1093
Rapid free breathing multi-slice radial CINE MRI using a patient sensing camera1Philips Healthcare, Best, Netherlands, 2Eindhoven University of Technology, Eindhoven, Netherlands
Synopsis
The benefits of the current cardiac CINE MRI are often limited by the requirement of patient co-operation for multiple breath-holds. To overcome this limitation, we present a new, free-breathing respiratory motion-compensated 2D multi-slice radial CINE method for left ventricular functional assessment. Our method utilizes the respiratory signal obtained from a patient sensing camera for performing motion weighted density compensation in radial gridding to minimize respiratory motion artifacts in the reconstructed image. The left-ventricular functional assessments from volunteers obtained using the proposed method are in good agreement with the results obtained using the standard Cartesian breath-hold method.
Introduction
Cardiac CINE MRI is clinically accepted as a gold standard to assess left ventricular (LV) volume and function assessment [1]. In this approach, an external electrocardiogram is used to synchronize the acquisition to freeze the contractile motion of the heart in each of the reconstructed cardiac phases. To minimize respiratory motion artifacts, several breath-holds are performed to acquire multiple 2D slices that cover the entire left ventricle, with a typical breath-hold time of 7-15s/slice depending on the Spatio-temporal resolution. Performing several long breath-holds may not be suitable for severely ill and/or uncooperative patients [2]. To overcome this limitation, a number of free-breathing CINE approaches that eliminate the breath-holds have been proposed [3] [4]. In this study, we developed a new rapid free-breathing non-respiratory gated CINE method based on multi-slice 2D radial acquisition using a patient sensing camera for retrospective respiratory motion correction.Methods
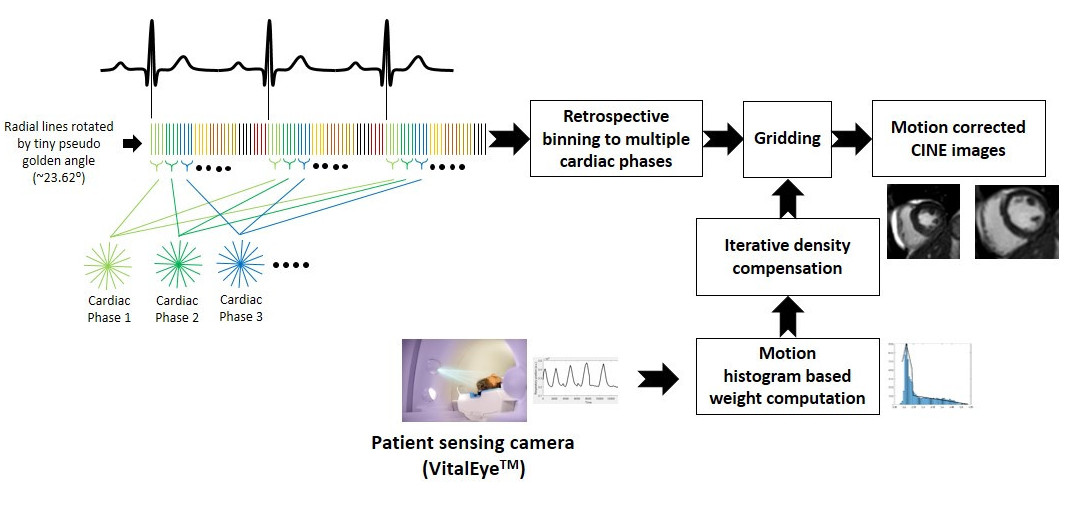
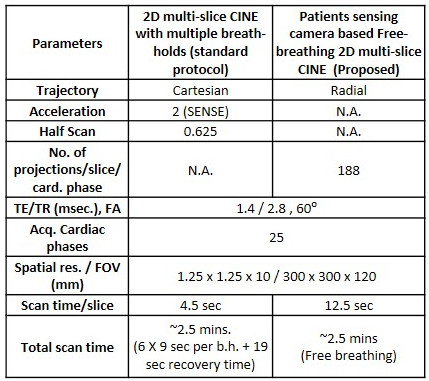
The schematic diagram of the proposed free-breathing cine imaging framework is shown in Fig.1. It is based on a multi-slice 2D radial bSSFP sequence with a pseudo-tiny-golden angle (23.62⁰) view ordering. Free-breathing radial acquisition with retrospective ECG triggering was performed while the respiratory signal as detected by the patient sensing camera (VitalEyeTM, Philips Healthcare, Best, The Netherlands) was recorded simultaneously. The acquired data were retrospectively binned to the different cardiac phases according to the acquired ECG signal. To minimize the image artifacts due to respiratory motion, a three-step procedure was followed: 1) respiratory motion weights for each radial projection were computed based on the histogram of the respiratory signal from VitalEyeTM. 