0945
Travelling kidneys: Multicentre multivendor variability of renal diffusion-weighted imaging – preliminary results1UCL Great Ormond Street Institute of Child Health, London, United Kingdom, 2Sir Peter Mansfield Imaging Centre, University of Nottingham, University Park, Nottingham, United Kingdom, 3Department of Radiology, Addenbrooke’s Hospital, Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom, 4Imaging Biomarkers Group, Department of Biomedical Imaging Sciences, University of Leeds, Leeds, United Kingdom, 5Kidney Research UK, Peterborough, United Kingdom, 6Department of Infection, Immunity and Cardiovascular Disease, University of Sheffield, Sheffield, United Kingdom, 7Neuroradiological Academic Unit, UCL Queen Square Institute of Neurology, University College London, London, United Kingdom, 8Dementia Research Centre, UCL Queen Square Institute of Neurology, University College London, London, United Kingdom, 9Wellcome Centre for Human Neuroimaging, UCL Queen Square Institute of Neurology, University College London, London, United Kingdom
Synopsis
Multicentre validation studies are required to enable clinical translation of renal MRI biomarkers. Here, we report on the feasibility of standardising renal diffusion weighting imaging protocols and on the variability of renal apparent diffusion coefficient across a range of vendors. Results suggest feasibility of implementing near-identical renal diffusion weighted imaging acquisition protocols with product sequences and the potential of the apparent diffusion coefficient as a robust metric to characterise renal microstructure in multi-centre studies.
Introduction
Important strides have recently been made in the renal MRI community to enable translation of methods to the clinic1, including on diffusion weighted imaging2. Nevertheless, the fact that multicentre validation studies (e.g. Donati et. al.3) are still sparse still hinders the widespread uptake of these methods. In this work, we report on preliminary results from a multicentre, multivendor study performed under the framework of the UK Renal Imaging Network - MRI Acquisition and Processing Standardisation (UKRIN-MAPS) project4 to assess the feasibility of standardising renal diffusion imaging protocols and the variability of renal apparent diffusion coefficient (ADC) across vendors.Methods
