dropout and distorsions, particularly in the cervical region. This study demonstrated the beneficial effect of using non-protonated perfluorocarbon liquid-filled SatPadsTM during fMRI acquisition. Indeed, results show an increase of 31.51% for the global signal and 36.59% for the temporal signal-to-noise ratio for resting-state fMRI data acquired in the cervical spinal cord.
Introduction
Functional Magnetic Resonance Imaging (fMRI) of the spinal cord is challenging due to the large variability of cords’ shape and curvature. Moreover, fMRI data of the spinal cord is prone to high physiological noise and large susceptibility artifacts that cause signal dropout and distortion1,2. These artifacts can severely impact the analysis of fMRI data. Recently, a non-protonated perfluorocarbon liquid-filled technology (SatPadsTM), has been introduced as a fat-saturation and stabilization device for MRI, with the potential to improve the acquisition of cervical spinal cord MRI. This study aims at evaluating the effect of the SatPadsTM on the quality of fMRI data of the spinal cord.Methods
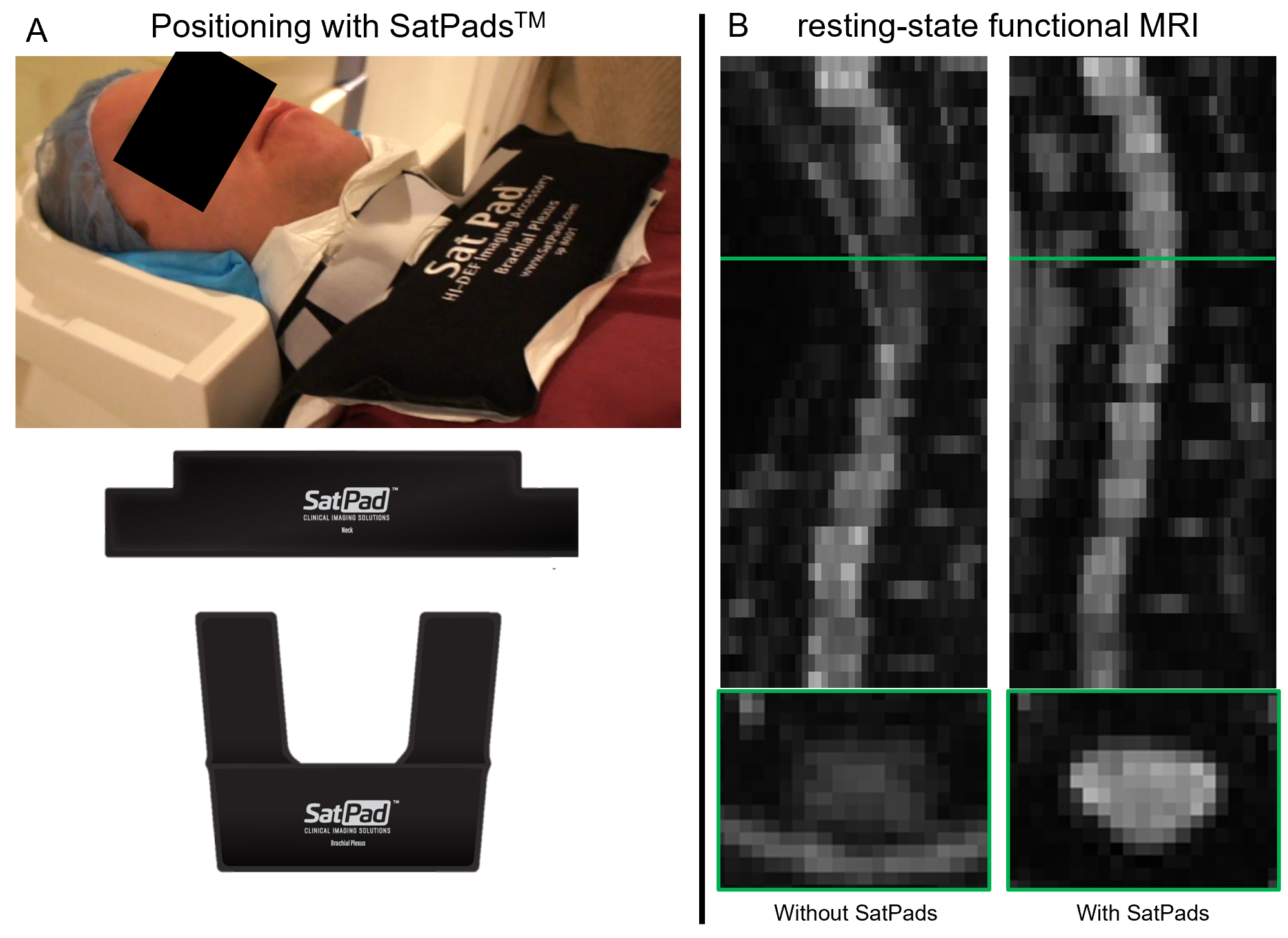
T1-weighted (T1w) and resting-state functional MRI (rs-fMRI) were acquired in 9 healthy subjects on a 3T Siemens Prisma fit scanner with a 64-channel head and neck coil, covering the brain and spinal cord from C1 to T2 vertebrae. All participants were scanned two times, with and without the Neck & Brachial Plexus SatPadTM set, with repositioning, as illustrated in Figure 1.A. The study was approved by the local ethics committees, and all participants gave their written informed consent. The acquisition parameters of the T1w magnetization-prepared rapid gradient echo (MPRAGE) sequence were: TR = 2,300 ms; TE = 3.31 ms; FoV = 320 × 320 mm; 176 slices, resolution=1.3x1.3×1.3 mm3. For rs-fMRI acquisitions, an echo-planar imaging (EPI) gradient-echo sequence was used with the following parameters: TR = 1,550 ms; TE = 23 ms; FA = 70°; FoV = 120 × 120 mm; matrix size = 64 × 64; slice thickness = 4.4 mm; in-plane resolution = 1.6 × 1.6 mm, parallel imaging with an accelerated factor of 3 and GRAPPA reconstruction, approximative acquisition time=155 sec.Preprocessing of the