1167
Axial T2*-Weighted Spiral MRI of the Spine at 1.5T1Phoenix Children's Hospital, Phoenix, AZ, United States
Synopsis
This study evaluates spiral as an alternative to Cartesian in axial T2*-weighted gradient echo imaging of the spine. SNR and CNR measurements were performed on spine data from a healthy volunteer. Expert reviewer ratings were also performed on data from 5 patients. Both the SNR/CNR measurements and reviewer ratings indicate that spiral can yield superior image quality without significant artifacts for a given scan time.
Introduction
Axial 2D T2*-weighted gradient echo (T2*GRE) imaging of the spine is valuable in the evaluation of spinal cord health and the identification of lesions. Its multi-echo variant (MERGE/MEDIC/mFFE) has shown higher sensitivity in the detection of spinal cord lesions compared to axial T2-weighted fast spin-echo (FSE/TSE) [1-2]. Gradient-echo images also suffer less CSF flow artifacts than T2FSE images [3]. Unfortunately, GRE sequences produce lower signal than T2TSE sequences, necessitating longer acquisition times, particularly at 1.5T. This study is an initial evaluation of axial T2*GRE spiral MRI as an alternative to Cartesian T2*GRE in the spine at 1.5T. It proposes that the signal-to-noise (SNR) to scan time advantage of spiral MRI will allow for shorter scan times while maintaining sufficient SNR for axial T2*GRE imaging in the spine.METHODS
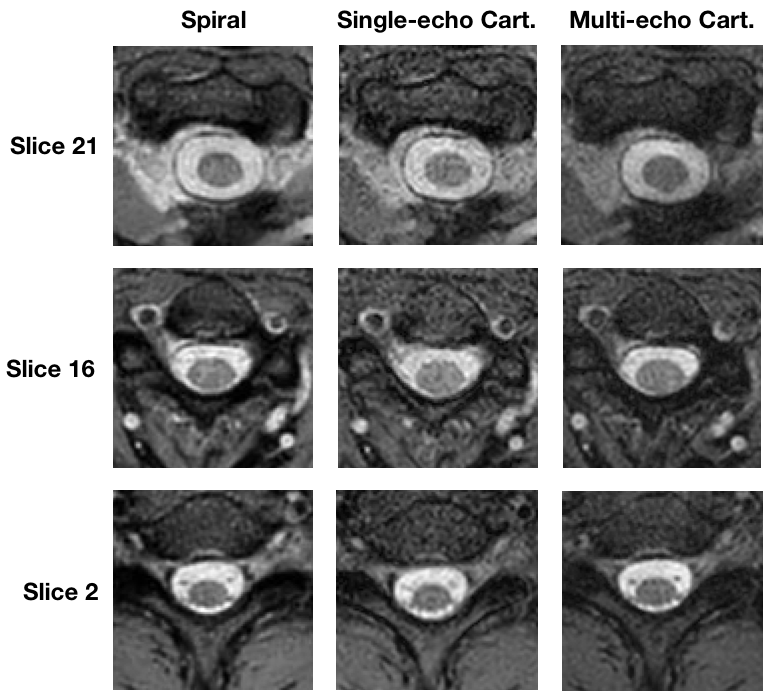
All data were collected on a Philips 1.5T system and were acquired in accordance with local IRB policy and following informed consent. The readout length of the spiral acquisition was set to 15ms. Fat suppression was accomplished using spectral pre-saturation with inversion recovery (SPIR) for the Cartesian sequences. Both single-echo and multi-echo Cartesian data (echoes = 3) were acquired. The spiral data were acquired at two echo times, and Dixon based fat/water separation was used to produce a water only image. Spatial saturation bands were positioned anterior to the spine to mitigate artifacts from motion.The following scan parameters were used for all acquisitions: FOV = 150 x 150 mm2, flip angle = 28, slice thickness = 4 mm, and slice gap = 0.4 mm. A 0.8 x 0.8 mm2 voxel size was used for the Cartesian data, while the spiral data made use of a 0.75 x 0.75 mm2 voxel size to partially compensate for the resolution loss from covering a circular rather than square area in k-space. All data were reconstructed using the vendor’s built-in reconstruction.
Spinal cord SNR was measured for spiral, Cartesian, and three-echo Cartesian T2*GRE data in the cervical spine of an adult volunteer. The contrast-to-noise ratio (CNR) between the CSF and spinal cord was also measured from the same data. Each scan was followed immediately by a noise only image acquisition accomplished by repeating the sequence with the gradient and RF waveforms turned off. Signal and noise measurements were taken from image regions corresponding to the spinal cord and CSF as appropriate. Root-mean-square combination of the echoes was first performed in the three-echo Cartesian data.
