1091
Leaf: A Novel 3D Radial Trajectory for Free-breathing 3D Cine Cardiac Magnetic Resonance Imaging1Cardiology, Harvard Medical School, cambridge, MA, United States, 2Cardiology, Harvard Medical School, boston, MA, United States, 3Cardiology, Harvard Medical School, Boston, MA, United States
Synopsis
Free-breathing 3D cine steady-state free precession (SSFP) sequence with radial phyllotaxis trajectory is recently performed for making cardiac magnetic resonance imaging (MRI) exams easy and more comfortable for patients. Phyllotaxis trajectory is susceptible to the eddy current artifact due to a large gradient change during the 3D cine SSFP acquisition for measuring the centerline of k-space. We, therefore, developed and validated a novel leaf trajectory that minimizes the gradient change, and eddy current.
Introduction
Two-dimensional (2D) steady-state free precession (SSFP) cine imaging is the method of choice for evaluating ventricular size and function because of its high signal-to-noise and contrast-to-noise ratios.1 The standard clinical approach uses a retrospective electrocardiogram (ECG)-gated segmented Cartesian cine SSFP sequence that acquires 1-3 slices per breath-hold. This 2D technique requires breath-holding to suppress the respiratory motion of the heart. However, some patients are too young or ill to hold their breath. Furthermore, the 2D technique is sensitive to misregistration error due to variations in breath-holding position2 and requires an operator-dependent planning. Recent advances in acceleration techniques have led to free-breathing 3D cine SSFP acquisition with radial phyllotaxis trajectory.3,4 This 3D technique, however, periodically interrupts the cine SSFP acquisition to suppress the signal from fat and then drives the net magnetization vector back to the steady-state by using 10 startup pulses. Although these periodic interruptions improve the signal-to-noise and contrast-to-noise ratios of the 3D cine images, they preclude the acquisition of cine