1080
Vessel-selective 4D-MRA Using Superselective pCASL Combined with CENTRA-Keyhole (4D-S-PACK) for Intracranial Dural Arteriovenous Fistulas1Department of Clinical Radiology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, 2Department of Molecular Imaging & Diagnosis, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, 3Philips Japan, Tokyo, Japan, 4Philips Research, Hamburg, Germany, 5Division of Radiology, Department of Medical Technology, Kyushu University Hospital, Fukuoka, Japan
Synopsis
In this study, we demonstrated the ability of 4D-S-PACK (4D-MRA based on superselective pCASL with CENTRA-keyhole and view-sharing) to visualize intracranial DAVFs. 4D-S-PACK enables a time-resolved and vessel-selective angiography within 5 minutes without a use of contrast agents. It was shown that good vessel selectivity for the internal and external carotid arteries was achieved with 4D-S-PACK. 4D-S-PACK enabled accurate identification of feeding arteries. Although the superselective labelling in 4D-S-PACK caused a slight reduction in CNR, compared to full labelling in 4D-PACK, this was acceptable since visualization was well preserved. 4D-PACK can be a non-invasive clinical tool for assessing intracranial DAVFs.
INTRODUCTION
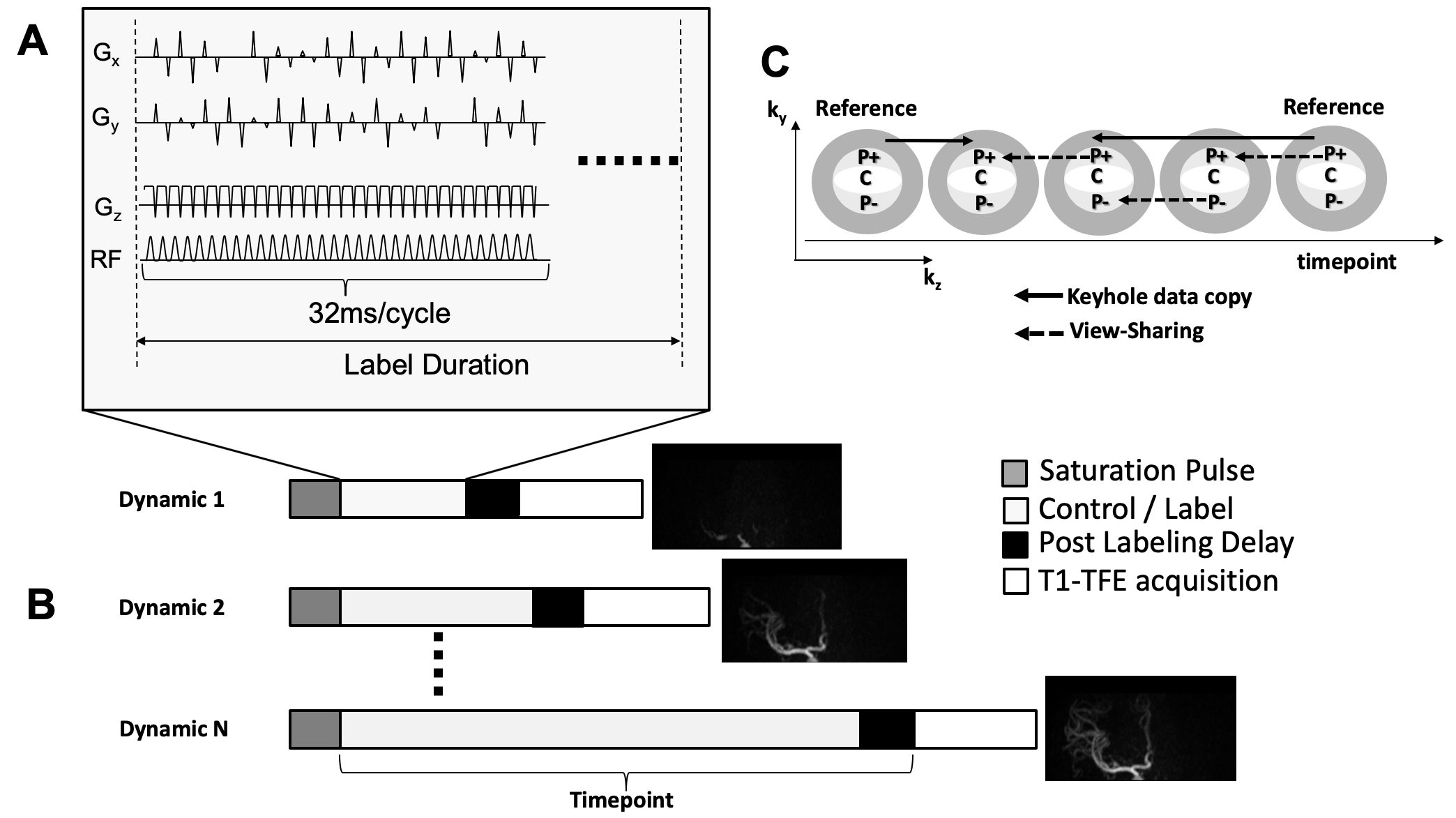