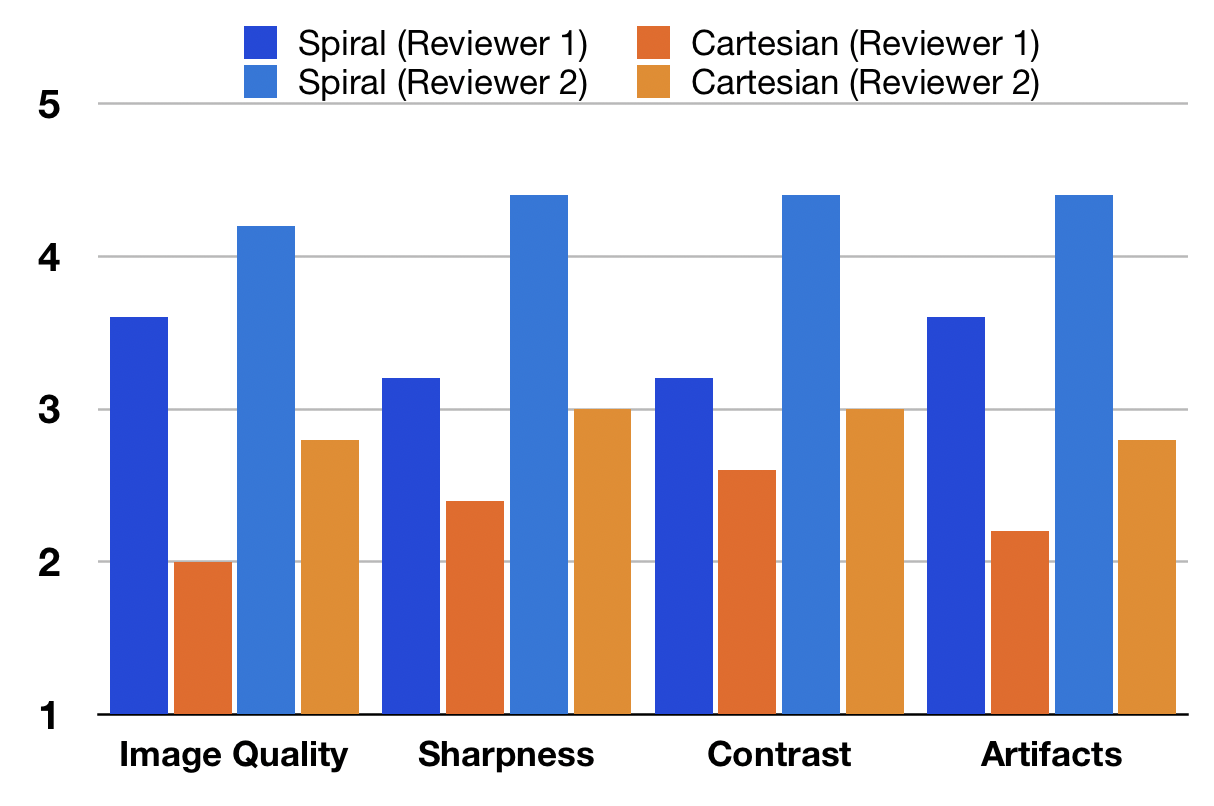
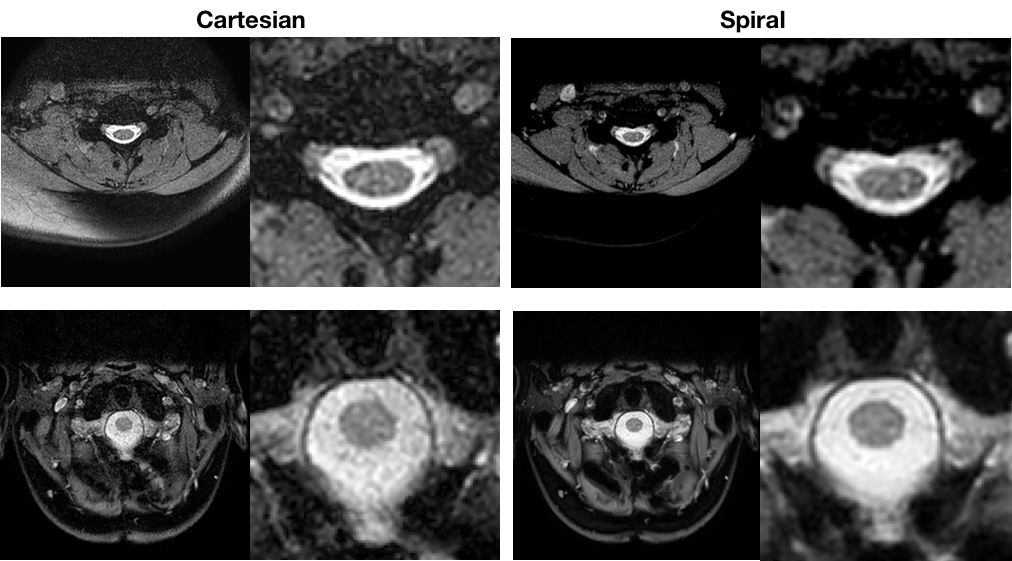
Spiral and single-echo Cartesian GRE data were acquired in the spine of five patients. Total scan time was matched between the spiral and Cartesian acquisitions. Two expert reviewers scored the image data from each patient based on overall image quality, sharpness, contrast, and level of artifact. Each image set was graded for these criteria on a scale of 1-5, with 1 being the worst and 5 being the best.
