1076
Compressed SENSE combined with Keyhole and View-Sharing accelerate Non-contrast enhanced 4D Intracranial MRA based on pCASL1Clinical Science, Philips Healthcare, Shanghai, China, 2Drum Tower Hospital, Medical School of Nanjing University, Nanjing, China
Synopsis
The non-contrast enhanced 4D MRA is time-consuming because of the needs to acquire high resolution data at multi-timepoints, which limited its clinical application.In current study, 4D-PACK combined with C-SENSE=6.5 can reduce 23% acquisition time(4 min 42s) for non-contrast enhanced 4D-MRA compared with 4D-PACK with SENSE acceleration, and the excellent acceleration advantage of C-SENSE can improve the clinical application for 4D MRA. the proposed acquisition scheme of 4DMRA with C-SENSE acceleration can be potentially used for evaluating arteriovenous malformation (AVM), arteriovenous fistulas (AVF), moyamoya disease, and stroke patients.
Introduction
Non-contrast enhanced 4D intracranial MRA(4D-MRA)can be acquired using arterial spin labeling techniques and be used for evaluating arteriovenous malformation (AVM), arteriovenous fistulas (AVF), moyamoya disease, and stroke[1]. However, the 4D MRA is time-consuming because of the needs to acquire high resolution data at multi-timepoints, which limited its clinical application. Obara M. demonstrated accelerated 4D dynamic MR angiography (4D-MRA) using pseudo-continuous arterial spin labeling (pCASL), combined with Keyhole and View-sharing (4D-PACK), but not implemented compressed sensing[2]. In current study, we proposed a protocol to further accelerate 4D MRA using 4D-PACK combined with Compressed SENSE(C-SENSE), while maintaining a high quality MRA image.Methods
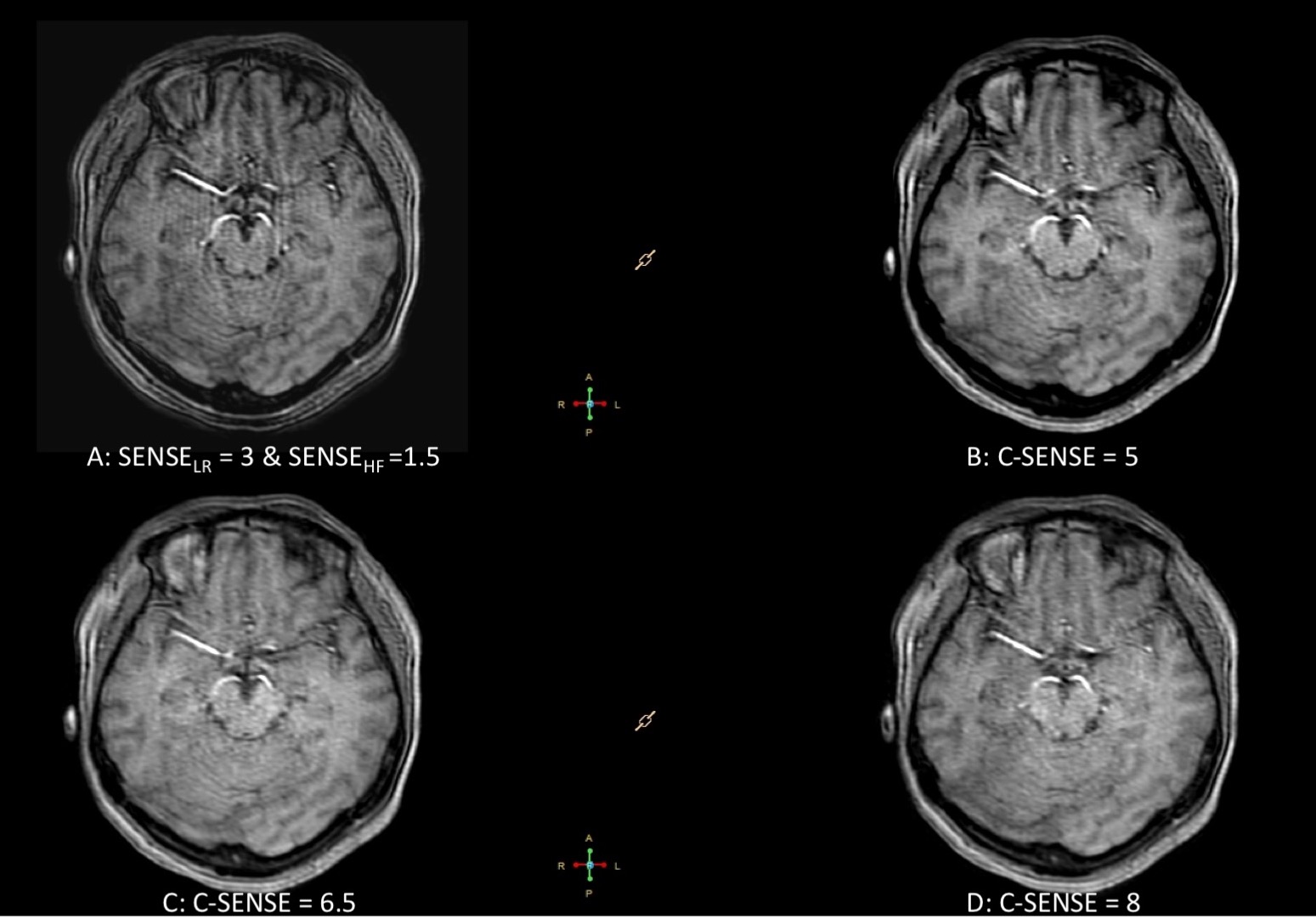
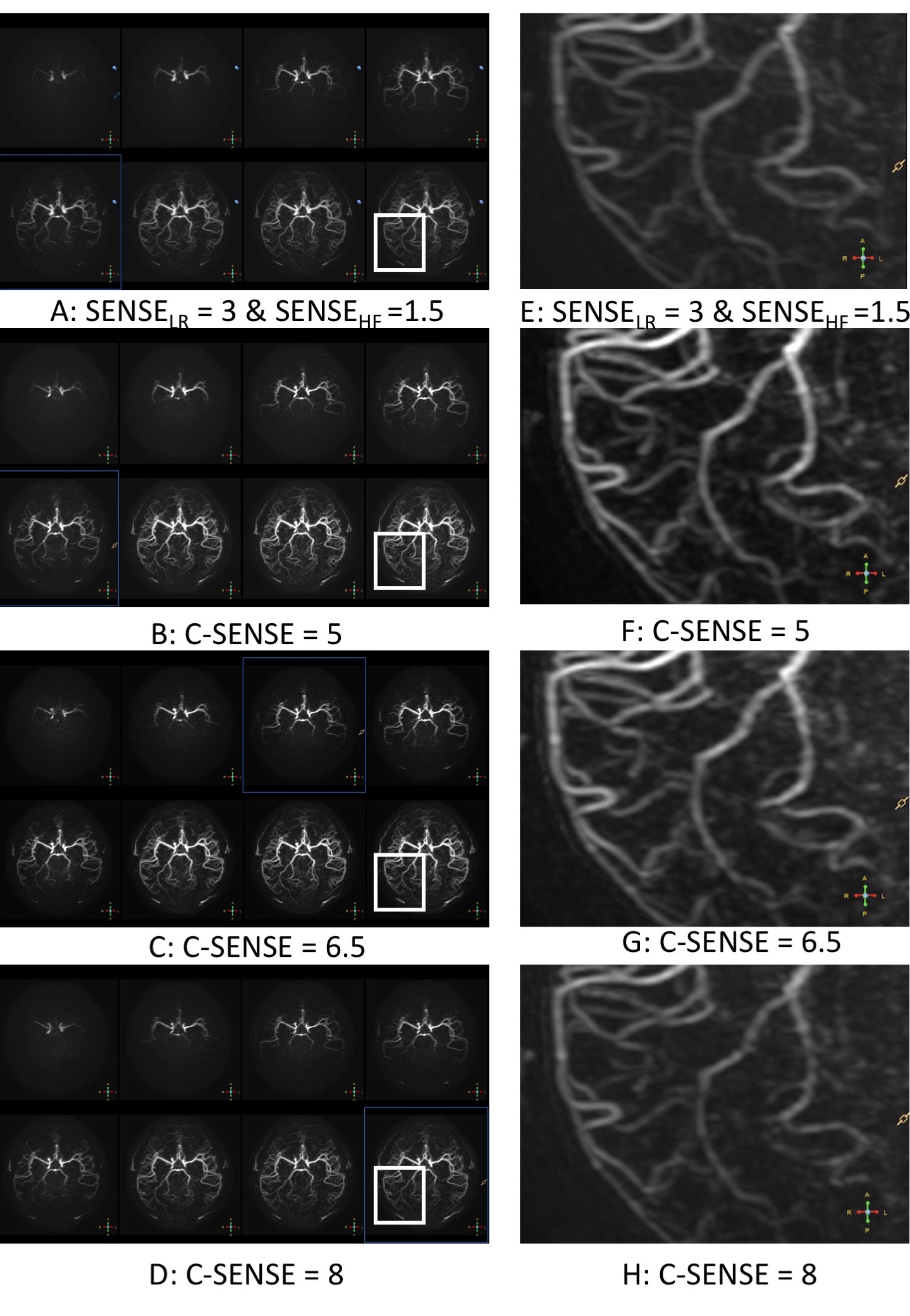