data throughout the entire cardiac cycle. Furthermore, phyllotaxis trajectory requires a large gradient change during data acquisition to read the centerline of k-space (for respiratory motion correction) that can create eddy current artifact. To address these shortcomings, we developed a non-interrupted 3D cine SSFP sequence with a novel leaf trajectory.Methods
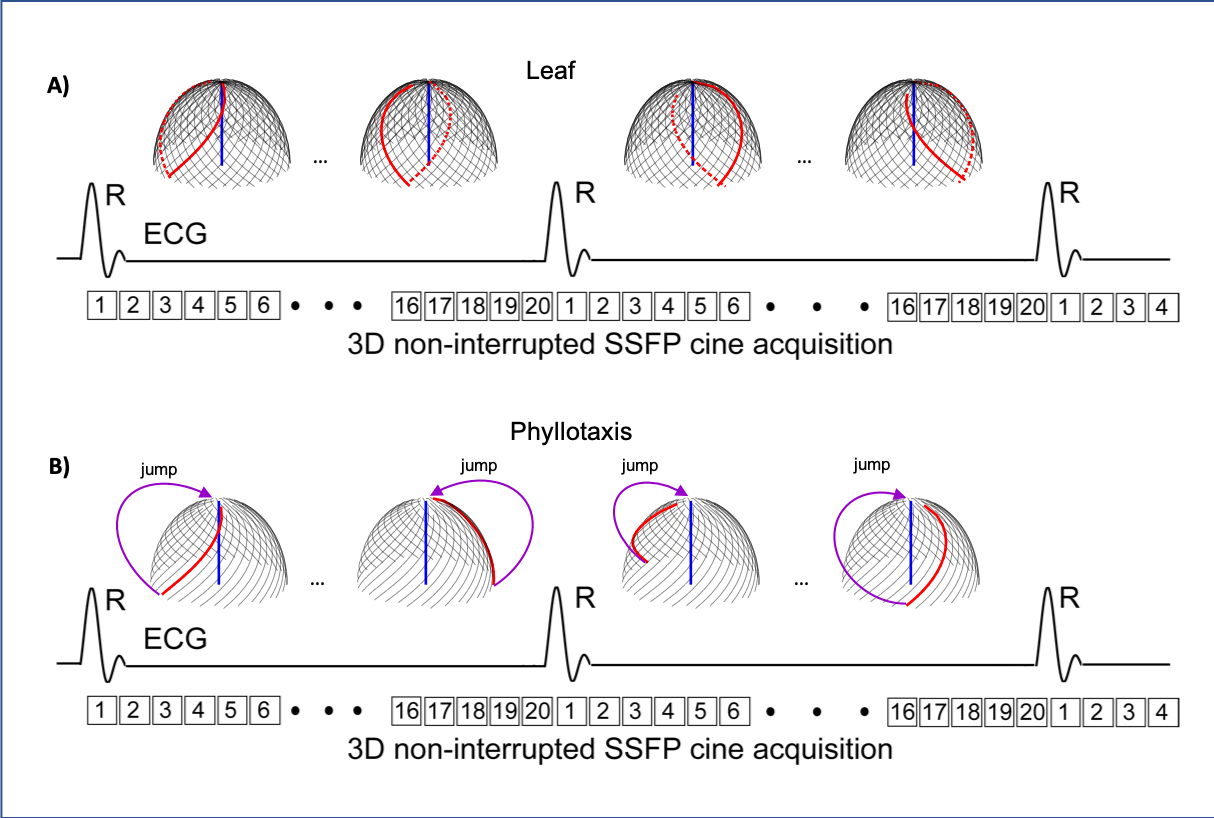
The schematic diagram of the developed non-interrupted 3D cine SSFP sequence with leaf trajectory is shown in Figure 1A. This sequence is using the ECG signal to retrospectively bin the data into 20 cardiac phases and a leaf trajectory to traverse the centerline of k-space along the superior-inferior direction at every other cardiac phase. Compared to the original phyllotaxis trajectory that has a large gradient change at the end of each cardiac phase to measure the centerline of k-space (Figure 1B), the leaf has a minimum gradient jump and a smooth change between each radial spoke. The leaf trajectory divides the total number of radial spokes in a 3D cine SSFP acquisition (i.e., N) to 2 groups: upward and downward arms. Then, it matches the closest upward and downward arms together and acquires those 2 arms in 2 consecutive cardiac phases. In this way, the leaf trajectory smoothly traverses from the zenith to horizon plane in one cardiac phase and then leaves the horizon plane toward the zenith in the next cardiac phase with a minimum gradient change. Furthermore, each leaf is rotated uniformly in the next two cardiac phases to take advantage of view sharing and evolution of signal over time. Figure 2 compares the phyllotaxis and leaf trajectories for a 3D cine SSFP acquisition. To assess the efficacy of this technique, we implemented the leaf trajectory on a 1.5T scanner (Philips, Achieva dStream) and performed a phantom and an in-vivo study. A phantom was imaged with the retrospective ECG-gated 3D cine SSFP sequence with the phyllotaxis and leaf trajectories. The imaging parameters