RESULTS
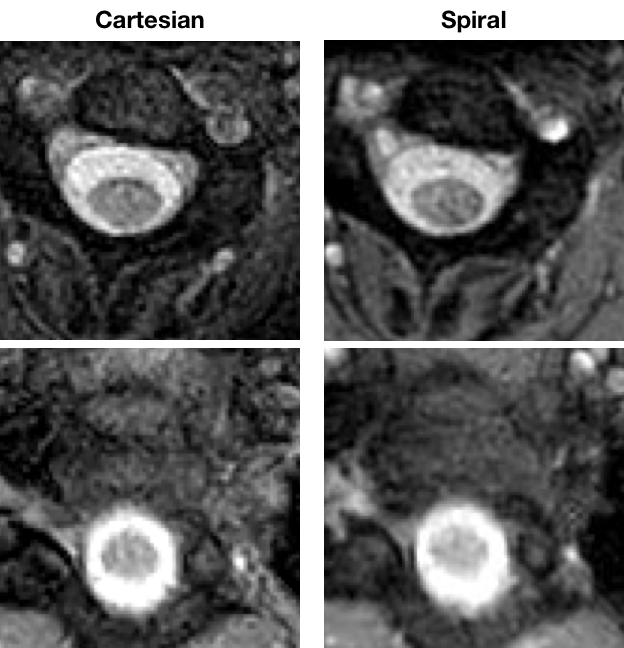
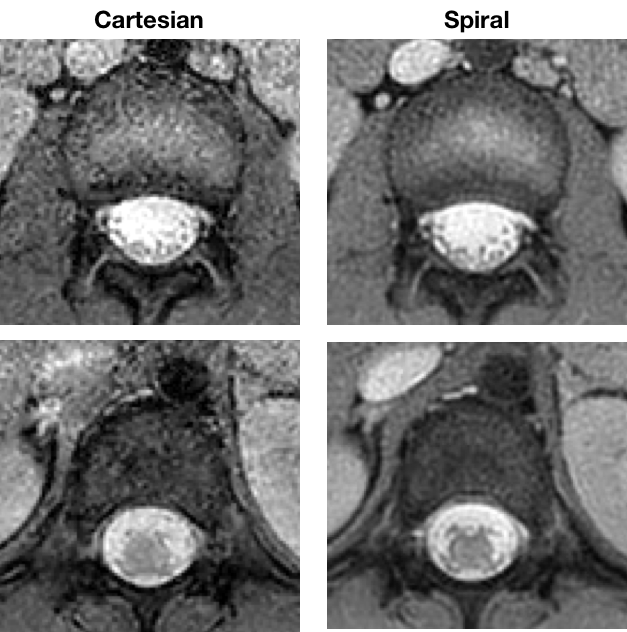
Three example slices from the 25 slice SNR measurement data are shown in figure 1. The SNR and CSF to cord CNR measurements were 26.8 and 14.1 for spiral, 16.2 and 10.6 for single-echo Cartesian, and 17.0 and 12.0 for multi-echo Cartesian. Mean reader rating scores taken across the five patients are shown in figure 2 for each of the rating criteria. Example images from three of the patients are shown in figures 3-5. The reviewers consistently rated the spiral data higher across patients and rating criteria. The one exception to this occurred in the patient corresponding to figure 4, in which one of the reviewers rated the sharpness and contrast of the Cartesian images slightly higher than the spiral images (3 vs 2). Both the spiral and Cartesian data for this patient received lower than average scores across reviewers and rating criteria.DISCUSSION
The SNR and CNR results demonstrate the signal to scan time efficiency benefit of the spiral acquisition. The higher SNR in the spiral acquisition contributed to a consistently higher perceived image quality by the image reviewers for the majority of the patients and rating criteria. Common artifacts that generally limit the utility of spiral such as off-resonance blurring and sensitivity to gradient errors were corrected in the image reconstruction and were not apparent in any of the data acquired for this study. These preliminary data suggest that the spiral data demonstrate good grey/white matter contrast in the cord, similar to that observed using multi-echo GRE sequences. This enhanced contrast may result in part because of the relatively long data readout in the spiral acquisition.CONCLUSION
This study suggests that spiral MRI could be a good alternative to single- or multi-echo Cartesian GRE for T2*-weighted imaging of the spine. As the number of patients studied was too small to present statistically significant results, further study is needed involving a larger number of patients.Acknowledgements
This work was supported in part by Philips HealthcareReferences
1. White M, Zhang Y, Healey K.Cervical spinal cord multiple sclerosis: evaluation with 2D multi-echo recombined gradient echo MR imaging. J Spinal Cord Med (2011); 34:93-98.
2. Martin M et al. Comparison of MERGE and Axial T2-Weighted Fast Spin-Echo Sequences for Detection of Multiple Sclerosis Lesions in the Cervical Spinal Cord. AJR (2012); 199: 157-162.
3. Katz HB, Quencer RM, Hinks RS. Comparison of Gradient-Recalled-Echo and T2-Weighted Spin-Echo Pulse Sequences in Intramedullary Spinal Lesions. AJNR (1989); 10:815-822.
Figures