1166
A ZOOM spiral TSE technique for spinal imaging1Neuroradiology, Barrow Neurological Institute, Phoenix, AZ, United States, 2Radiology, Phoenix Children's Hospital, Phoenix, AZ, United States, 3Philips Healthcare, Gainesville, FL, United States
Synopsis
Spine is a challenging area for MRI due to both anatomical features and motion. Spiral TSE has been proposed for spinal MRI. Aliasing in spiral spinal MRI is mitigated by combining oversampling with saturation band, with the latter not always achieving consistent and good signal suppression. In this work, the ZOOM technique has been incorporated into spiral TSE. Phantom and in vivo results demonstrate better signal suppression with ZOOM spiral TSE compared to spiral TSE acquired with a saturation band.
Introduction
Spinal imaging comprises a significant portion of routine neuro imaging. Most spinal MRI protocols include sagittal TSE scans (for T1, T2, or STIR contrast). Cartesian TSE spinal imaging often suffers from flow and motion artifacts. A spiral based TSE sequence has been proposed for spinal imaging. 1,2 In sagittal spiral imaging of the spine, in-plane oversampling is required to mitigate aliasing artifact as there is no distinct frequency and phase encoding directions. One concern with oversampling in spiral acquisition is that any motion, even outside the desired FOV, may be aliased into the image and manifested as incoherent artifacts. In previous work, a saturation band was used to suppress the signals outside the target FOV. 2 However, good suppression is not always achieved with a saturation band, resulting in residual signal outside the desired FOV that may degrade the image quality. The ZOOM technique, 3 combining oblique excitation/refocusing and saturation bands, has been demonstrated in EPI to reduce unwanted aliasing from signals outside the imaging FOV. In this work we implemented the ZOOM technique for spiral SE/TSE imaging with an elliptical FOV and verified it in sagittal T2 imaging of the spine.Methods
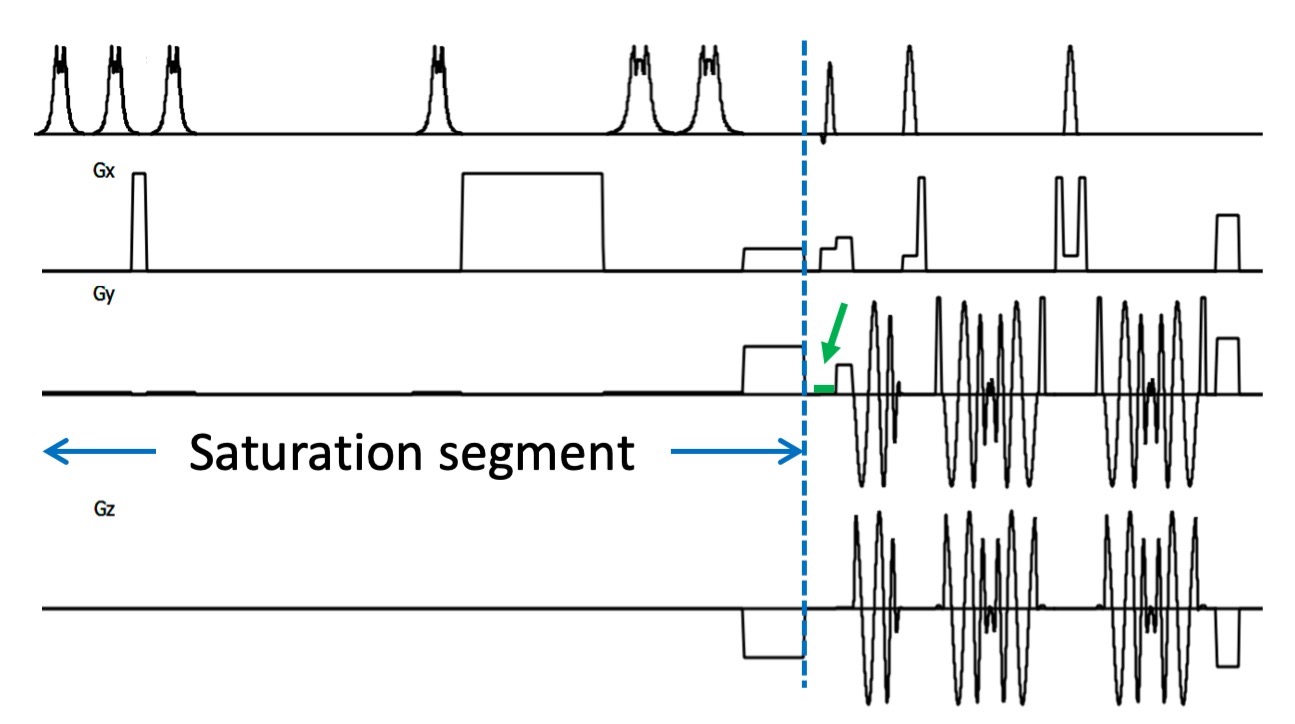
Due to the anatomic features of the cervical spine, an elliptical FOV is used in sagittal scans with the spiral TSE sequence. 2,4 The elliptical FOV in spiral imaging requires nominal phase encoding along the long axis (i.e., the foot-head direction) in spinal imaging to achieve a typical rectangular resolution, while the ZOOM technique requires phase encoding along the short axis (i.e., the anterior-posterior direction). This conflict is resolved by switching the axis of certain gradients to achieve signal suppression in the desired direction. The ZOOM technique is also made compatible with oversampling in spiral imaging. The schematic diagram is shown in Fig. 1.The ZOOM spiral TSE sequence was implemented on a 3T Philips Ingenia scanner (Philips Healthcare, Best, the Netherlands). Phantom and volunteer data were acquired with saturation band and the proposed ZOOM spiral TSE approach to demonstrate the improvement in suppressing signals outside the desired FOV. Scan parameters include: desired FOV = 120x240 mm2, prescribed FOV = 180x240 mm2 to match the resolution of corresponding Cartesian scan (0.65x0.87 mm2), oversampling factor = 1.3. Cartesian T2 TSE data with mDixon were also acquired with similar parameters.