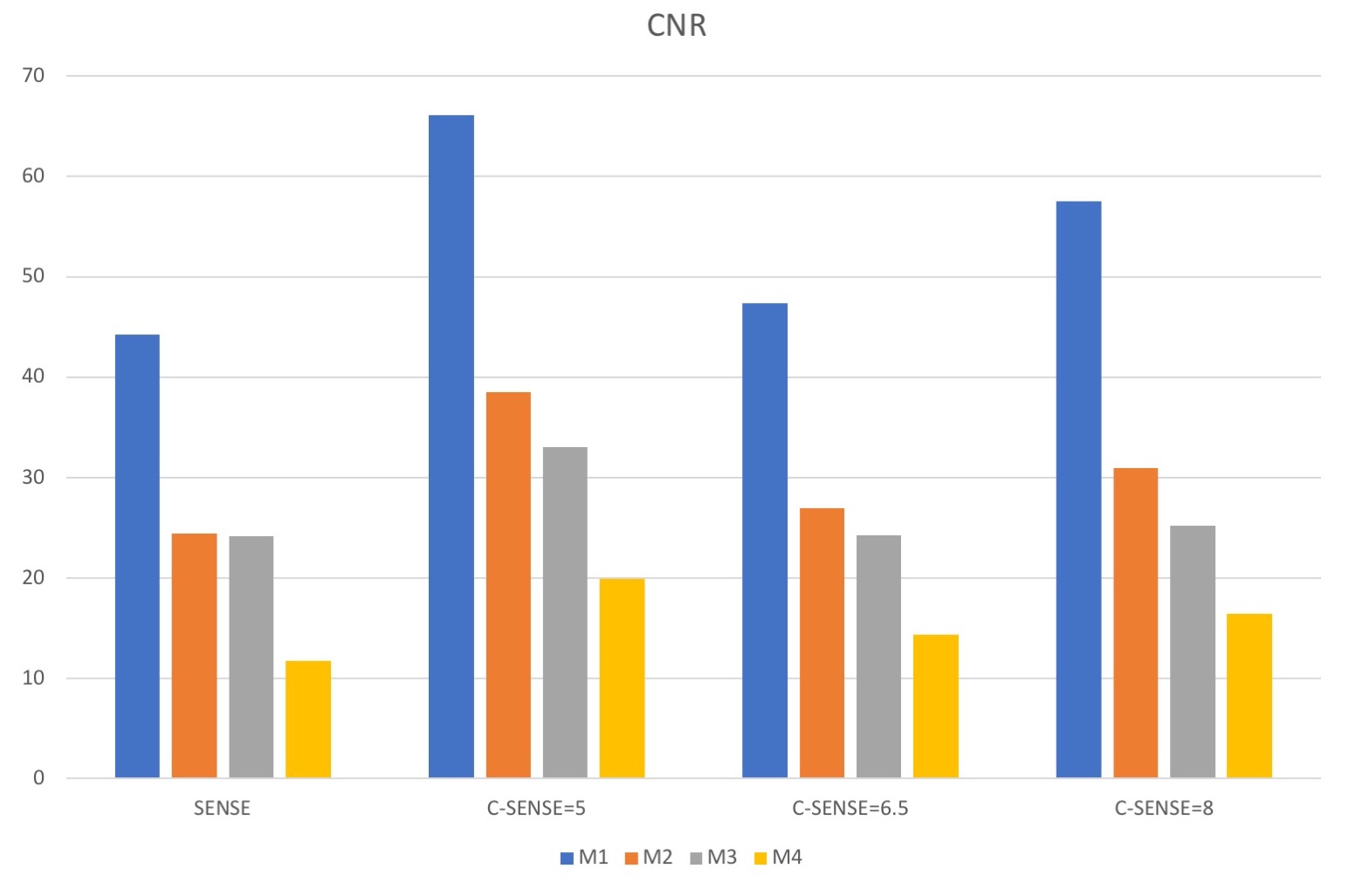
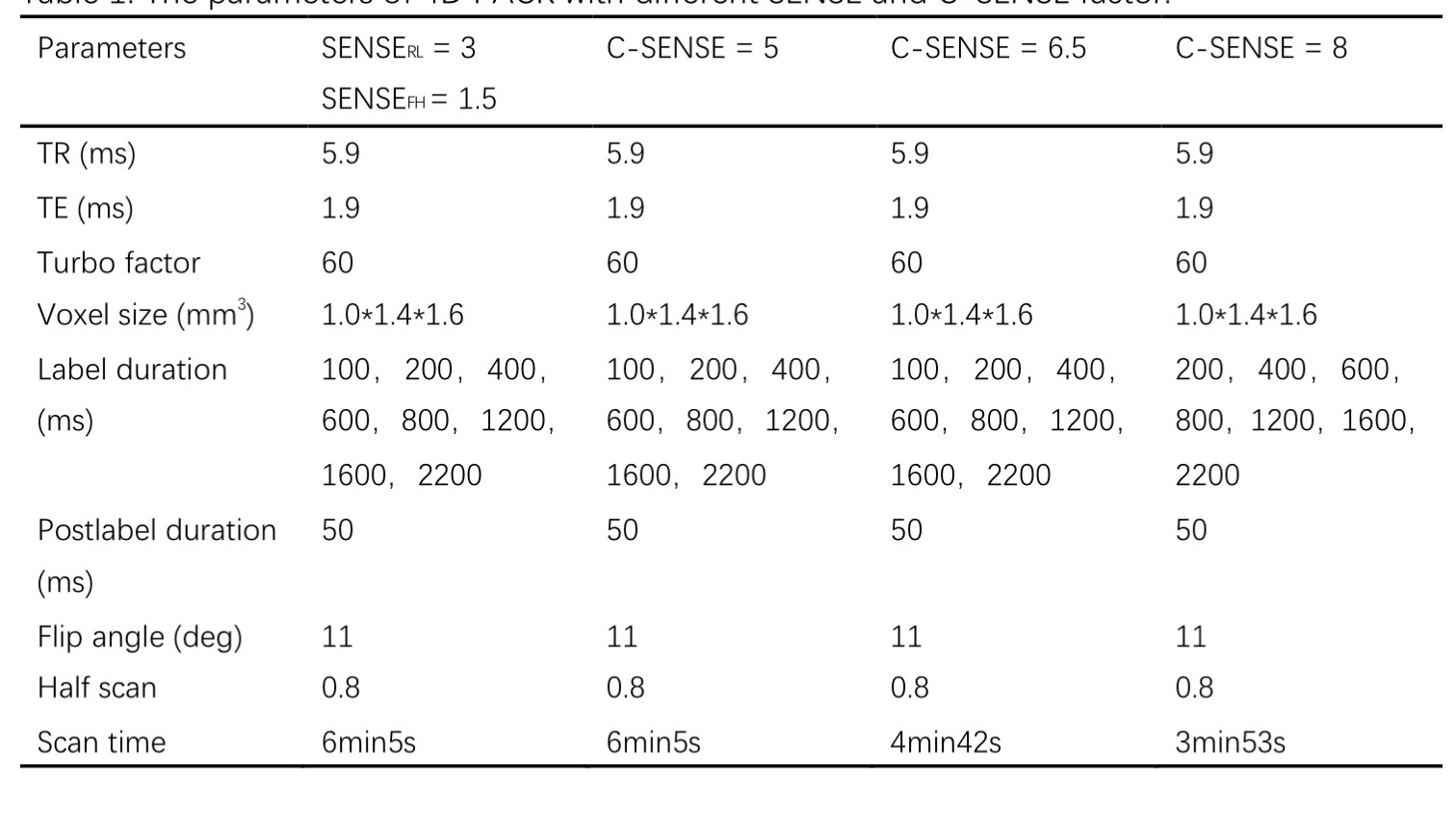
4D-PACK with Compressed SENSE were performed on 3.0T MR system (Ingenia CX, Philips Healthcare, Best, The Netherland)with a 32 channel head coil compared with 4D-PACK with the conventional SENSE acquisition techniques (SENSELR= 3 & SENSEHF=1.5). One healthy subject(female, 48 years)was examined for different Compressed SENSE factor(C-SENSE factor, 5, 6.5 and 8) compared with SENSE factor = 5, the detail parameters were presented in Table 1. The axial maximum intensity projection (MIP) images and the source image for each timepoint were used to evaluate the image quality. The regions of interest(ROI) were drawn on white matter (WM) and middle cerebral artery (MCA) which include M1, M2, M3, M4 segments. The mean signal of 4 MCA segments and WM were extracted to calculate contrast