rs-fMRI images included (i) motion correction using a slice-wise regularized non-linear registration approach based on cross-correlation within a mask of the spinal cord and CSF available in SCT3, (ii) automatic spinal cord segmentation using PropSeg4, manually corrected when necessary, and (iii) registration of the fMRI images to the PAM50 template5 via the T1w image using a two-step non-linear deformation approach based on the spinal cord segmentation.
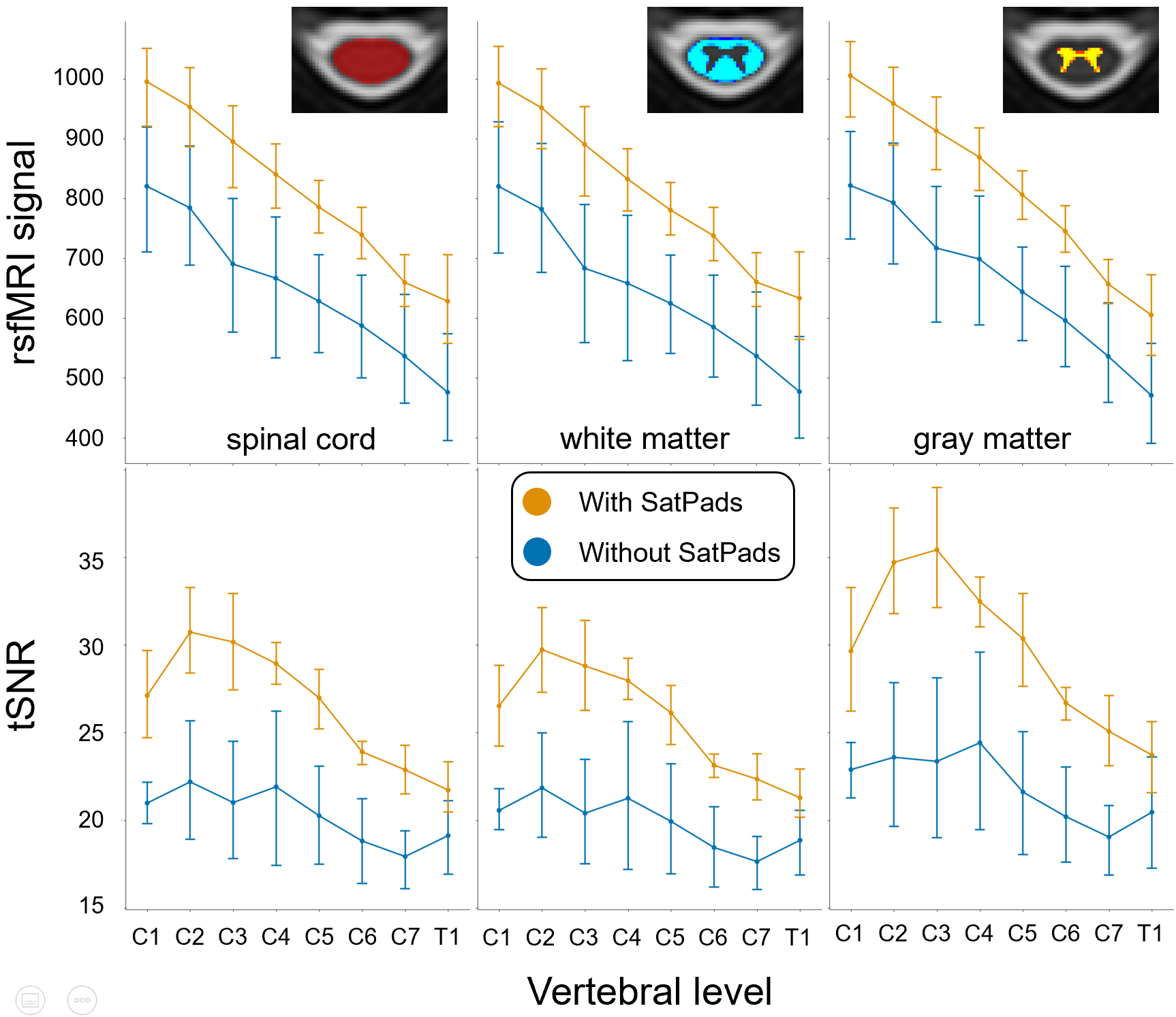
To evaluate the impact of the SatPadsTM on the rs-fMRI images, two comparison metrics (the rs-fMRI signal and the tSNR) were extracted over each vertebral level from C1 to T1 in the gray matter, in the white matter and in the spinal cord as a whole. The temporal signal-to-noise ratio (tSNR) for each voxel was calculated as the fMRI signal averaged over time divided by its standard deviation, after applying high-pass temporal filtering (sigma=100s) to avoid any low-frequency drifts. Paired statistical student t-tests were performed to evaluate the significance of the differences between the results with and without SatPadsTM for each of the metrics, with correction for multiple comparisons (⍺=0.0055).
Results
Figure 1.B illustrates the effect of SatPadsTM on the quality of rs-fMRI images, particularly at the C2-C5 vertebral levels. Figure 2 shows the global differences of rs-fMRI signal and tSNR between the images acquired with and without the SatPadsTM, within the spinal cord, the gray matter, and the white matter. In all cases, the results show a statistically significant increase (p<0.001) in both rs-fMRI signal and tSNR with the SatPadsTM. Examining the spinal cord as a whole, using SatPadsTM increases, on average, the rs-fMRI signal by 31.51% (range: 24.36-39.55) and the tSNR by 36.59% (range: 16.95-51.59).Discussion / Conclusion
Functional imaging of the spinal cord is challenging due to large susceptibility artifacts and signal dropouts, particularly in the cervical region. Improving the quality of fMRI images is an important step for the translation and standardization of such procedures in a clinical context. This study presents the evaluation of a new device, based on a non-protonated