Intracranial dural arteriovenous fistula (DAVF) is a vascular condition where abnormal connections are made between branches of arteries and veins in the dura matter which can cause serious intracranial hemorrhage as well as other neurological issues. DSA is the current reference standard for the diagnosis of DAVF, however, it carries the risk of neurological complications and adverse reactions to contrast agents. We previously reported a new ASL-based approach for 4D-MRA named 4D-pCASL-based angiography using CENTRA-keyhole and view-sharing (4D-PACK), which enables multi-phase acquisition within a short scan time by using keyhole and view sharing, while keeping a high flow signal in later phases by using pCASL2,3. In 2010, superselective-pCASL was introduced as a pCASL based vessel-selective labeling method for regional perfusion imaging4,5. On top of the pCASL labelling scheme, superselective-pCASL uses additional gradients perpendicular to the flow direction resulting in labelling selectivity in those two directions. By dynamically changing the direction of the additional gradients in combination with changes to the phases of the RF pulses to neutralize the phase effects of these gradients at the targeted location, circular or elliptical labeling spots can be created. Recently, we proposed combining 4D-PACK with superselective pCASL as a new vessel-selective 4D-MR angiography technique, referred to as 4D-S-PACK (4D-MRA based on superselective pCASL with CENTRA-keyhole and view-sharing) hereafter6. The aim of the present study was to evaluate the ability of 4D-S-PACK to visualize intracranial DAVFs as compared with DSA and non-selective 4D-PACK.METHODS
