1074
Comparison of Spiral and Cartesian k space filling strategies for Time of Flight MR angiography for cervicocerebral arteries – Pilot Study
Ravi Varma Dandu1, Karthick Raj Rajendran2, Rithika Varma Dandu3, Sivakanth Nalubolu4, Kiran Barla1, Narayana Rolla5, and Indrajit Saha6
1Citi Neuro Centre, Hyderabad, India, 2Philips Healthcare, Eindhoven, Netherlands, 3RV College of Engineering, Bengaluru, India, 4Narayana Health City, Bangalore, India, 5Philips Healthcare, Bangalore, India, 6Philips Healthcare, Gurgaon, India
1Citi Neuro Centre, Hyderabad, India, 2Philips Healthcare, Eindhoven, Netherlands, 3RV College of Engineering, Bengaluru, India, 4Narayana Health City, Bangalore, India, 5Philips Healthcare, Bangalore, India, 6Philips Healthcare, Gurgaon, India
Synopsis
This study compares the performance of Time of Flight MR angiography (ToF-MRA) with spiral k-space filling and ToF-MRA with cartesian filling, for evaluation of the cervicocerebral circulation in 16 healthy volunteers. The imaging protocols were adjusted to give similar coverage and scan times for both techniques. Spiral ToF-MRA showed better visualization of almost all arteries of the cervicocerebral circulation – especially in the small distal intracranial arteries. Artefactual signal drops in segments with slow flow were also fewer with spiral ToF-MRA. Spiral ToF-MRA can potentially evaluate the cervicocerebral arterial system with higher spatial resolution than Cartesian ToF-MRA.
Introduction
Non-contrast Time of Flight MR angiography with Cartesian k space filling (cToF-MRA) is popular as a safe and effective, noninvasive screening tool for evaluation of the cervicocerebral arteries. The major drawbacks of cToF-MRA include long scanning times and its vulnerability to signal-intensity drop-out artefacts in regions of slow flow1. Although Contrast enhanced MRA is more accurate than cToF-MRA, concerns over the safety of gadolinium-based contrast material combined with the expense of the material and its administration have generated a demand for better strategies for non-contrast MRA2. On the other hand, spiral MR imaging employs a fast non-Cartesian k-space data acquisition scheme. It has found its application in cardiac imaging, coronary artery imaging and functional MRI. In this pilot study, we evaluate Time of Flight MR angiography with spiral k-space filling sToF-MRA, in comparison with time-matched cToF-MRA.Methods
The study was approved by the institutional ethical committee and informed patient consents were obtained prior to the scans. Non contrast MR angiography with Cartesian (cToF-MRA) and spiral (sToF-MRA) techniques were sequentially acquired in 16 healthy volunteers, using a 32 element head coil at 3T MR Unit (Ingenia at R5.6 software release, Philips Healthcare, Best, Netherlands). MRA was acquired in three stations covering the cervicocerebral arterial system, with the same head-foot coverage for the two techniques. The parameters for cToF-MRA and sToF-MRA were adjusted so as to match the acquisition times for each station. Total acquisition time was 4 minutes 50 seconds for cToF-MRA and 4 minutes 45 seconds for sToF-MRA. The imaging parameters are summarized in Figure 1.Full thickness rotating maximum intensity projection (MIP) images were generated from the MRA data. The images were evaluated by three radiologists with 20 years, 5 years and 2 years’ experience, blinded to the clinical history and imaging technique. Image quality was scored in 20 segments of the cervicocerebral arterial system (detailed in Figure 2). The visualization of the artery in each segment was graded by three observers blinded to each other, on a four point scale described by Koktzoglou etal3 (4 - Excellent, sharply defined arterial borders with excellent image quality for highly confident diagnosis; 3 - Good, minor inhomogeneities not influencing vessel delineation; 2 - Fair, ill-defined vessel borders with suboptimal image quality for diagnosis; and 1 - Nondiagnostic, barely visible lumen rendering the segment nondiagnostic). The presence of artefacts in each segment was also noted using a 4-point scale (0 – No artefact, 1 – Artefact causing luminal irregularity – but not stenosis, 2 – Artefact with apparent stenosis and 3 – Artefact with non-visualization of flow). Fleiss Kappa was used to assess the inter-rater agreement for visualization of the vessels.
Results
The result of observer rating for arterial visualization, artefacts and interrater agreement are summarized in Figure 2.Arterial visualization was rated to be better with sToF–MRA than with cToF-MRA in almost all segments of the cervicocerebral arterial system (p <0.05). The rating scores on sToF-MRA were significantly better than cToF-MRA in the peripheral branches of the middle cerebral arteries (3.83 vs 2.65 for M3 segment and 3.40 vs 1.69 for M4 segment), anterior cerebral arteries (3.81 vs 2.63 for A3 segment and 3.29 vs 1.77 for A4 segment) and posterior cerebral arteries (3.58 vs 2.42 for P3 segment and 3.04 vs 1.75 for P4 segment). Average rating was poorer on sToF-MRA than cToF MRA only for the origins of the great vessels (2.90 vs 3.17). (Figure 3)
Apart from the distal branches, cToF-MRA also showed more artefactual signal drops as compared to sToF-MRA. This was best appreciated at the carotid bifurcations, M1 and M2 segments of the middle cerebral arteries and A1 segment of the anterior cerebral arteries. sToF-MRA suffered from susceptibility related signal loss in the cavernous segments of the internal carotid arteries. Artefacts in rest of the segments were comparable between cToF-MRA and sToF-MRA.
