0824
Double Echo Steady State (DESS) Cones for Non-Contrast-Enhanced Breast MRI1Radiology, Stanford University, Stanford, CA, United States, 2Electrical Engineering, Stanford University, Stanford, CA, United States
Synopsis
Breast MRI without a contrast injection has the potential to increase accessibility and compliance to the method in women who are recommended to undergo annual MRI to screen for breast cancer. Steady-state diffusion weighted methods provide robust image quality in comparison to conventional diffusion weighted methods which can suffer from variable image quality due to distortion, blurring and low-resolution. Double Echo Steady State (DESS) acquisition with a cones k-space trajectory is investigated for non-contrast enhanced breast MRI in 30 women undergoing clinically indicated breast MRIs.
Introduction
Multiple recent studies demonstrate that breast MRI could be impactful as the primary breast cancer screening modality in a much wider population of women than the highest risk population in which it is currently recommended. Eliminating the intravenous contrast injection from screening breast MRI has the potential to increase compliance in the high-risk population and possibly expand utilization of the method to a wider population of women. Diffusion-Weighted Imaging (DWI) is established as the most promising method to serve as the centerpiece of a non-contrast-enhanced breast MRI protocol. Double Echo Steady State (DESS) imaging provides robust high-resolution and distortion-free alternative to conventional DWI methods. In this work we investigate DESS with a cones trajectory for motion-robust, non-contrast breast MRI. The method is assessed in-vivo in 30 patients undergoing clinically-indicated breast MRIs.Materials and Methods
The primary advantage of steady-state diffusion weighted sequences like DESS for breast cancer screening is the more robust images quality. DESS images are distortion-free and achieve high resolution particularly through-plane with respect to conventional DWI acquisitions [1]. The inherent motion-robustness of the cones k-space trajectory (Figure 1c) eliminates coherent motion artifacts at effective b-values of 600 in comparison to Cartesian DESS acquisitions [2 – Figure 2]. Calculation of a b-value with steady-state diffusion is not as direct as with conventional DWI. With knowledge of the characteristics of tissues of interest in the breast (T1, T2, ADC) an effective b-value can be estimated. In this work we aim to achieve an effective b-value of 600 with DESS cones (Figure 1b).DESS cones was acquired in 30 patients undergoing clinically-indicated breast MRIs. All patients were recruited and consented following IRB policies. All scans were performed on a 3T GE (Signa Premier) scanner with a Sentinelle 16-channel breast coil. T2, conventional DWI, and DESS-cones were all acquired prior to the Contrast-Enhanced (CE) acquisition. Imaging parameters of the DESS-cones are as follows: 1.5 m x 1.5 mm x 3 mm, 36 cm FOV, 64 slices, 2-4 min scan time, ~600 b-value equivalent, DWI single-shot, 2.1 mm x 2.1 mm x 5.0 mm, b-value 600 s/mm2, diffusion direction 3in1, accel factor 2x. A dual-volume shim was used with both DESS cones and DWI. Analysis of DESS cones images was focused on 4 components 1) degree of motion artifacts in DESS cones images 2) depiction of tissue/lesion morphology 3) lesion-to-fibroglandular tissue contrast in comparison to DWI.
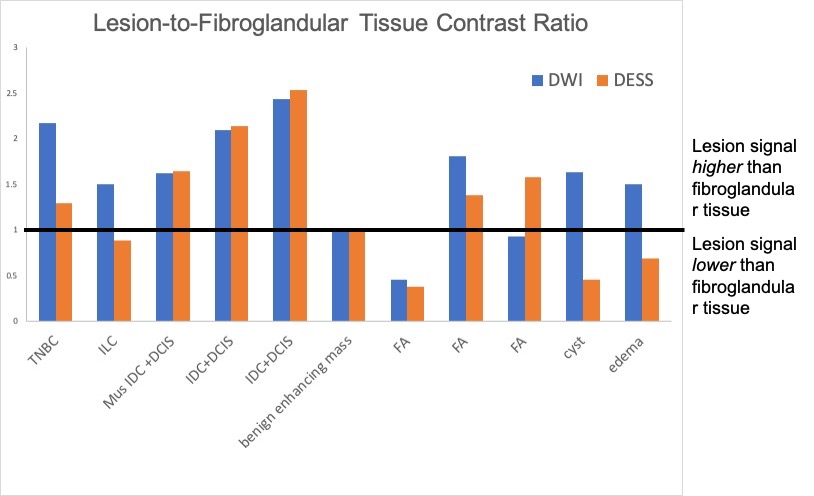
Lesion type was established based on biopsy or surgery or review of prior images. Six malignant (1 TNBC, 1 ILC, 1 DCIS, 1 Mus IDC + DCIS and 2 IDC + DCIS) four benign lesions (1 benign enhancing lesion, 3 fibroadenomas and 1 cyst) have been identified to date. Lesion-to-fibroglandular tissue signal ratios were calculated for the lesions on the DESS cones and DWI images. The DCIS case did not enhance on CE MRI and was not included in the contrast analysis. Also, a region of perilesional edema was included. A breast radiologist with 20+ years of breast imaging experience qualitatively assessed the DESS cones images for presence of motion artifact and depiction of lesion morphology in comparison to the DWI and CE images.
