0833
Parallel imaging compressed sensing in fully balanced SSFP for prostate brachytherapy MRI without an endorectal coil: a prospective study1Imaging Physics, University of Texas MD Anderson Cancer Center, Houston, TX, United States, 2Radiation Oncology, University of Texas MD Anderson Cancer Center, Houston, TX, United States, 3Diagnostic Radiology, University of Texas MD Anderson Cancer Center, Houston, TX, United States, 4Radiation Physics, University of Texas MD Anderson Cancer Center, Houston, TX, United States, 5Cancer Systems Imaging, University of Texas MD Anderson Cancer Center, Houston, TX, United States
Synopsis
Parallel imaging and compressed sensing (PICS) techniques have demonstrated the ability to accelerate MRI acquisitions in a number of clinical MRI protocols. For postimplant prostate brachytherapy MRI, an endorectal coil (ERC) is currently used to achieve images of sufficient signal-to-noise ratio (SNR) for postimplant quality assessment. Previously we retrospectively demonstrated the feasibility of using PICS to accelerate postimplant prostate brachytherapy MRI. In this work, we prospectively demonstrate that combining PICS with fully balanced steady-state free precession MRI enables high resolution and high SNR images of the prostate without an ERC.
Introduction
The standard of practice for imaging after low-dose-rate (LDR) prostate brachytherapy relies on computed tomography (CT) because of the high contrast it provides of the implanted radioactive seeds. However, CT is limited by its poor soft-tissue contrast, which makes it difficult to delineate the prostate anatomy and surrounding normal tissues. Researchers have demonstrated the ability to use MRI alone to simultaneously image the implanted radioactive seeds, seed markers, and anatomy using a single MRI pulse sequence and an endorectal coil (ERC) for improved SNR. However, the use of an ERC has several disadvantages and is primarily limited to use by major academic centers. Previously, we