1087
Retrospective Compensation of Cardiac and Respiratory Motion in Mice using nonuniform Self-Gating1Core-Facility Small Animal Imaging, Ulm University, Ulm, Germany, 2Experimental Cardiovascular MRI, Ulm University Medical Center, Ulm, Germany
Synopsis
The application of self-gating techniques to small animal imaging poses challenging problems, particularly dominated by the high respiratory frequencies. Established self-gating methods are based on information that is extracted either from the k-space itself or from low-resolution images, leading to one-dimensional gating signals. These approaches are prone to fail in the case of arrhythmic respiratory and/or cardiac motion. The concept of nonuniform self-gating is capable of retrospectively considering respiratory and cardiac motion despite significant changes in cardiac or respiratory frequencies by using a two-dimensional gating matrix for deriving the required gating information.
Introduction
Mouse models are widely used to study human cardiac diseases due to a well characterised genome and many possible genetic modifications. Electrocardiograms(ECG) are most commonly used to synchronise the MRI acquisition with the cardiac cycle. However, the main magnetic field, the applied magnetic field-gradients and radio frequency pulses induce electric currents which strongly influence the ECG signal. Furthermore, only the ECG triggered data within e.g. the expiratory phase is used to minimise respiration-related artefacts.Established self-gating approaches which exploit signal variations around the k-space centre are prone to gradient induced signal variations, require dedicated signal filtering and processing and are likely to fail in the case of non-regular respiratory and cardiac motions.
Therefore, we present a nonuniform self-gating approach(nuSG), based on the work of Wundrak et al.1, adapted to the retrospective correction of respiratory and cardiac motion in rodents. The nuSG approach allows for non-uniform cyclic motion trajectories by replacing the one-dimensional gating signal of conventional image-based self-gating techniques with a two-dimensional gating matrix.
Methods
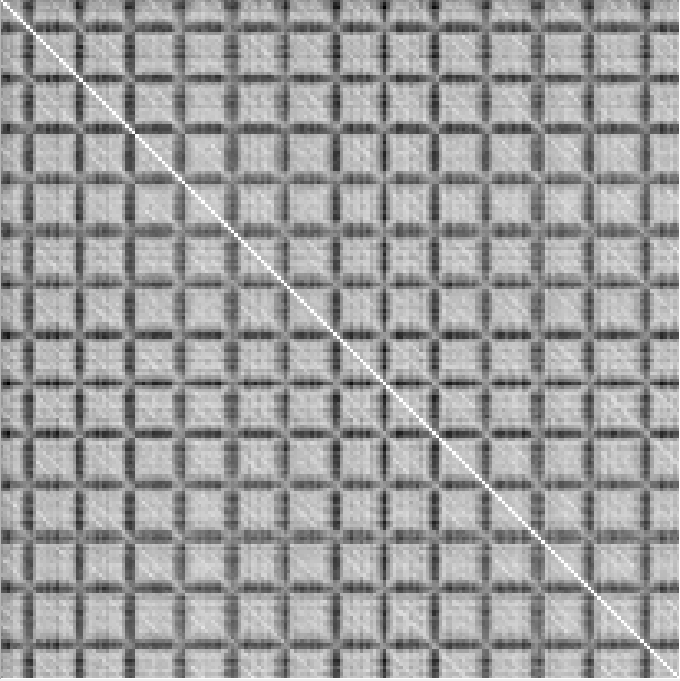
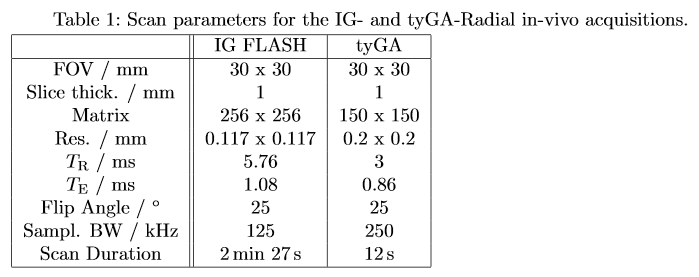