Results
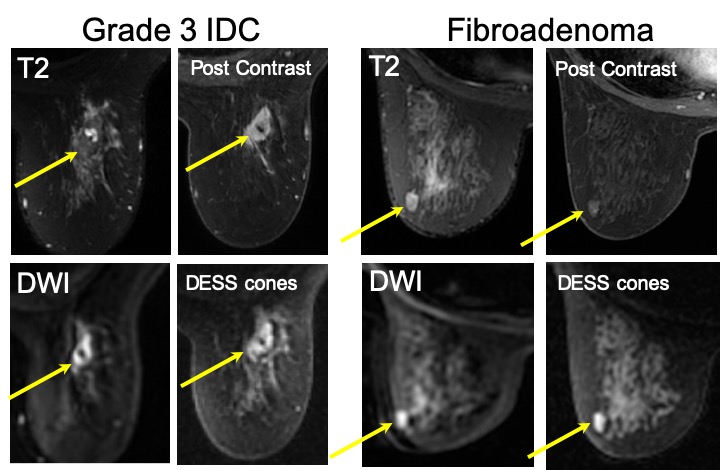
All DESS cones images were free of coherent motion artifacts (Figure 2). Lesion-to-fibroglandular tissue ratios were correlated between DESS cones and DWI in 3/5 malignant lesions and 2/5 benign lesions. Interestingly both the cyst and edema demonstrated much lower signal on DESS-cones than on the respective DWI images (Figure 3, 4). The high diffusivity and very long T2 of these tissues may be the source of suppression of signal in DESS-cones demonstrating that certain high-T2 signal lesions will not result in shine-through on the DESS images.Discussion and Conclusion
DESS implemented with a cones trajectory consistently achieves distortion-free, high-resolution images with the potential to achieve contrast reflective of that of conventional DWI methods and may suppress at least some structures that result in T2-shine through with conventional DWI. Robust image quality is of particular importance in a screening paradigm. Further studies with increased number and types of lesions will continue to elucidate the contrast of DESS cones in comparison to conventional contrast mechanisms utilized in conventional breast MRI. The flexibility of the cones trajectory to increase efficiency through extension of the readout will also be investigated.Acknowledgements
We acknowledge NIH K24-AR062068-07, R01 EB00905 and research support from GE healthcare.References
1. Granlund et al., MRI 32(4) 2014: 330-41.
2. Moran et al., 27th Annual Meeting of ISMRM, Montreal 2019, p 769.
3. Gurney et al., MRM 55 2006: 575-582.
Figures
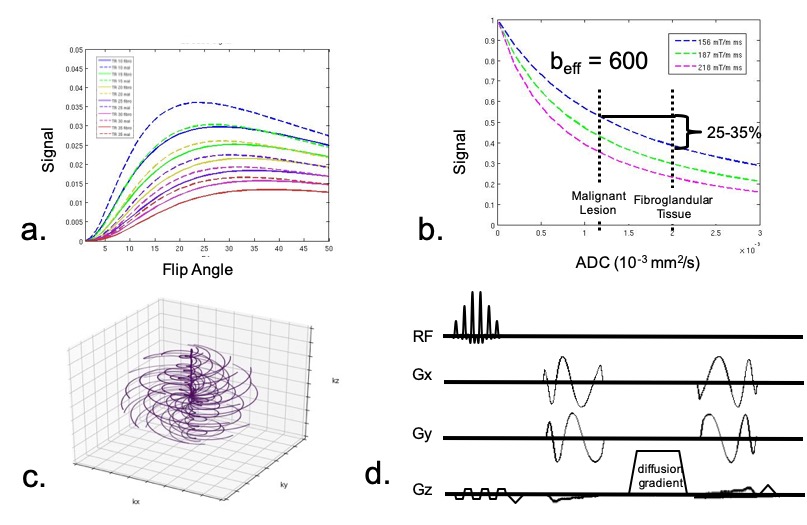

Figure 2. Coherent ghosting artifacts due to motion were eliminated with DESS cones across all 30 cases ( 3 example cases shown). There is a reduction in SNR with increasing diffusion-weighting (case c. versus case a. and b.) but normal tissue is still visible with much less restricted diffusion than would be present in a tumor.