1090
Real-Time free breathing cardiac CINE MRI with 84 channel high density receive array at 3 Tesla: Initial experience1University Medical Center Utrecht, Utrecht, Netherlands, 2Amsterdam University Medical Center, Amsterdam, Netherlands, 3Leiden University Medical Center, Leiden, Netherlands
Synopsis
Cardiac triggered CINE imaging is used clinically for the assessment of cardiac function. The purpose of this study is to investigate the feasibility of real time free breathing CINE MRI using a high density receive array on a 3T clinical system with online compressed SENSE image reconstruction. We demonstrate feasibility of real-time 2D CINE imaging using a high-density coil array.
Introduction
Cardiac triggered CINE imaging is used clinically for the assessment of cardiac function. For ample data quality breath-holds are needed to eliminate breathing motion artifacts, which is time consuming and uncomfortable for patients1. Furthermore, CINE CMR is challenging in patients with arrhythmias and requires real-time imaging, resulting in low spatial resolution. Therefore, it is desirable to accelerate CINE cardiac MRI to a single heartbeat acquisition per slice with reasonable spatial resolution. Parallel imaging is limited by the signal-to-noise ratio (SNR) and coil geometry2. High-density coil arrays can increase the maximal obtainable acceleration factor, by maximizing SNR and minimizing the g-factor3. The purpose of this study is to investigate the feasibility of real time free breathing CINE MRI using a high density receive array on a 3T clinical system with online compressed SENSE image reconstruction.Methods
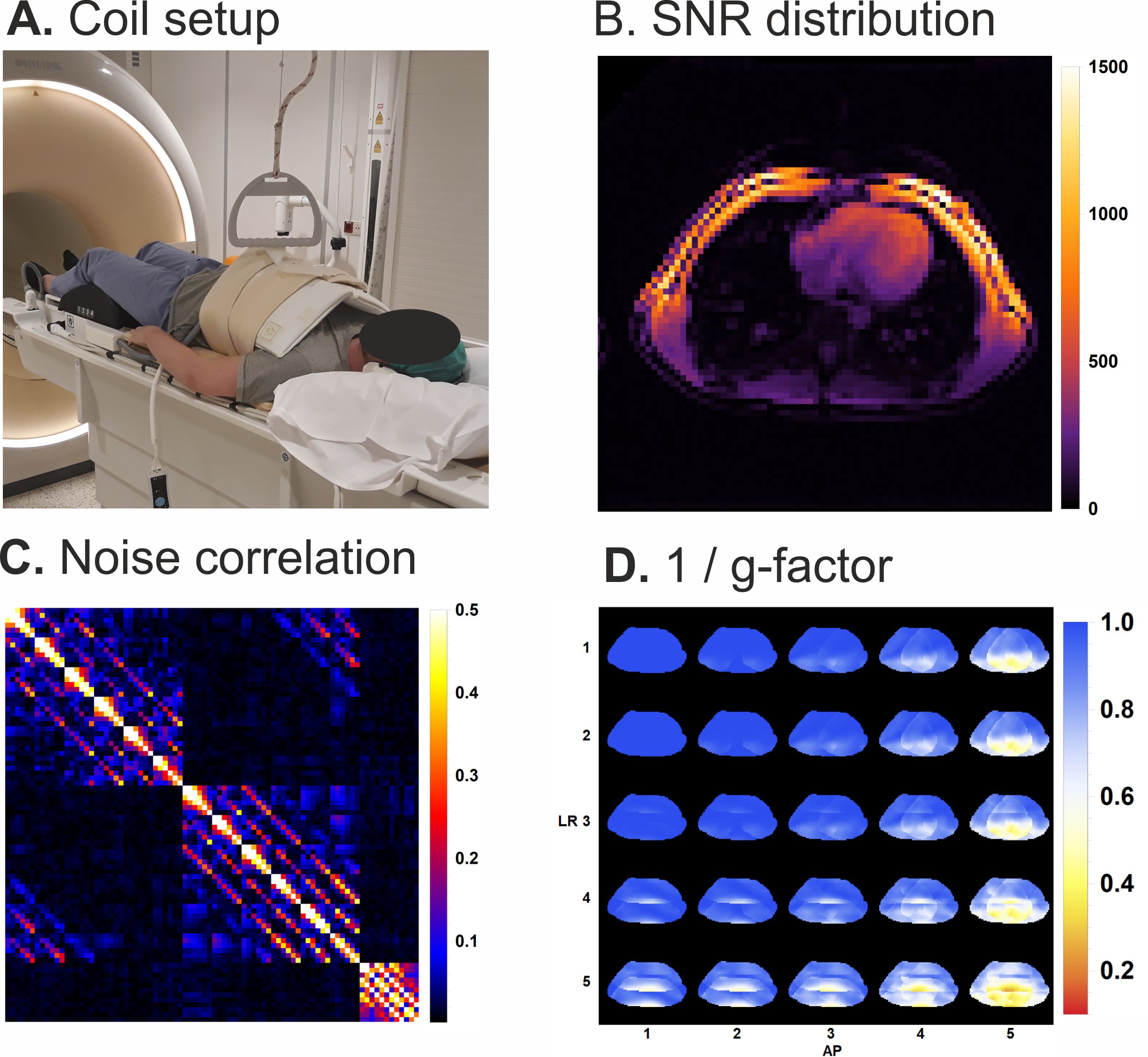
The coil setup consists of a high-density 72-channel cardiac array (Tesla Dynamic Coils, Zaltbommel, Netherlands) combined with the standard 12-channel posterior coil inside the patient table (Fig. 1) on a Philips 3T Ingenia system with dStream architecture (Philips, Best, Netherlands). To evaluate the acceleration performance of the coil setup four experiments using 2D CINE MRI were performed on a single volunteer (male, 29). All experiments comprised 2D CINE cardiac synchronized balanced SSFP acquisitions (TE = 1.4ms, TR = 2.8ms, FOV 300x300mm, acquisition voxel size = 2.0x1.6x8mm, recon voxel size = 1.25x1.25x8mm, FA = 45 degrees, temporal resolution: 45ms) with varying compressed-SESNSE acceleration factors. First, a 3 slice short axis, a 4 chamber and 2 chamber CINE acquisition with a C-SENSE factor 3.5 was acquired during 5 consecutive 4s breath-holds (4 heart-beats (HB) per slice) per slice. Secondly, to evaluate the C-SENSE performance of the coil, 6 dynamics of a single slice free-breathing acquisition were performed with C-SENSE factors of 3, 6 and 9 (4, 2, and 1 HB per slice, respectively). Thirdly, a free breathing whole heart (12 slices) acquisition with a C-SENSE factor 6 (duration 24 HB, 2HB per slice) and a C-SENSE factor 9 (duration 12 HB, 1HB per slice) was performed. Fourthly, 6 dynamics of a real-time free breathing 6 slice axial acquisition was performed using a C-SENSE factor 9 (duration 36HB, 1HB per slice).Results