2) These respiratory motion based weights were set as initial weights for each radial projection in the iterative density compensation computation proposed by Zwart et al., [1]. 3) The computed density compensation factors were then used in the gridding of the cardiac binned radial data to generate the final CINE images. The proposed method was implemented on a 1.5T MRI scanner (Ambition X, Philips Healthcare, Best, The Netherlands). All reconstructions were performed in-line on the scanner using a gridding algorithm developed in RECON 2.0. The performance of the proposed free-breathing radial method with respiratory weighted gridding was compared against the standard Cartesian breath-held CINE sequences for left-ventricular (LV) functional measurements in 8 volunteers of age 54±19 (mean ± sd.). The imaging parameters for the standard Cartesian sequence and the proposed free-breathing radial sequence are shown in Table 1. LV measurements including end-diastolic volume (EDV), end-systolic volume (ESV), and stroke volume (SV) were computed for the standard breath-hold method and the proposed free-breathing method using Philips IntelliSpace Portal software package.Results & Discussions
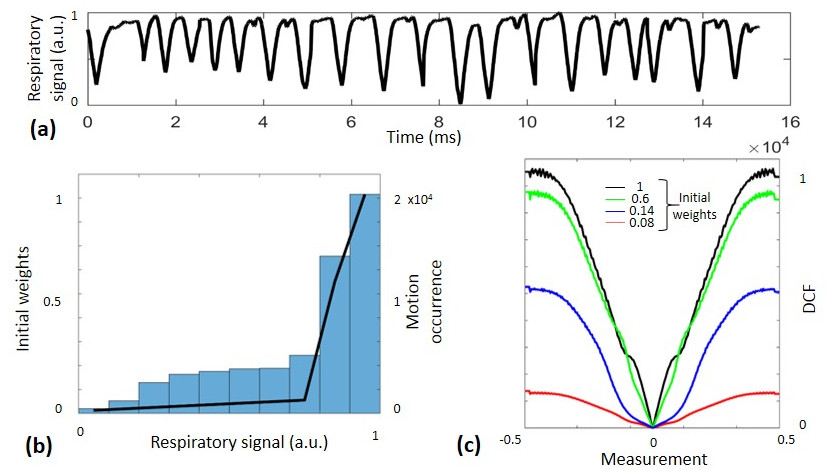
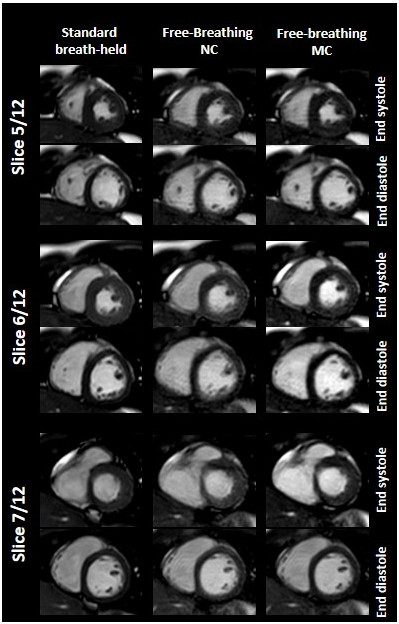
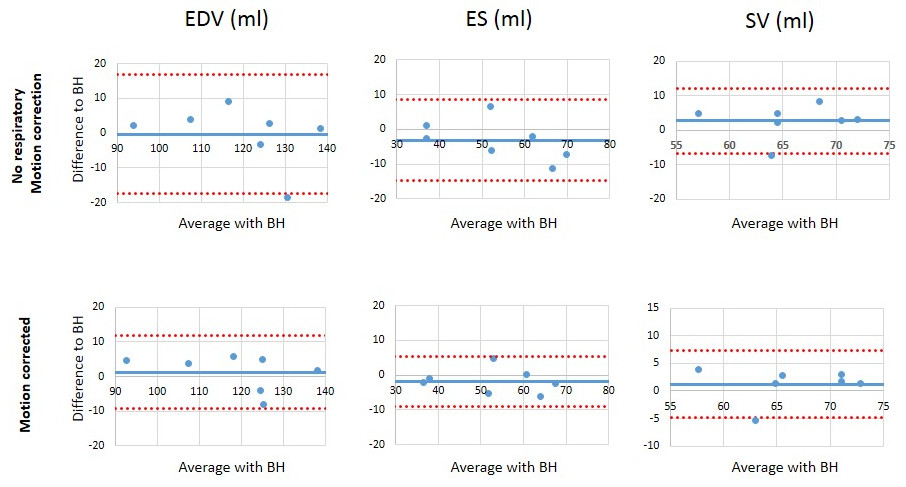
The 1D plot of the respiratory signal obtained from the patient sensing camera is shown in Fig 1(a). The initial weights as computed based on the respiratory motion histogram, shown in Fig 1 (b). The density compensation factors computed using the iterative algorithm [1] for each projection depending on the initial weights to be applied in the gridding of cardiac binned radial data are shown in Fig 2(c). According to the initial weights, the iterative density compensation algorithm automatically converges such that the overlapping regions of the radial projections in k-space are weighted to minimize artifacts due to respiratory motion while maintaining overall uniformity for faithful gridding. Representative images of the proposed method with and without motion correction are compared against the standard breath-hold method in Fig 3. Blurring due