Discussion
MRA with spiral k-space filling permits evaluation of cervicocerebral arteries with higher spatial resolution than time-matched cToF-MRA. The advantages of sToF-MRA are distinctly seen in visualization of the small peripheral intracranial arteries. cToF-MRA was poor in depiction of these vessels considering the small calibre and slower blood flow velocities within them. Similarly, carotid bifurcations, M1 and M2 segments of the middle cerebral arteries and A1 segment of the anterior cerebral arteries frequently show signal loss due to in-plane saturation on cToF-MRA. The improved intravascular signal permitted better visualization of these arteries on sToF-MRA.The faster data acquisition with spiral MRA permit complete coverage of cervicocerebral arterial system with shorter scan duration. This will be of value in evaluation of patients with acute ischemic stroke. Similarly, the improvement in quality of non-contrast MR angiography offered by spiral imaging may obviate the need for contrast enhanced MR angiography for evaluation of the cervicocerebral arterial system.
Conclusion
In conclusion, this study demonstrates that ToF MR angiography with spiral k-space filling has the potential to permit the evaluation of cervicocerebral arterial system with higher spatial resolution than cToF-MRA.Acknowledgements
No acknowledgement found.References
-
Carr JC, Shaibani A, Russell E, et
al. Contrast-enhanced magnetic resonance angiography of the carotid
circulation. Top Magn Reson Imaging 2001;12:349–57.
-
Babiarz LS, Romero JM, Murphy EK, Brobeck B, Schaefer PW,
Gonzalez RG, Lev MH. Contrast-Enhanced MR Angiography Is Not More Accurate Than
Unenhanced 2D Time-of-Flight MR Angiography for Determining >70% Internal
Carotid Artery Stenosis AJNR Am J Neuroradiol 2009; 30:761–68.
- Koktzoglou I, Murphy IG, Giri S, Edelman R. Quiescent Interval Low Angle Shot Magnetic Resonance Angiography of the Extracranial Carotid Arteries. Magnetic Resonance in Medicine 2016; 75: 2072–2077.
Figures

Figure 1:
Imaging
Parameters used in the study
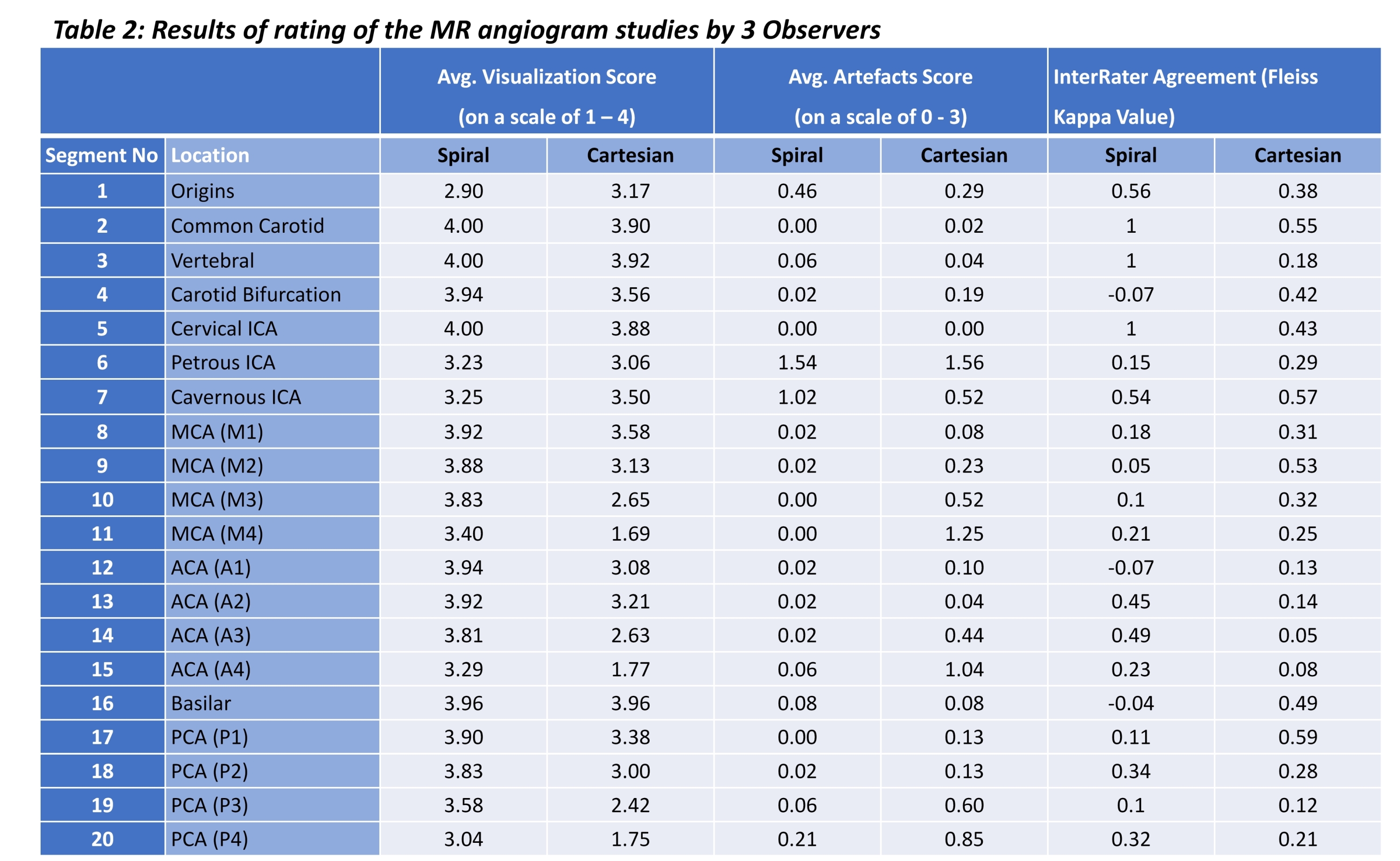
Figure 2:
Results
of rating of the MR angiogram studies by 3 Observers
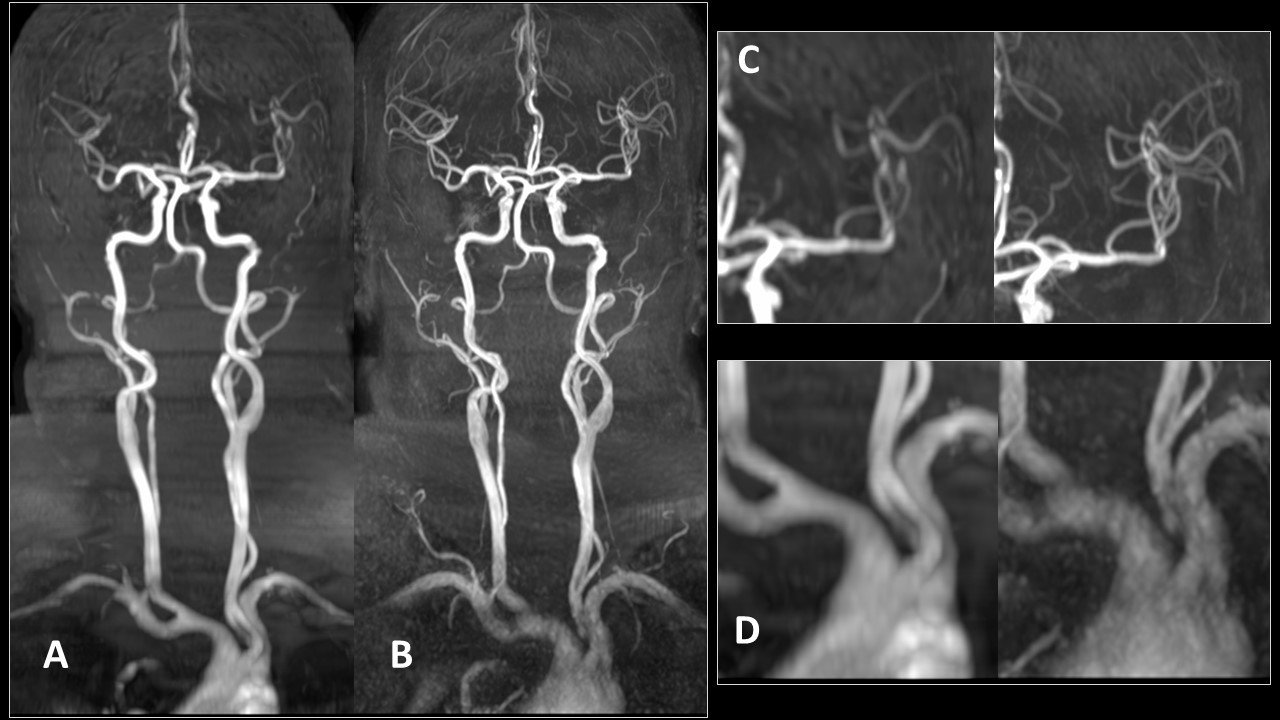
Figure 3:
MR
angiogram of cervicocerebral arterial system acquired with c-ToF MRA (A) and
s-ToF-MRA (B) techniques. Magnified view of the middle cerebral arteries (C)
shows better depiction of the M3 and M4 vessels on sToF as compared to cToF.
The origins of the great vessels however are better visualized on cToF than on
sTOF (D).