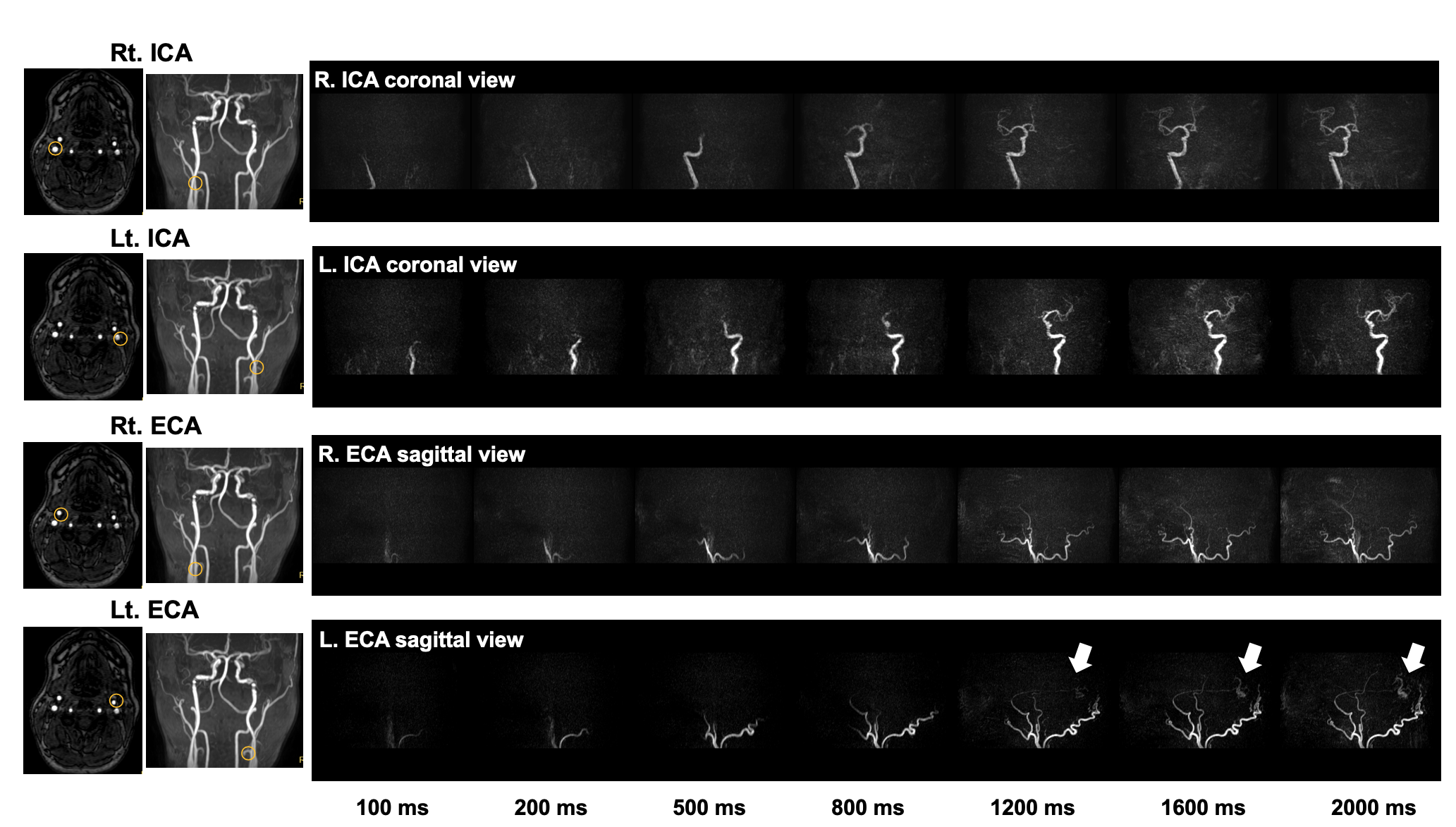
[Patients] Seven patients with intracranial DAVFs (age 64.0 ± 17.5 years; 4 males, 3 female) were examined. All patients underwent MRA and DSA within one month.[MRI] MR imaging were performed on a 3T MR scanner (Ingenia 3.0T, Philips, Best, The Netherlands) with a 15-channel head coil. 4D-S-PACK: Individual labeling of the internal carotid artery (ICA) and external carotid artery (ECA) on both sides was performed using the superselective-pCASL method (Fig. 1). The labeling focus was placed in the proximal ICA or ECA (Fig. 2). The gradient moment was set to be 0.75 mT/m/ms to create a labeling spot with a diameter of approximately 2cm. Images were obtained by changing the label duration: 100ms, 200ms, 500ms, 800ms, 1200ms, 1600ms, 2000ms. Scans were further accelerated with view-sharing. The other parameters were: sequence, 3D T1-TFE; TR/TE, 5.0/1.81ms; FA, 11°; ETL, 60; slab thickness, 80mm; voxel size, 1.0*1.4*1.6mm; SENSE, 3.0; keyhole 70%, acquisition time: approx. 5min.4D-PACK: Images were obtained with label durations of 100ms, 200ms, 400ms, 600ms, 800ms, 1200ms, 1600ms, and 2200ms. Other parameters were the same as those for 4D-S-PACK.