The nuSG reconstruction is based on continuously acquired 2D radial short axis images with scan parameters shown in table 1. All images were acquired using a tiny golden angle (tyGA) acquisition2 scheme to minimise motion sensitivity and eddy current artefacts on a 11.7 T preclinical MRI system (Biospec 117/16, Bruker, Ettlingen, Germany). High-resolution Intra-Gate(IG) images were acquired for comparison3. Frames with high temporal resolution were reconstructed from the radial datasets using a sliding window (SW) reconstruction. A ROI was then selected at the lung/liver interface to track respiratory motion over all SW-frames. The correlation matrix is then obtained by a pairwise correlation of all SW-frames of the ROI1. Each coefficient in the matrix is therefore a measure for the correlation of individual SW-frames with values ranging from zero to one. Each row in the correlation matrix corresponds to a 1D gating signal based on correlation coefficients with respect to the selected row (SW-frame). Afterwards, a Contour Fit1 is introduced which follows the respiratory motion with respect to the initial SW-frame (first local correlation maximum in the first row). Using the Contour Fit, it is possible to combine the k-space data of similar motion states and to reconstruct an associated image with high temporal and spatial resolution. The same procedure is then repeated for a second ROI which is placed over the left ventricle. Afterwards the correlation coefficients between both correlation matrices (lung, heart) are compared and matching correlations are then used for final image reconstruction.In contrast to the IntraGate approach, nuSG reconstructs a movie with equal temporal resolution (48 ms) as the initial SW reconstruction yet with combined data from several heart phases. Therefore, not a single averaged cardiac cycle is reconstructed, but the complete time evolution of the acquisition can be shown. To verify that the nuSG reconstruction is not mixing data from different motion states a frequency analysis can be performed. Identical ROIs (lung/liver edge and cardiac) as in the SW-frames are placed on the nuSG reconstructed frames, the correlation matrices calculated and a 1D-gating signal derived. The same (arbitrary, but usually the first) row of the correlation matrices (SW and nuSG), corresponding to a 1D-gating signal, is Fourier transformed into frequency domain and can be analyzed.
Results
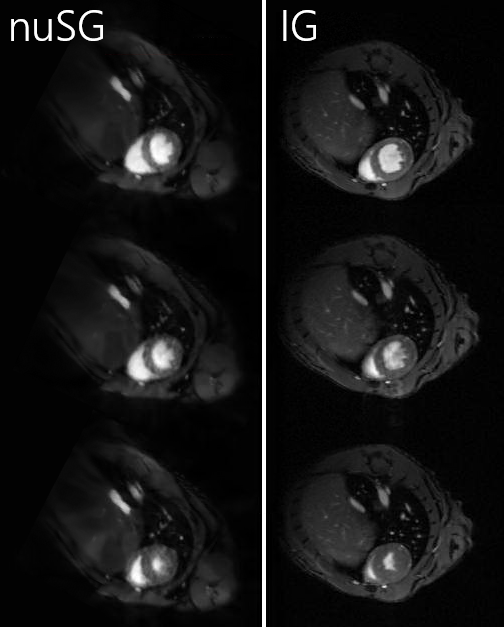
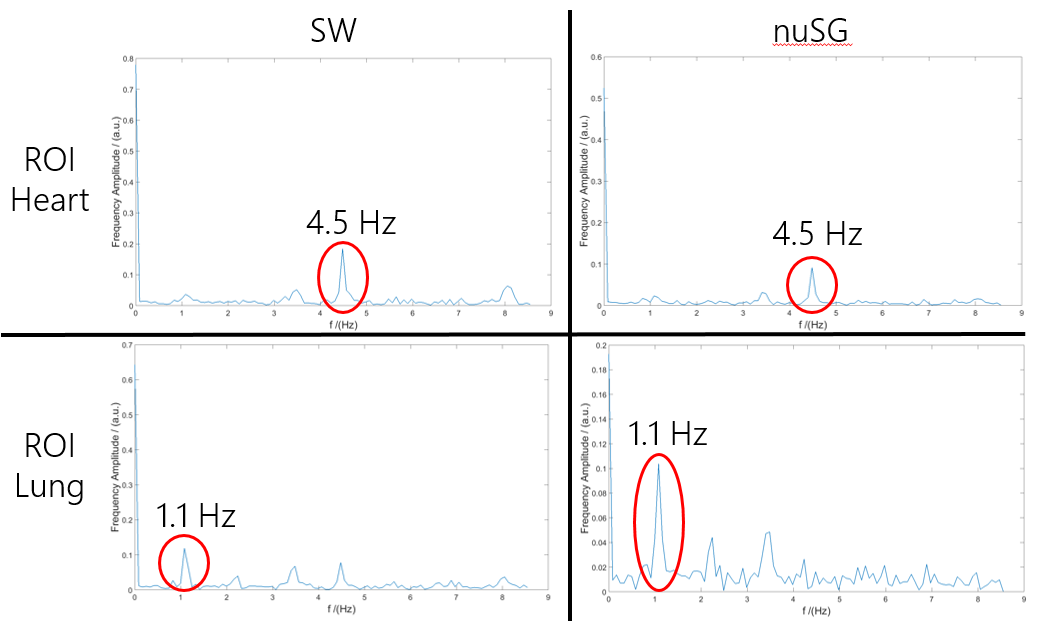