to noise ratio(CNR), CNR = (SI_meanMCA– SI_meanWM) / SI_stdWM. The CNR value can reflect flow visualization ability in 4D-PACK. One patient with intracranial aneurysms were acquired 4D-PACK data to implement clinical feasibility of 4D MRA.Results
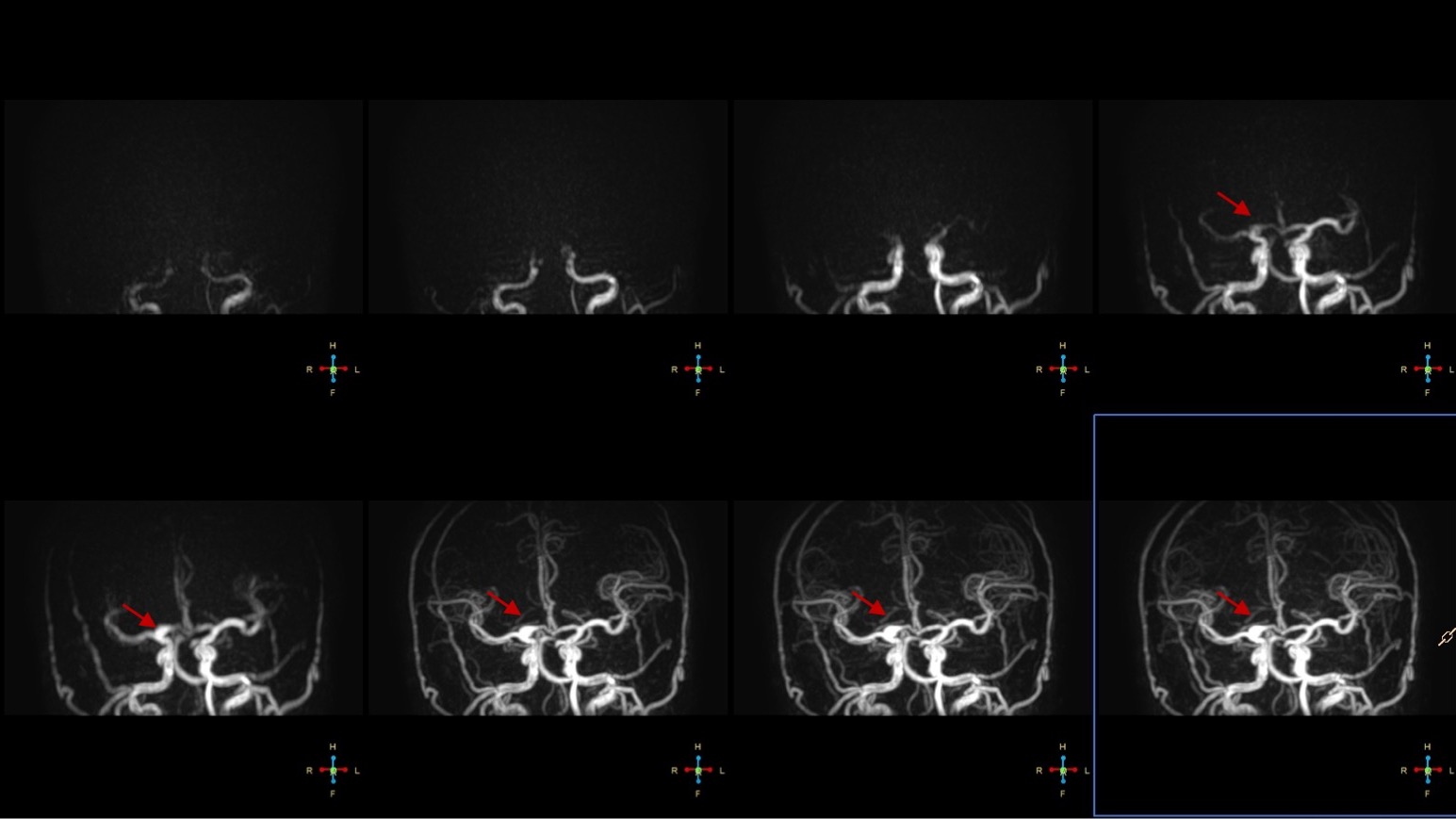
The source images of 4D PACK with SENSELR= 3 & SENSEHF=1.5 have subtle artifacts within brain tissue and artery vessel areas. The artifacts are reduced in 4D-PACK with C-SENSE acceleration(Figure 1). The axial 4D MIP-MRA based on 4D-PACK with different acceleration factor(SENSELR= 3 & SENSEHF=1.5., C-SENS=5, 6.5, 8) for each timepoint are exhibited in Figure 1A. The 4D MRA images obtained from all acceleration factor show similar dynamic arterial inflow, and the images with C-SENSE factor, especially C-SENSE = 5 or 6.5, are presented sharper blood vessels than SENSELR= 3 & SENSEHF=1.5.The