perfluorocarbon liquid, that aims at reducing the susceptibility artifacts and signal dropouts in the cervical spinal cord when acquiring fMRI data. The results demonstrate that using the SatPadsTM during the MR acquisition improves the quality of the fMRI images in the cervical spinal cord, by 31.51% for the fMRI signal and 36.59% for the temporal signal-to-noise ratio. These results may be explained by the reduction of the air-tissue interface proximity with the spinal cord at the cervical level, which is known to affect the fMRI signal in the spinal cord. Future work will include the evaluation of the effect of the SatPadsTM on other types of MR acquisitions, particularly on quantitative MRI data, such as diffusion-weighted imaging, magnetization transfer imaging, and T2*-weighted imaging, as well as their capabilities in reducing the patient’s motion during the acquisition.Acknowledgements
The authors would like to acknowledge all participants to the study, as well as the BIC (McGill University) and UNF (Université de Montréal) members who helped in the MRI acquisition. This study was supported by the Canada First Research Excellence Fund via the TransMedTech Institute, the Healthy Brain for Healthy Lives (HBHL) initiative, the NSERC Discovery Grant awarded to JD, and the Fondation Courtois.References
1. Wheeler-Kingshott CA, Stroman PW, Schwab JM, Bacon M, Bosma R, Brooks J, et al. The current state-of-the-art of spinal cord imaging: applications. Neuroimage. 2014 Jan 1;84:1082–93.
2. Stroman PW, Wheeler-Kingshott C, Bacon M, Schwab JM, Bosma R, Brooks J, et al. The current state-of-the-art of spinal cord imaging: methods. Neuroimage. 2014 Jan 1;84:1070–81.
3. De Leener B, Lévy S, Dupont SM, Fonov VS, Stikov N, Louis Collins D, et al. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage. 2017 Jan 15;145(Pt A):24–43.
4. De Leener B, Kadoury S, Cohen-Adad J. Robust, accurate and fast automatic segmentation of the spinal cord. Neuroimage. 2014 Sep;98:528–36.
5. De Leener B, Fonov VS, Collins DL, Callot V, Stikov N, Cohen-Adad J. PAM50: Unbiased multimodal template of the brainstem and spinal cord aligned with the ICBM152 space. Neuroimage. 2018 Jan 15;165:170–9.
Figures