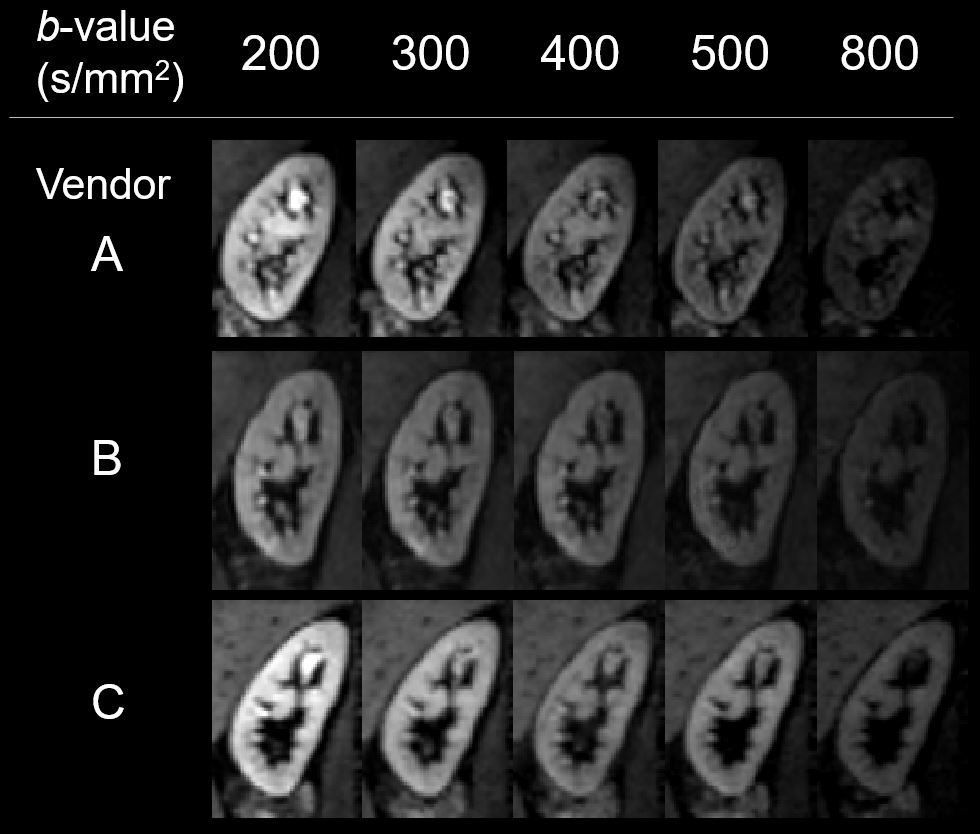
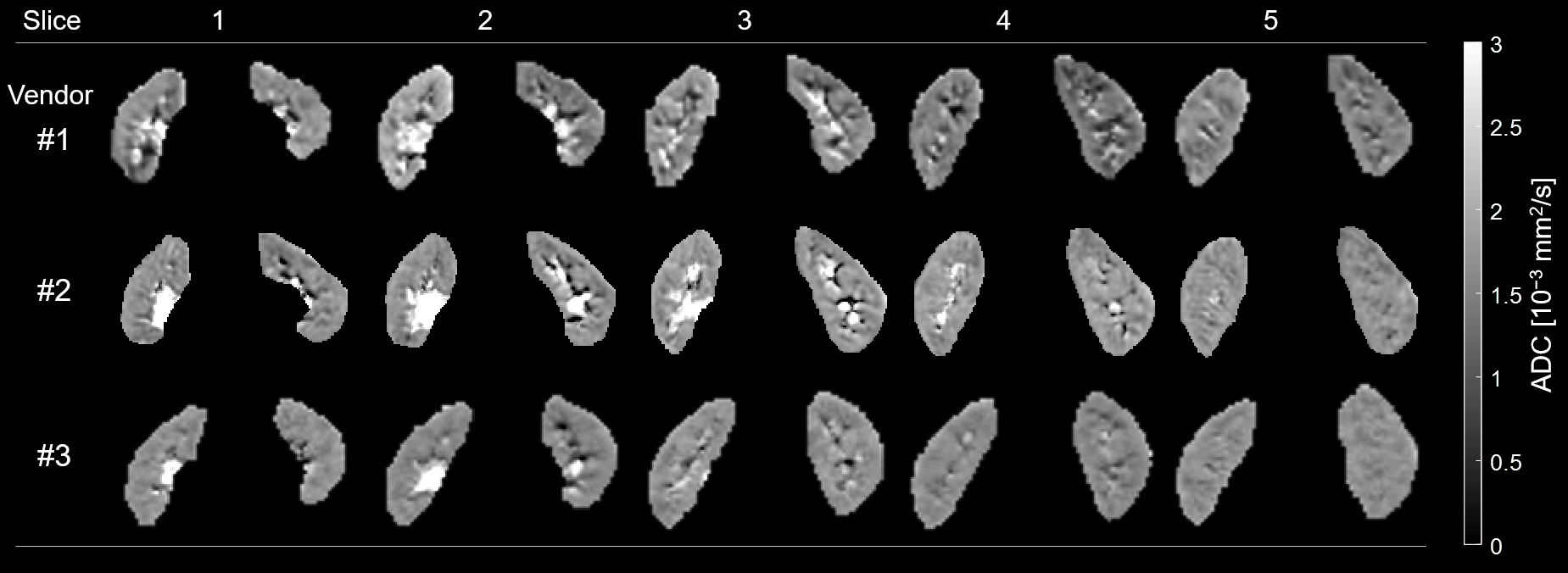
Multi-shell renal diffusion imaging scans were performed in 4 subjects (age 33±8 years) at three sites using MR systems from different vendors (Siemens, Philips, GE – henceforth referred to randomly as vendors A, B and C). The median time between scans of the same subject in each vendor was 24 days. Near-identical MR protocols were implemented in each vendor (acquisition parameters are given in Table 1). The voxelwise ADC was calculated from a linear fit by taking the natural logarithm of the diffusion-weighted signal5. Regions of interest were manually segmented based on the image with the lowest diffusion-weighting (b=200 s/mm2) and the ADC maps. ADC maps were visually inspected during segmentation to avoid including motion-corrupted voxels in the regions of interest (ROIs) (e.g. due to an inconsistent position of the kidneys during the scan). Mean ADC measures are reported across vendors/subjects and cortex/medulla (separately for left and right kidneys), as well as their coefficient of variation across vendors. A repeated measures analysis of variance (rmANOVA) was used to test for effects of vendor on ADC as well as side(left/right)-vendor interactions. The Mauchly’s test was used to verify the compound symmetry assumption for the repeated measures model.Results
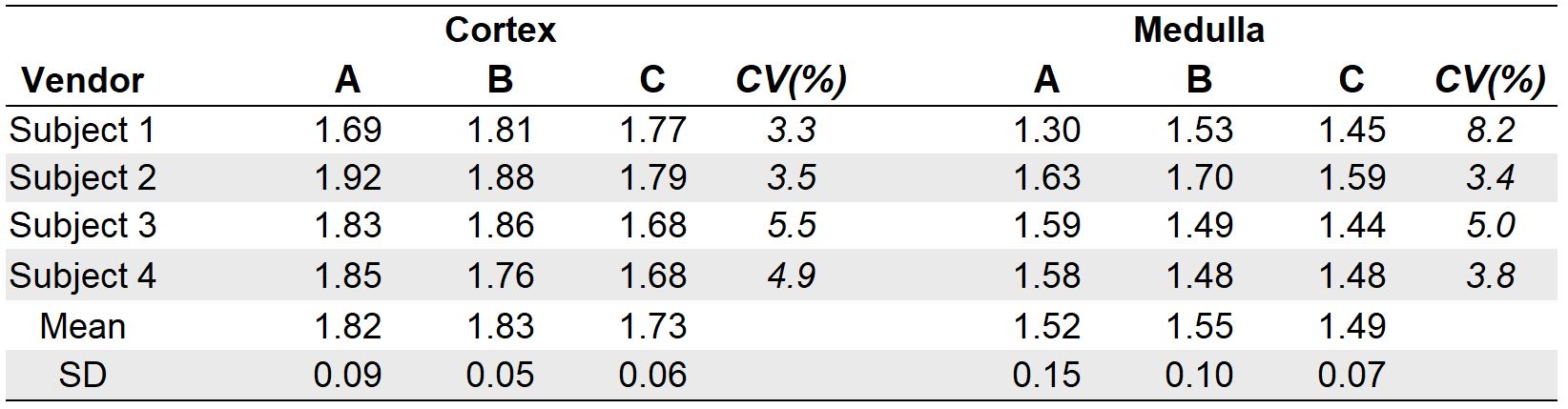
Examples of diffusion weighted images (averaged across directions/averages) from the right kidney of one subject are shown in Figure 1 for all acquired b-values. Representative ADC maps from another subject are shown in Figure 2. Across all vendors/subjects, mean ADC was (1.80±0.17)×10−3 mm2/s and (1.52±0.12)×10−3 mm2/s, respectively in the cortex and medulla. Mean ADC from each acquisition in each individual subject, for both cortex and medulla are reported in Table 2. ADC was found to be significantly higher in the cortex than in the medulla in all vendors (p<0.0001), a somewhat expected finding given that the information on the ADC maps was taken into account during ROI-drawing (as explained above). The coefficients of variation of the ADC measures across vendors ranged from 3.3 to 5.5% in the cortex and 3.8 to 8.2% in the medulla (Table 2). The compound symmetry assumption was shown to hold for our repeated measures model (Mauchly’s test, p > 0.05) and no significant effects of vendor on the ADC measure were found as well no side-vendor interaction for either cortex or medulla (rmANOVA all p-values > 0.1).Discussion