to respiratory motion was visibly minimized in the proposed method with respiratory motion correction when compared to the images without motion correction. The LV assessments as measured using different methods (standard BH Cartesian, FB radial without motion correction and FB radial with motion correction) were: EDV = 67.2±5.8, 64.5±5.3 & 66±5.51, ED = 119.4±13.9, 119.3±16.3 & 118±16, ES = 52.2±12, 55.3±15.1 & 53.9±12.6. The Bland-Altman plots comparing the LV volume assessments using the proposed method against the standard method are shown in Fig. 4. The LV assessments obtained from the proposed method were in good agreement with those obtained from the standard breath-hold method. However, residual aliasing artifacts were observed in the proposed method even after motion correction when compared to the standard Cartesian breath-hold method. The residual artifacts can potentially be removed by employing parallel imaging and/or deep learning-based reconstructions.Conclusions
We have developed a new free-breathing radial cardiac cine method with respiratory motion compensation based on a patient sensing camera, and evaluated its performance on volunteers for LV functional assessments. The proposed respiratory weighted radial gridding method is fast, simple and can be easily adapted to the current clinical settings for routine evaluation of patients who cannot hold their breath.Acknowledgements
This work was supported by the European Commission within the Horizon 2020 Framework through the MSCA-ITN-ETN European Training Networks (project number 642458)References
1. Sechtem, U., et al., Measurement of right and left ventricular volumes in healthy individuals with cine MR imaging. Radiology, 1987. 163(3): p. 697-702.
2. Jahnke, C., et al., Coronary MR imaging: breath-hold capability and patterns, coronary artery rest periods, and beta-blocker use. Radiology, 2006. 239(1): p. 71-78.
3. Ma, Y., et al., Compressed SENSE single-breath-hold and free-breathing cine imaging for accelerated clinical evaluation of the left ventricle. Clinical Radiology, 2019. 74(4): p. 325.e9-325.e17. 4. Usman, M., et al., Whole left ventricular functional assessment from two minutes free breathing multi-slice CINE acquisition. Physics in Medicine and Biology, 2015. 60(7): p. N93-N107.
5. Zwart, N.R., K.O. Johnson, and J.G. Pipe, Efficient sample density estimation by combining gridding and an optimized kernel. Magnetic Resonance in Medicine, 2012. 67(3): p. 701-710.
Figures