All 84 receiver channels are well decoupled according to the noise-correlation matrix and the high density of small elements resulted in lower G-factors compared to the clinical used setup with 28 channels (Fig. 1). Additionally, calculated SNR distribution maps shows an increased SNR in the heart with respect to lower channel count coil setups. The first experiment shows that the 84 channel coil results in homogeneous CINE image in 3 orientations using very short breath-holds (~4s) (Fig. 2). For free breathing acquisitions, motions artifacts are still visible at C-SENSE 3 (see fig3 right top panel). With C-SENSE 6 and C-SENSE 9 scans breathing artifacts are minimized or mitigated, although the image quality is slightly lower (Fig. 3). Whole heart acquisition in free breathing is feasible for C-SENSE 6 and C-SENSE 9 where the tradeoff between C-SENSE 6 and 9 is the risk of motion artifacts versus image quality (Fig. 4). With C-SENSE 6 more slice to slice motion is visible compared to C-SENSE 9. Finally, free breathing real-time imaging for full heart coverage is feasible over multiple (36) heartbeats (Fig. 5).Discussion
In this study we show feasibility of real-time whole heart imaging in free breathing using a 84-channel coil setup with high SNR, superb acceleration performance and good to excellent image quality. Our results show a homogeneous CINE image, but short breath holds are required to eliminate breathing motions artifacts. To mitigate breath holds increased acceleration can be used with concessions to image quality. With a C-SENSE factor of 6 the image quality is acceptable. However there is still risk of introducing motion artifacts since the acquisition is spread over two cardiac cycles. To allow real time free breathing cine imaging the acquisition is optimally limited to one cardiac cycle, which can be obtained using a C-SENSE factor of 9. To Improve image quality of highly accelerated CINE we will add an additional high density receiver array to the posterior side of the body in future work.Conclusion
We demonstrate feasibility of real-time 2D CINE imaging using an 84 channel high-density coil array. In future work we will further increase the number of receiver channels to obtain even higher acceleration factors.Acknowledgements
No acknowledgement found.References
1: M. Saeed, T. A. Van, R. Krug, S. W. Hetts and M. W. Wilson, "Cardiac MR imaging: current status and future direction," Cardiovascular Diagnosis & Therapy, vol. 5, no. 4, pp. 290-310, Aug 2015.
2: K. P. Pruessmann, M. Weiger, M. B. Scheidegger and P. Boesiger, "SENSE: sensitivity encoding for fast MRI," Magn. Reson. Med., pp. 952-962, 1999.
3: Uğurbil, K, Auerbach, E, Moeller, S, et al. Brain imaging with improved acceleration and SNR at 7 Tesla obtained with 64‐channel receive array. Magn Reson Med. 2019; 82: 495– 509.
Figures