[Image Analysis] 1) The accuracy of vessel selectivity was assessed with a 4-point scale (1, poor; 4, excellent)7, 2) identification of feeding arteries, 3) The visualization of the feeding artery and venous drainage was assessed using the DSA image as the reference standard with a 5-point scale; 4) The CNRs were measured using the following equation; CNR = (Vesselmax – WMave) / WMSD.[Statistical Analysis] The identification of the feeding artery was compared between the methods by the chi-square test. The visualization scores and maximum CNRs were measured between 4D-S-PACK and 4D-PACK using the Wilcoxon matched-pairs signed rank test.
RESULTS
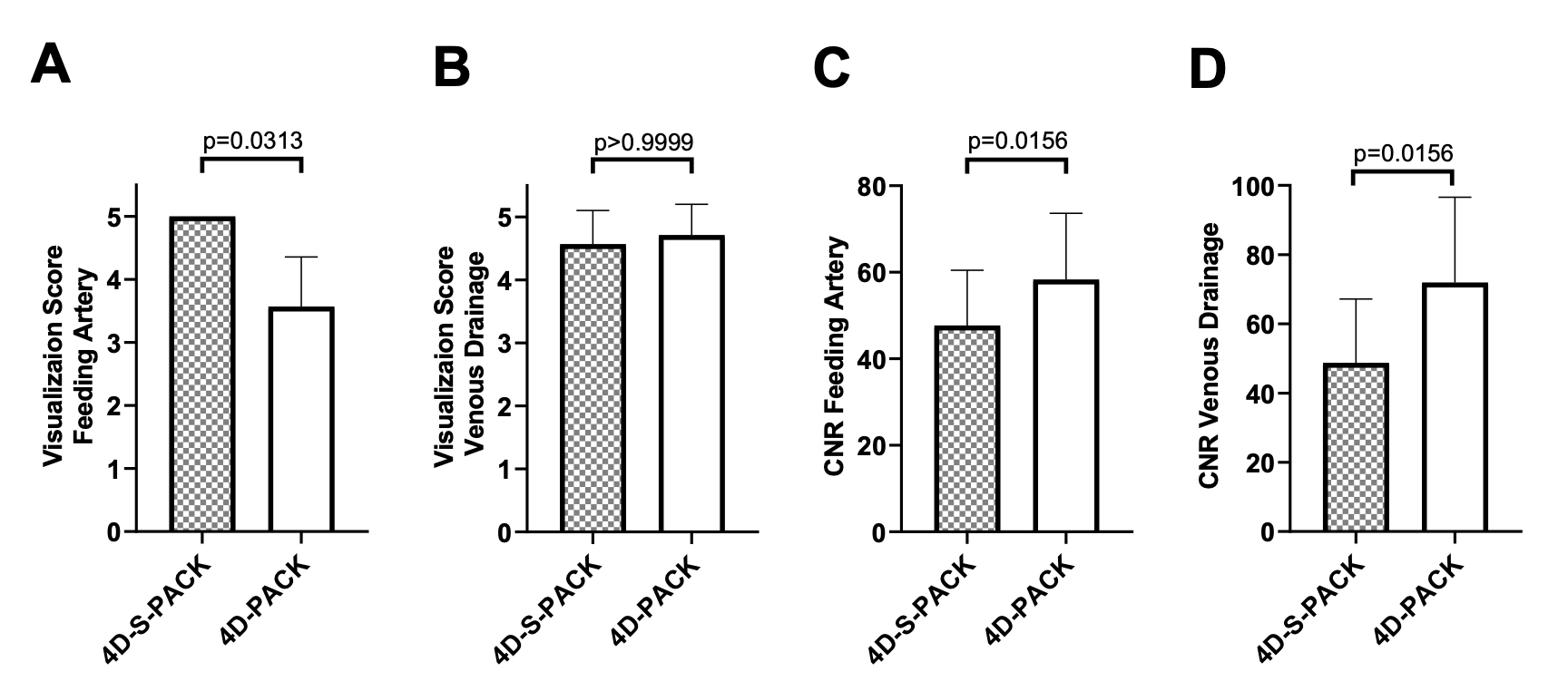
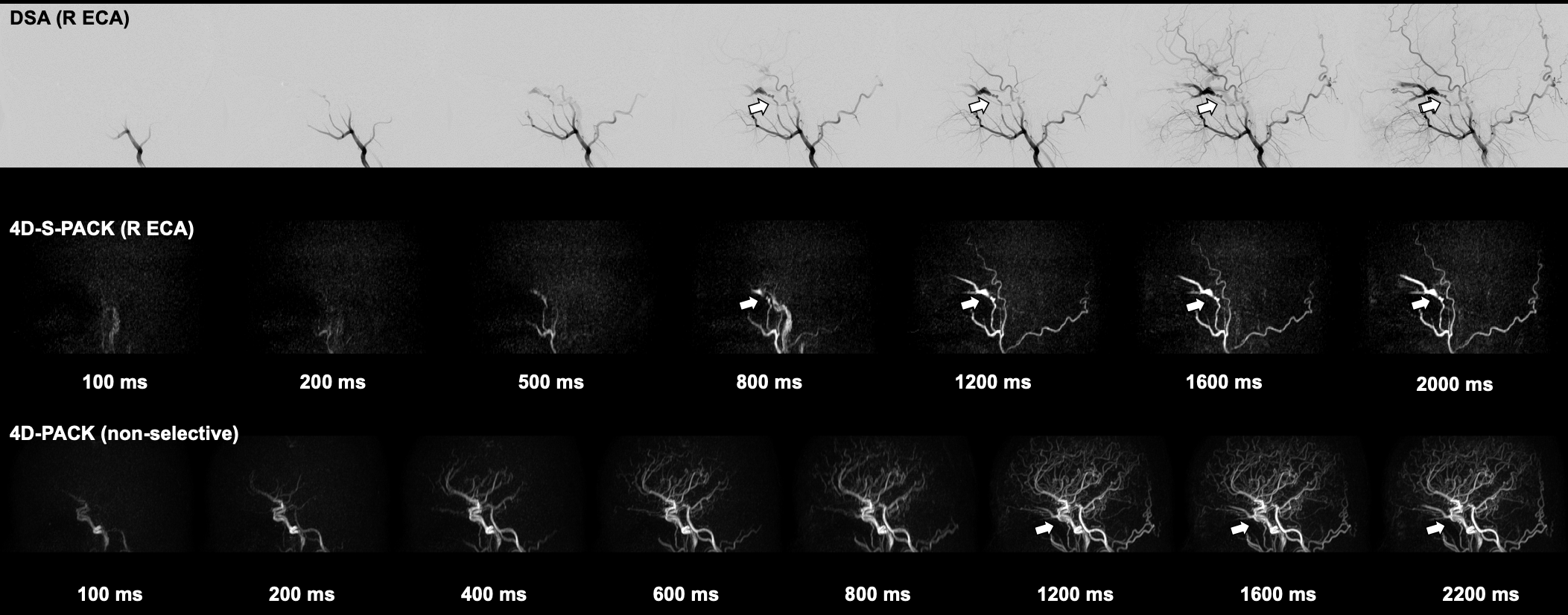
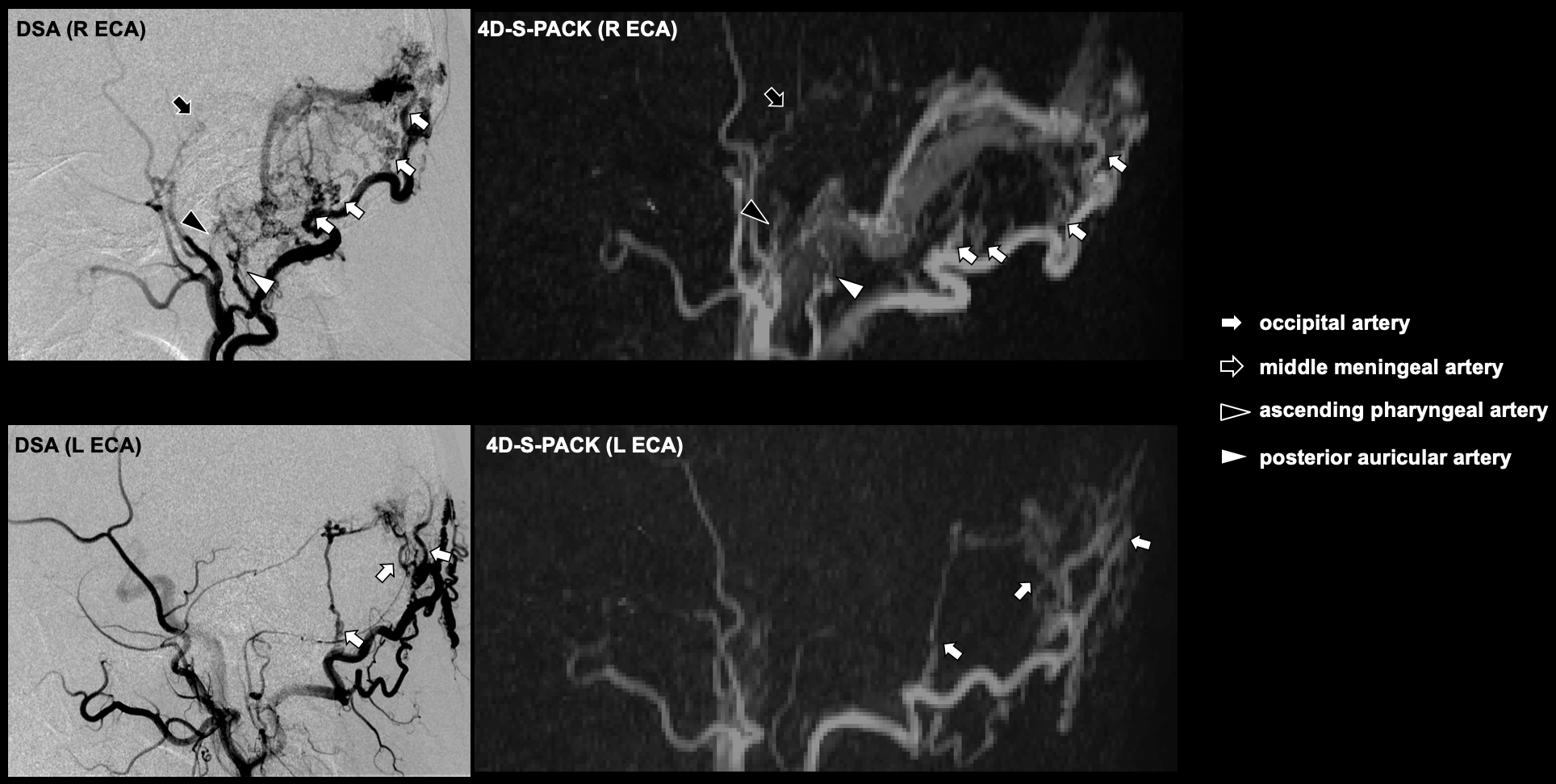
The vessel selectivity with 4D-S-PACK was perfect (grade 4) in 22 out of 28 territories (78.6%). 4D-S-PACK detected 22 out of 31 feeding arteries (sensitivity, 71.0%; specificity, 100%, accuracy, 90.1%, p<0.0001) whereas the 4D-PACK detected seven out of 31 arteries (sensitivity, 22.6%; specificity, 100%, accuracy, 75.5%). Figure 3 shows the visualization scores and maximum CNRs. The