Figure 1 shows exemplarily three reconstructed heart phases of the nuSG and IntraGate approach. Each nuSG image was reconstructed using $$$\approx 300$$$ radial tyGA spokes, collected over correlating heart and respiratory phases.The frequency analysis is shown in figure 2. The left hand side shows the spectra for the SW-frames, the right hand side for the nuSG frames. Distinct peaks can be seen at 4.5 Hz for the cardiac ROI and at 1.1 Hz for the lung/liver edge ROI in both columns. For the SW-frames an additional peak at $$$\approx 8.1$$$ Hz is visible for both ROIs.
Discussion and Conclusion
Image quality is reduced within the nuSG approach, but can still be deemed diagnostic. The epicardial border can be well delimited in all cardiac phases. The endocardial border is well delimited in diastole, papillary muscles can be distinguished from the blood pool. In the systolic images, the endocardial border is slightly blurred, but not to an extent hindering analysis.The equal peaks in the 1D-gating signal of the sliding-window and nuSG reconstruction confirm the correctness of the proposed reconstruction method. The peak at $$$\approx 8.1$$$ Hz, which is only visible in the sliding-window derived frequency spectra, corresponds to gradient switching. This peak is minimized in the nuSG reconstruction due to the combination of data from different points in time during the acquisition.The nuSG approach shows promising results for retrospective correction of cardiac and respiratory motion in mice. The image quality is reduced compared to the gated reference standard but could be further improved, e.g. by longer acquisitions or Compressed Sensing. Further examinations in a larger cohort and comparison of functional values would be necessary to validate the use of nuSG in cardiac real-time imaging in the mouse. Furthermore, the nuSG approach is capable of reconstructing images of arbitrary motion states, as well as displaying the motion in chronological order, leading to a full assessment of cardiac and respiratory motion.
Acknowledgements
The authors thank the Ulm University Centre for Translational Imaging MoMAN for its support.References
[1] Wundrak S., Paul J., Radermacher M., Hombach V., Rottbauer W., Bernhardt P. and Rasche V. High-quality reconstruction of arrhythmic cardiac cycles. J Cardiovasc Magn Reson. 18, 2016.
[2] Wundrak S., Paul J., Ulrici J., Hell E., Geibel M.A., Bernhardt P., Rottbauer W. and Rasche V. Golden ratio sparse MRI using tiny golden angles. Magn Reson Med. 75, 2372-2378, 2016.
[3] Zuo Z., Subgang A., Abaei A., Rottbauer W., Stiller D., Ma G. and Rasche V. Assessment of Longitudinal Reproducibility of Mice LV Function Parameters at 11.7 T Derived from Self-Gated CINE MRI. BioMed Res Int. 2, 1-10, 2017.
Figures