distal vessel branches at last timepoint for C-SENSE = 8.5 are not clearly displayed or disappear, but other acceleration factors are displayed excellent distal vessel branches (Figure 1B). The CNR of 4D MRA in all MCA segments with C-SENSE = 8 is higher than other acceleration factors, and C-SENSE=6.5 is better than SENSE=5, the detail presented in Figure 3. Thus, we suggested that the 4D-PACK with C-SENSE =6.5 can be used to achieve excellent dynamic artery inflow and not effect the image quality with 23% acceleration than 4D-PACK with C-SENSE=5 and SENSELR= 3 & SENSEHF=1.5. The 4D MRA of patient with intracranial aneurysms clearly shows the blood from carotid artery through the aneurysm to distal branches(Figure 4).Conclusion
4D-PACK combined with C-SENSE=6.5 can reduce 23% acquisition time(4 min 42s) for non-contrast enhanced 4D-MRA compared with 4D-PACK with SENSE acceleration, and the excellent acceleration advantage of C-SENSE can improve the clinical application for 4D MRA. Thus, the proposed acquisition scheme for 4DMRA with C-SENSE acceleration can be potentially used for evaluating arteriovenous malformation (AVM), arteriovenous fistulas (AVF), moyamoya disease, and stroke patients.Acknowledgements
No acknowledgement foundReferences
1.Fujima N, Osanai T, Shimizu Y, et al. Utility of noncontrast‐enhanced time‐resolved four‐dimensional MR angiography with a vessel‐selective technique for intracranial arteriovenous malformations[J]. Journal of magnetic resonance imaging, 2016, 44(4): 834-845.
2.Obara M, Togao O, Beck G M, et al. Non‐contrast enhanced 4D intracranial MR angiography based on pseudo‐continuous arterial spin labeling with the keyhole and view‐sharing technique[J]. Magnetic resonance in medicine, 2018, 80(2): 719-725.
Figures