visualization scores for feeding arteries (5.00±0.00, p=0.0313) were significantly higher in 4D-S-PACK than in 4D-PACK (3.57±0.79), while the scores for venous drainage were not different between the two methods (4D-S-PACK, 4.57±0.53; 4D-PACK, 4.71±0.49). Maximum CNRs in both feeding arteries (4D-S-PACK, 47.7±12.8; 4D-PACK, 58.3±15.3, p=0.0156) and draining veins (4D-S-PACK, 48.7±18.5; 4D-PACK, 71.9±24.7, p=0.0156) were significantly lower in 4D-S-PACK than in 4D-PACK. Figure 4 shows a DAVF supplied by the right accessary meningeal artery with drainage into the right cavernous sinus, and then the right superior and inferior ophthalmic veins. The selective labeling of the right ECA was successful, and no untagged vessels were observed. 4D-S-PACK sequentially depicted the feeding artery and then draining veins, and its visualization was comparable to that on DSA. It was difficult to identify the feeding artery on non-selective 4D-PACK because of overlap with many other vessels. Figure 5 shows a DAVF supplied by multiple branches of bilateral ECAs. 4D-S-PACK enabled the separate labeling and imaging of each ECA as seen on DSA, which helped the accurate identification of feeding arteries.DISCUSSION