retrospectively demonstrated the feasibility of using combined parallel imaging and compressed sensing (PICS) to accelerate post-implant MRI and potentially boost SNR when imaging without an ERC through multiple signal averages. The purpose of this study was to prospectively investigate PICS for postimplant prostate brachytherapy MRI without an ERC.Methods
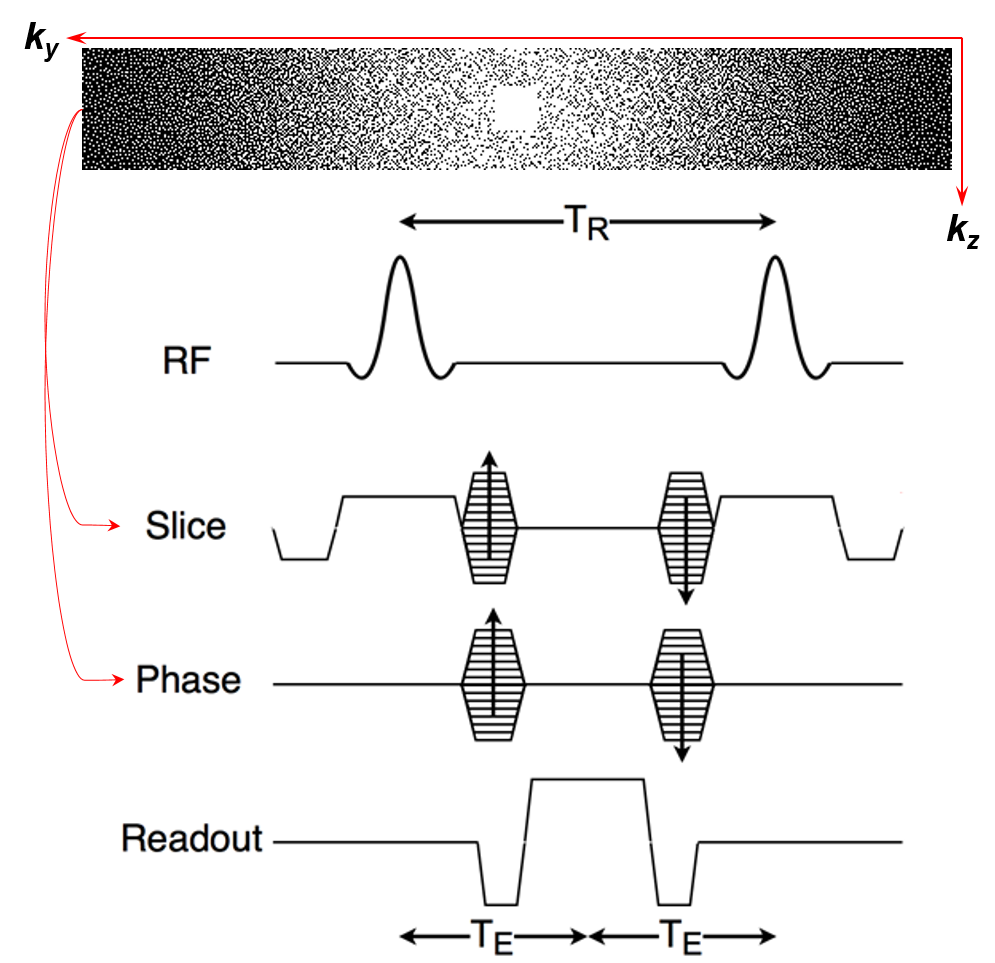
Arbitrary k-space sampling was incorporated into a 3D fully balanced steady-state free precession pulse sequence (constructive interference in steady-state, CISS) (Figure 1). The CISS sequence provides a mix of T1 and T2 contrast with high signal-to-noise ratio (SNR), enabling visualization of implanted seed markers and anatomical structures in a single acquisition. Five k-space sampling patterns were investigated including fully sampled, random, pseudo-random Poisson disk, and both single- and multi-phase encoding GRAPPA accelerations.Ten prostate cancer patients underwent LDR prostate brachytherapy with radioactive seeds stranded together with positive MR-signal seed markers [1]. The postimplant prostate cancer patients were imaged under a HIPAA compliant, IRB-approved protocol. Informed consent was acquired prior to patient imaging. Patients were imaged on a 3T Siemens Prisma scanner with two 18-channel external array coils. An ERC was not used for imaging. Typical scan parameters were: field of view = 15 × 15 cm, slice thickness = 1.2 mm, TR/TE = 5.29/2.1 ms, flip angle = 40°, readout bandwidth = 558 Hz/px, and 100% phase oversampling (left-right direction). More information about the pulse sequence and parameters can be found in prior publications [2-3]. Moderate (0.586 mm × 0.586 mm, interpolated to 0.293 mm × 0.293 mm), high (0.469 mm × 0.469 mm, interpolated to 0.234 mm × 0.234 mm), and very high (0.390 mm × 0.390 mm, interpolated to 0.195 mm × 0.195 mm) in-plane spatial resolution scans were acquired. 