were as follows: field-of-view (FOV) 200 mm, resolution 2.0 mm, flip-angle 60°, TR/TE 3.0/1.47 ms, number of shots (i.e., interleaves) 144, and TFE-factor (i.e., radial spokes per interleaf) 15. A 27-year-old male healthy volunteer was also imaged using the same sequence with the leaf trajectory and the following imaging parameters: FOV 200 mm, resolution 2.0 mm, flip-angle 60°, TR/TE 3.1/1.56 ms, number of shots 117, and TFE-factor 13. At the end of phantom and human subject scans, the k-space data and the centerline of k-space were extracted and the 3D cine SSFP images were reconstructed offline using a 3D NUFFT technique.8Results
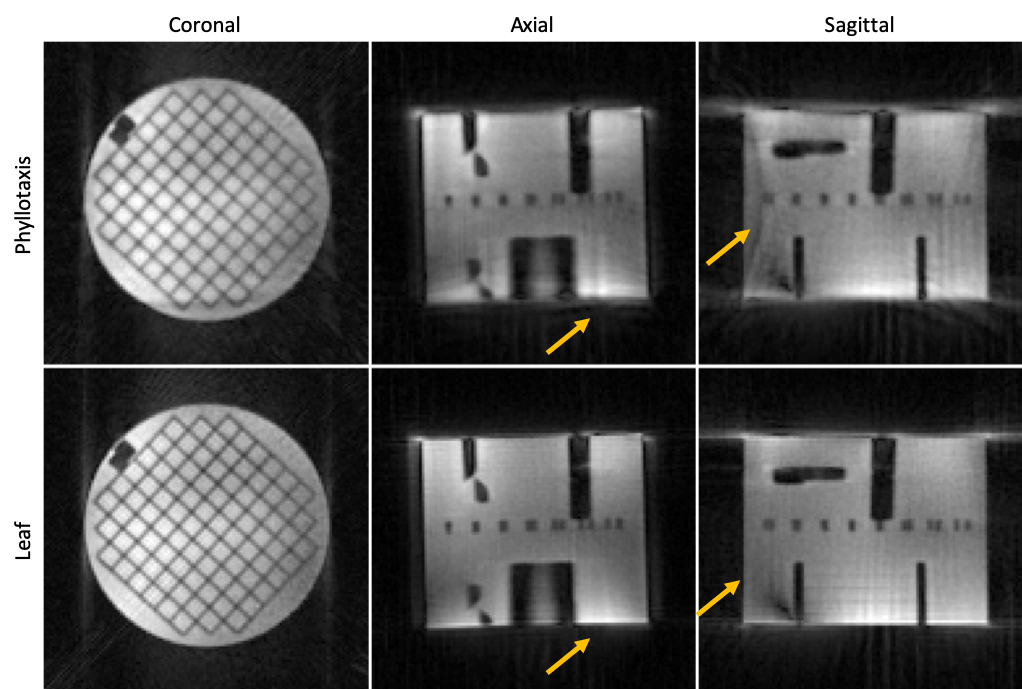
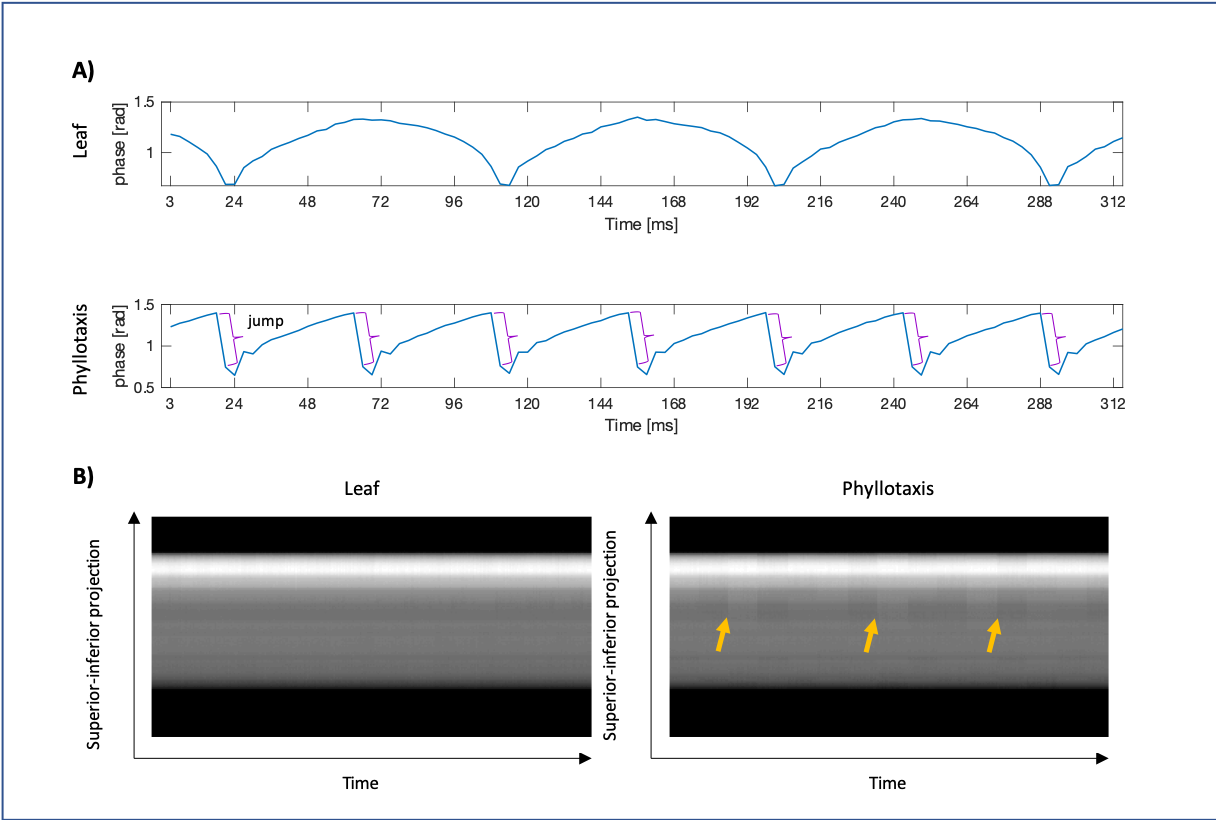
Figure 3 shows the phantom images acquired with the 3D cine SSFP sequence using phyllotaxis and leaf trajectories. The imaging time for both phyllotaxis and leaf trajectories were 2.3 minutes. The images of leaf trajectory show less artifact due to smaller gradient change, and therefore less eddy current artifact. As shown in Figure 4A, there is a minimum phase jump in the center point of k-space in the leaf trajectory. However, the phyllotaxis trajectory has a large phase jump at the end of each cardiac phase when the gradient is significantly changing for reading the centerline of k-space. Compared to phyllotaxis, the centerlines of k-space in the leaf trajectory are more homogeneous (Figure 4B). Figure 5 shows the free-breathing 3D cine images of the human subject in axial, coronal, and sagittal orientations. The acquisition time was ≈6.0 minutes.Discussion & Conclusion
We developed a novel leaf trajectory for free-breathing 3D cine SSFP sequence. Despite reducing the gradient jumps and gradient eddy current artifact in the leaf trajectory, the gradient delays and B0 induced phase error are still present in the datasets that need to be corrected. Also, a more sophisticated reconstruction pipeline, proposedly in-wavelet regularization and total variation along the time