4D-S-PACK enabled a time-resolved and vessel-selective angiography within 5 min without contrast agents. Good vessel selectivity was achieved with this method. 4D-S-PACK was useful in the identification of feeding arteries since these arteries were readily detected on the DSA-like images on 4D-S-PACK. Although the CNRs were reduced in 4D-S-PACK compared to 4D-PACK presumably due to a labeling loss during super-selective label focusing, this was acceptable since visualization was well preserved.CONCLUSION
4D-S-PACK allowed for vessel-selective 4D-MRA and was useful in visualizing intracranial DVFs, especially in identification of feeding arteries. The 4D-S-PACK can be a non-invasive clinical tool for intracranial DAVFs.Acknowledgements
No acknowledgement found.References
1. Hernesniemi JA, Dashti R, Juvela S, et al. Natural history of brain arteriovenous malformations: A long-term follow-up study of risk of hemorrhage in 238 patients. Neurosurgery 2008;63:823-829.
2. Obara M, Togao O, Beck GM et al. Non-contrast enhanced 4D intracranial MR angiography based on pseudo-continuous arterial spin labeling with the keyhole and view-sharing technique. Magn Reson Med. 2018 Aug;80(2):719-725.
3. Togao O, Hiwatashi A, Obara M, et al. 4D ASL-based MR angiography for visualization of distal arteries and leptomeningeal collateral vessels in moyamoya disease: a comparison of techniques. Eur Radiol. 2018 Nov;28(11):4871-4881.
4. Helle M, Norris DG, Rüfer S, et al. Superselective Pseudocontinuous Arterial Spin Labeling. Magn Reson Med 2010;64: 777–786.
5. Helle M, Rüfer S, van Osch MJ, et al. Superselective arterial spin labeling applied for flow territory mapping in various cerebrovascular diseases. J Magn Reson Imaging. 2013 Aug;38:496-503.
6. Obara M, Togao O, Helle M, et al. Investigation of Intracranial Artery Selective Visualization in Superselective 4D-MR Angiography with Pseudo-Continuous Arterial Spin Labeling Combined with CENTRA-Keyhole and View-sharing (SS-4D-PACK). Proc Int Soc Magn Reson Med. 2018;27:185.
7. Fujima N, Osanai T, Shimizu Y et al. Utility of noncontrast-enhanced time-resolved four-dimensional MR angiography with a vessel-selective technique for intracranial arteriovenous malformations. J Magn Reson Imaging. 2016 Oct;44:834-45.
Figures