2-3 signal averages (NEX) were acquired at an acceleration factor (R) of 2 for each scan, with the goal of limiting scan time to 4-6 minutes to minimize motion artifacts. The k-space data of the accelerated acquisitions were reconstructed with PICS algorithms (ESPIRiT and L1-ESPIRiT) [4] using the Berkeley Advanced Reconstruction Toolbox [5], and the reconstructed k-space data were processed in the Siemens image calculation environment (ICE) to generate DICOM-compatible images.
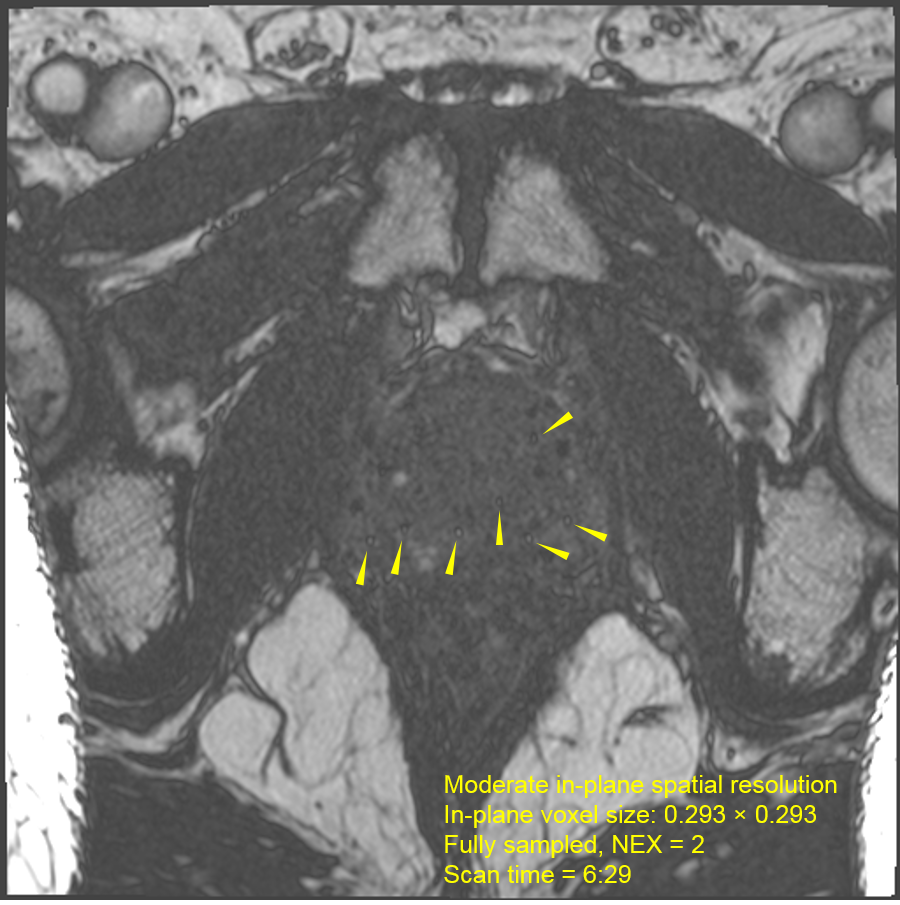
For reference, one patient was scanned on a 1.5T Siemens Aera scanner with two 18-channel external array coils and a spine coil and without an ERC. Pulse sequence parameters were similar to the above, except that only a moderate spatial resolution with NEX = 2 was acquired.
Results
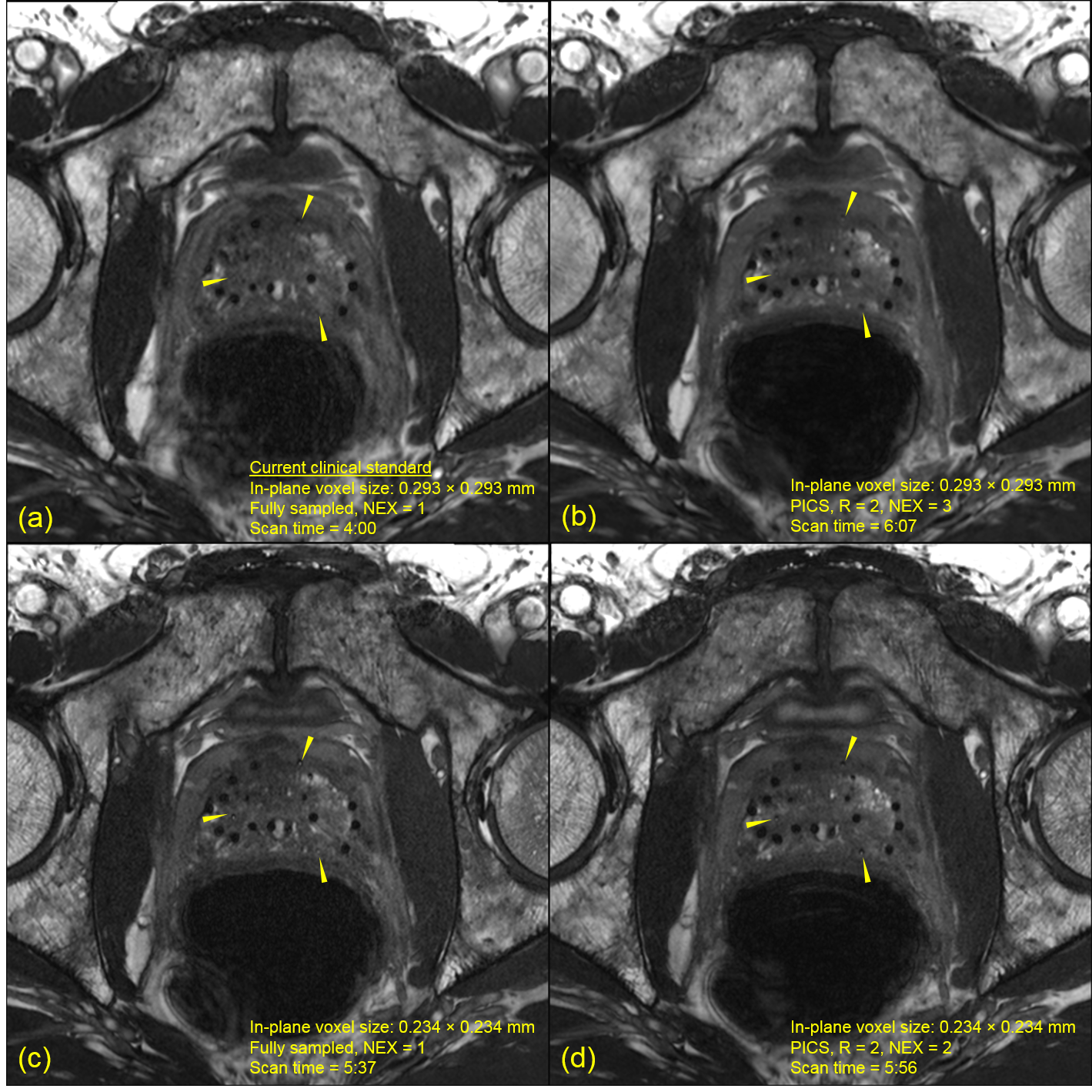
The radioactive seed markers were well visualized when imaging at 1.5T (Figure 2). However, the low CNR and SNR made it difficult to delineate the anatomical boundaries of the prostate and rectum. Acceleration in a single phase-encoding direction with a GRAPPA sampling pattern yielded the highest seed marker conspicuity (Figure 3). Additionally, including an L1 wavelet penalty into the k-space reconstruction reduced the noise amplification caused by the g-factor effect (Figure 3, ESPIRiT vs. L1-ESPIRiT). Partial volume artifacts caused some of the seed markers to be unrecognizable when imaging at the lower in-plane spatial resolution (Figure 4a). Increasing the in-plane spatial resolution mitigated these artifacts and improved overall seed marker detection and visualization at the expense of reduced SNR (Figure 4a,c). Additionally, imaging without the ERC produced inherently lower SNR than imaging with the ERC. However, the reduced SNR due to imaging at higher spatial resolution and without an ERC was compensated by the multi-NEX acquisitions that were enabled by PICS (Figure 5).Discussion and conclusion