dimension, could further improve the image quality. Furthermore, the blood-to-myocardium signal to noise ratio of the 3D cine images should be further improved for favoring this technique in clinical practice over standard 2D cine acquisitions. Future work will include correcting for the gradient delays, B0 induced phase error, and comparing this technique with the standard 2D cine acquisitions in terms of scan time, ventricular volumetric measurements, and image quality.Acknowledgements
No acknowledgement found.References
1. Peters D.C., Nezafat R., Holger E., Stehning C., and Manning W.J.: 2D free-breathing dual navigator-gated cardiac function validated against the 2D breath-hold acquisition. J Magn Reson Imaging 2008; 28: 773-777.
2. Liu J, Wieben O, Jung Y, Samsonov AA, Reeder SB, Block WF. Single breathhold cardiac CINE imaging with multi‐echo three‐dimensional hybrid radial SSFP acquisition. J Magn Reson Imaging. 2010;32: 434– 440.
3. Piccini D, Feng L, Bonanno G, Coppo S, Yerly J, Lim RP, Schwitter J, Sodickson DK, Otazo R, Stuber M. Four-dimensional respiratory motion-resolved whole heart coronary MR angiography. Magn Reason Med 2017;77:1473–1484.
4. Feng LI, Coppo S, Piccini D, et al. 5D whole‐heart sparse MRI. Magn Reson Med. 2018;79:826–838.
5. Block K, Chandarana H, Milla S et al.Towards routine clinical use of radial stack-of-stars 3D gradient-echo sequences for reducing motion sensitivity. J Korean Soc Magn Reson Med 2014;18(2):87–106.
6. Piccini D, Littmann A, Nielles-Vallespin S, Zenge MO. Spiral phyllotaxis: the natural way to construct a 3D radial trajectory in MRI. Magn Reson Med 2011;66(4):1049–1056.
7. Brodsky EK, Samsonov AA, Block WF. Characterizing and correcting gradient errors in non-cartesian imaging: are gradient errors linear time-invariant (LTI)? Magn Reson Med 2009;62:1466–1476.
8. Knoll, F.; Schwarzl, A,; Diwoky, C.; Sodickson DK.: gpuNUFFT - An open-source GPU library for 3D gridding with direct Matlab interface. Proc ISMRM p4297 (2014).
Figures