Results
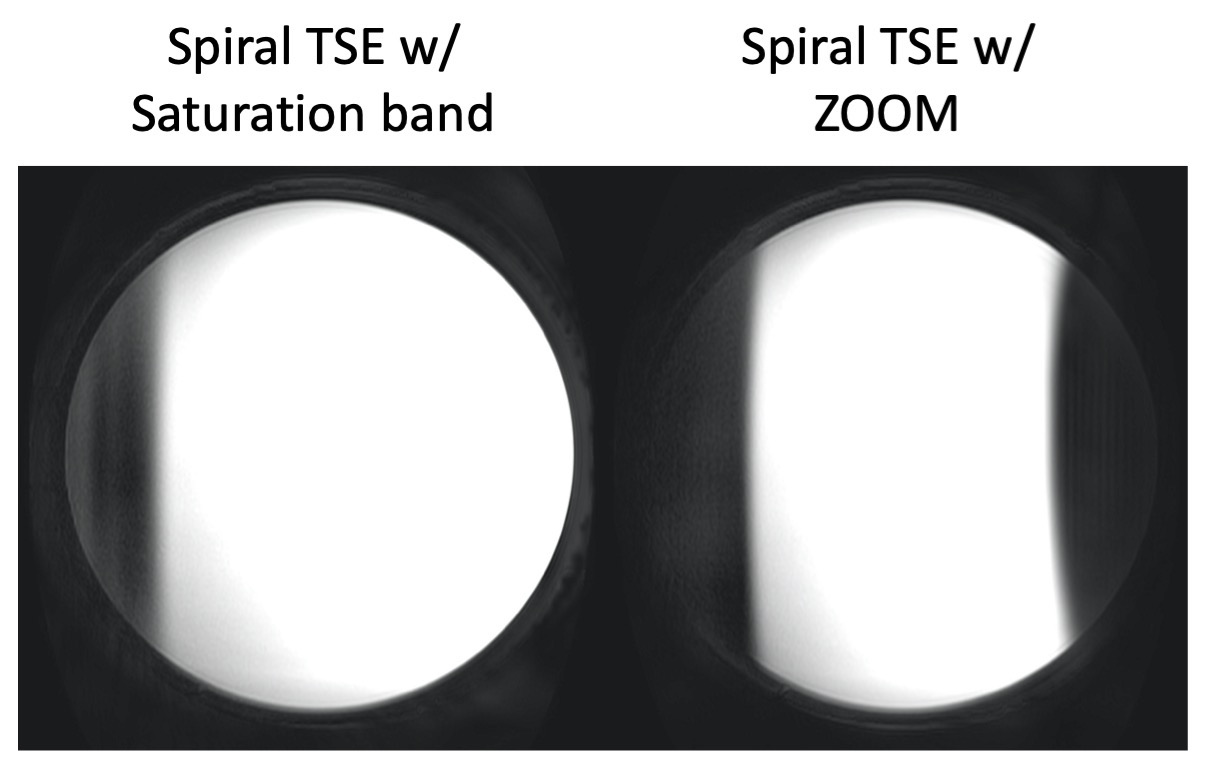
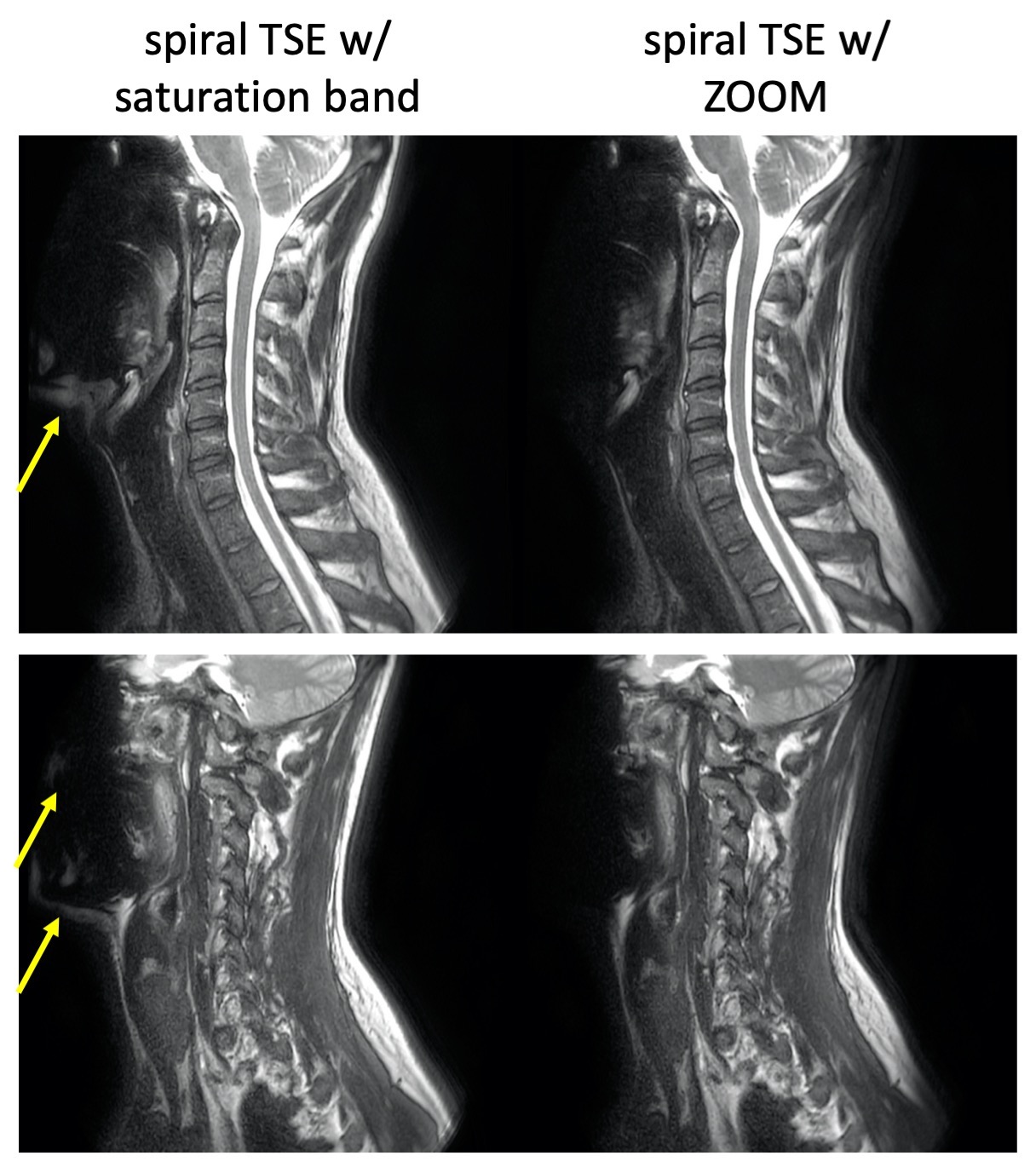
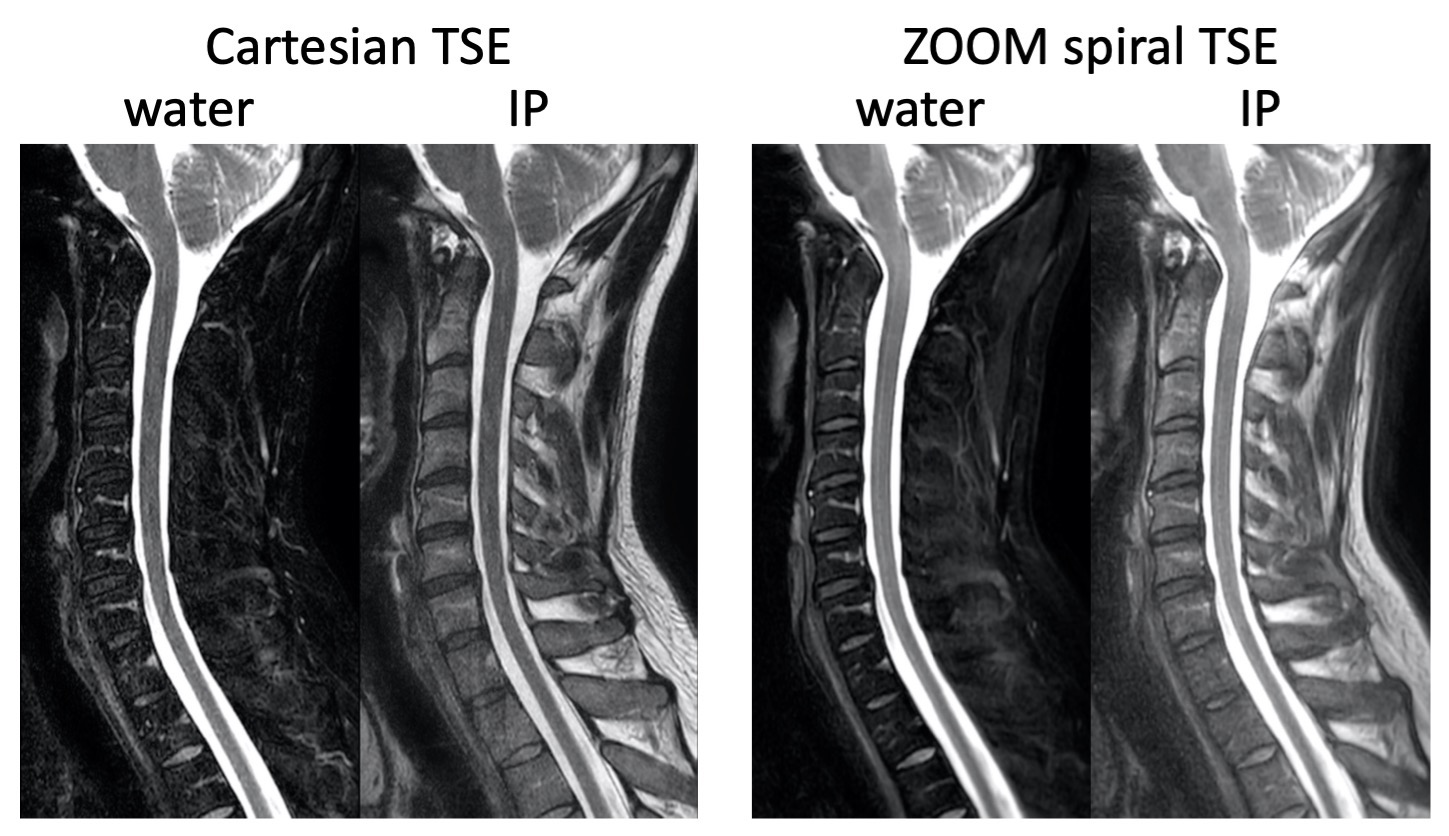
The phantom results are shown in Fig. 2. As can be seen from the images, there are residual unsuppressed signals with the saturation band (a), while much better suppression is achieved with ZOOM (b). The in vivo in-phase (IP) water/fat images (intermediate images before being cropped to user-prescribed FOV) are compared in Fig. 3, which confirm the effectiveness of ZOOM spiral TSE in suppressing signals outside the desired FOV. Fig. 4 compares the water and IP images from ZOOM spiral TSE to those with Cartesian