The ability to acquire high-quality postimplant MRIs without an ERC has several advantages including reduced cost, improved patient tolerance, higher clinical throughput, and greater accessibility for community practices. We previously demonstrated the feasibility of using PICS to accelerate postimplant prostate brachytherapy MRIs retrospectively. This study confirmed the feasibility of this approach in the context of prospective clinical patient imaging. High spatial resolution images were acquired using a total scan time between 4-6 minutes, indicating the practicality of this technique for integration into routine clinical workflow. Multi-NEX acquisitions enabled by PICS provided the highest quality images for postimplant dosimetry and were superior to the clinical standard. As such, combining PICS with fully balanced SSFP enables high resolution and high SNR for prostate brachytherapy MRI without an ERC.Acknowledgements
The authors would like to acknowledge Brandy Willis and the follow MRI technologists for coordinating and performing the patient MRI exams: Stephanie Carlon, Michelle Underwood, Sandra Schuster, Asa McCoy, Jerell Jones, Vi Dinh, and Richard Triano III.References
[1] Frank SJ, Stafford RJ, Bankson JA, et al. “A Novel MRI Marker for Prostate Brachytherapy,” Int J Radiat Oncol Biol Phys 2008;71(1):5-8.
[2] Sanders JW, Song H, Frank SJ, et al. “Parallel imaging compressed sensing for accelerated imaging and improved signal-to-noise ratio in MRI-based postimplant dosimetry of prostate brachytherapy”, Brachytherapy 2018; 17(5), 816-824.
[3] Ma J, Moerland MA, Venkatesan AM, et al. “Pulse sequence considerations for simulation and postimplant dosimetry of prostate brachytherapy,” Brachytherapy 2017; 16(4):743-753.
[4] Uecker M, Lai P, Murphy MJ, et al. “ESPIRiT—an eigenvalue approach to autocalibrating parallel MRI: Where SENSE meets GRAPPA”, Magn Reson Med 2014; 71(3), 990-1001.
[5] Uecker M, Ong F, Tamir JI, et al. “Berkeley Advanced Reconstruction Toolbox,” Proc. Intl. Soc. Mag. Reson. Med. 2015;23:pp.2486.
Figures