This work demonstrates the feasibility of standardising diffusion imaging protocols for ADC mapping across a range of vendors. Furthermore, these results suggest that the ADC is a robust metric without a significant variation across vendors, especially considering the minimal image processing pipeline (no motion correction/outlier rejection) and that each individuals’ physiological state was not standardized at the time of the acquisition. However, improvements in these areas will likely be necessary to obtain robust IVIM parameters such as the fast diffusion component and perfusion fraction parameters from a biexponential analysis of diffusion-weighted imaging data; this will be the focus of future work.Conclusion
Renal diffusion weighted imaging acquisition protocols were standardised across three MR vendors. Subsequently, a small cohort of healthy volunteers were scanned and shown to have repeatable renal ADC values across vendors, showing its potential as a robust metric to characterise renal microstructure in multi-centre studies.Acknowledgements
This work is funded by MRC Partnership grant MR/R02264X/1.References
1. Mendichovszky, I. et al. Technical recommendations for clinical translation of renal MRI: a consensus project of the Cooperation in Science and Technology Action PARENCHIMA. Magn. Reson. Mater. Physics, Biol. Med. (2019). doi:10.1007/s10334-019-00784-w
2. Ljimani, A. et al. Consensus-based technical recommendations for clinical translation of renal diffusion-weighted MRI. Magn. Reson. Mater. Physics, Biol. Med. (2019). doi:10.1007/s10334-019-00790-y
3. Donati, O. F. et al. Diffusion-weighted MR Imaging of Upper Abdominal Organs: Field Strength and Intervendor Variability of Apparent Diffusion Coefficients. Radiology 270, 454–63 (2014).
4. Francis, S. et. al. UK Renal Imaging Network (UKRIN): MRI Acquisition and Processing Standardisation (MAPS). (2018). Available at: https://www.nottingham.ac.uk/research/groups/spmic/research/uk-renal-imaging-network/ukrin-maps.aspx. (Accessed: 10th July 2019).
5. Garyfallidis, E. et al. Dipy, a library for the analysis of diffusion MRI data. Front. Neuroinform. 8, (2014).
Figures