TSE, showing improved SNR, superior delineation of the vertebrae, and good overall image quality with ZOOM spiral TSE compared to Cartesian mDixon TSE.Discussions
The phantom and in vivo images demonstrate the feasibility of using the ZOOM technique in spiral TSE imaging for better suppression of unwanted signals. One disadvantage of the ZOOM technique is the increased sequence duration and SAR due to the more advanced saturation segment; on the other hand, spiral TSE uses a reduced number of RF pulses compared to Cartesian TSE, which mitigates the overall SAR increase in the ZOOM spiral TSE combination. Additionally, the RF based reduced FOV technique may be incorporated to overcome this drawback. Future works also include more volunteer scans to demonstrate the improvement and reproducibility in overall image quality.Acknowledgements
This work is partially supported by Philips Healthcare.References
1. Li Z, et al. A 2D Spiral turbo spin echo technique. Magn Reson Med 2018;80:1989-1996.
2. Li Z, et al. T1, T2, and STIR-weighted spine MRI using spiral SE/TSE techniques. ISMRM 2019:2895.
3. Symms MR, et al. Zonally-magnified Oblique Multislice (ZOOM) EPI. ISMRM 2000;8:160.
4. King KF. Spiral scanning with anisotropic field of view. Magn Reson Med 1998;39:448-456.
Figures