0819
Erasing artifacts from arterial phase MRI: Motion Artifact Reduction using a Convolutional network (MARC)
Shinya Kojima1,2, Daiki Tamada 2, Tetsuya Wakayama 3, Shintaro Ichikawa 2, Hiroyuki Morisaka 4, Shigeru Suzuki 1, and Utaroh Motosugi 2
1Department of Radiology, Tokyo Women’s Medical University Medical Center East, Arakawa, Japan, 2Department of Radiology, University of Yamanashi, Yamanashi, Japan, 3MR Collaboration and Development, GE Healthcare, Hino, Japan, 4Department of Radiology, Saitama Medical University International Medical Center, Saitama, Japan
1Department of Radiology, Tokyo Women’s Medical University Medical Center East, Arakawa, Japan, 2Department of Radiology, University of Yamanashi, Yamanashi, Japan, 3MR Collaboration and Development, GE Healthcare, Hino, Japan, 4Department of Radiology, Saitama Medical University International Medical Center, Saitama, Japan
Synopsis
Motion artifact by irregular respiration disturbs accurate diagnosis in dynamic contrast-enhanced MRI of the liver. We developed a motion artifact reduction algorithm using a convolutional network (MARC). The training was performed using U-net with the arterial phase images with and without simulated artifacts. For verifying the ability of MARC algorithm, contrast-to-noise ratio measurement and visual assessment were performed in 120 cases. The image quality of arterial phase images with motion artifacts were significantly improved after applying MARC algorithm, while no particular difference was observed in the images without motion artifacts. MARC provides motion artifacts reduction without variation of image contrast.
Introduction
In dynamic contrast-enhanced MRI (DCE-MRI) of the liver, breath-hold failure causes motion artifact, which degrades the image quality and makes the diagnosis of hypervascular tumors, e.g. hepatocellular carcinoma difficult. Re-acquisition of the arterial phase images is impossible, because optimal timing of arterial phase has passed in dynamic imaging. Recently, a motion artifact reduction using convolutional neural network (MARC) was reported1. In the original report, MARC was implemented for images obtained by a differential subsampling with cartesian ordering (DISCO), which reported the significant improvement in image quality by MARC in the series of 6 arterial phase images acquired with DISCO sequence. In this study, we developed a new MARC algorithm for images acquired with a turbo liver acquisition with volume acceleration (turbo-LAVA), which is widely used for liver dynamic imaging without view-sharing technique. The purpose of this study is to demonstrate the validity of the new MARC algorithm for turbo-LAVA images.Methods
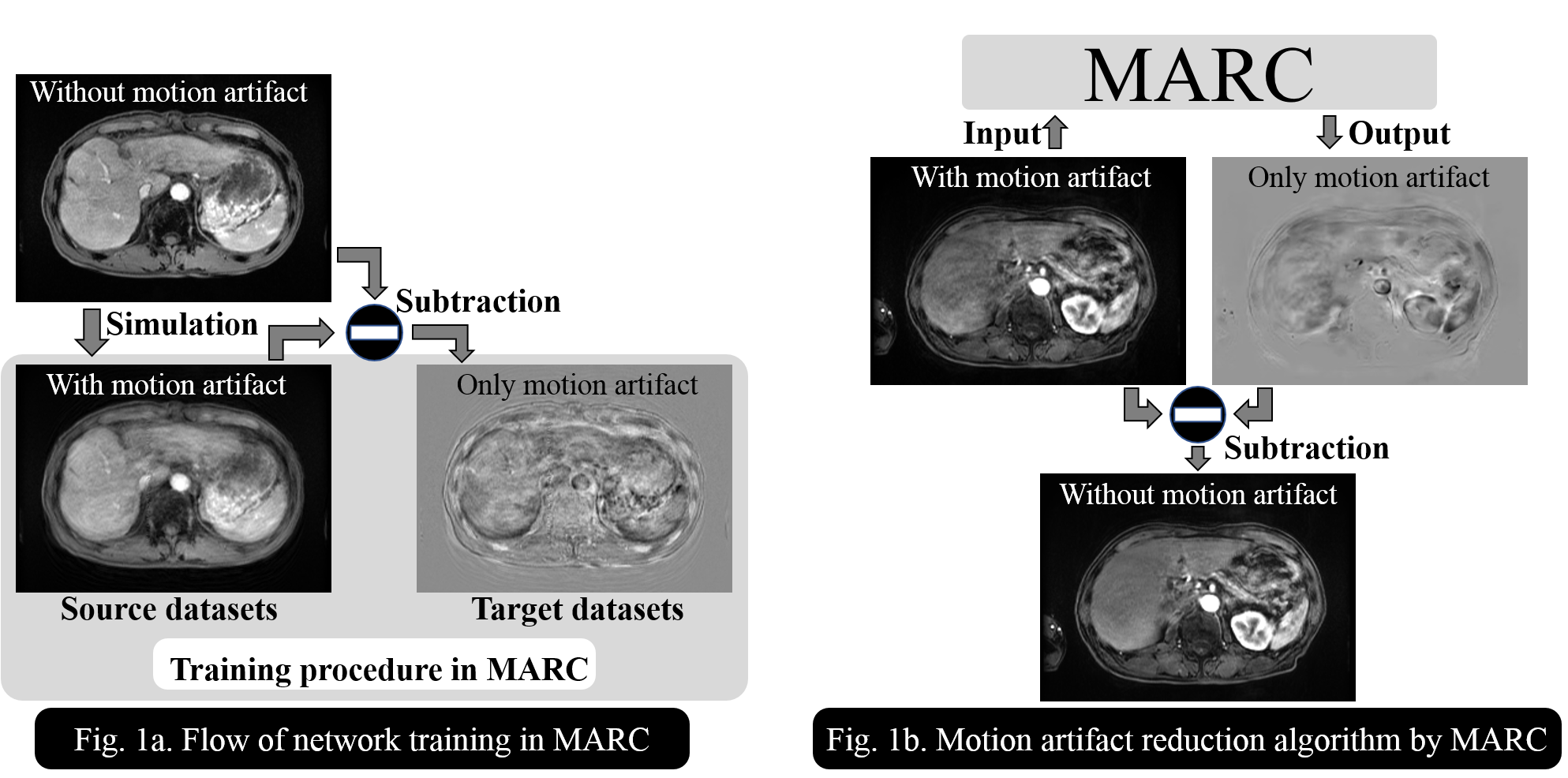
DCE-MRI was performed using turbo-LAVA at three 3-Tesla systems (SIGNA Premier, Discovery 750, and Discovery 750w, GE healthcare). U-net, which consisted of a contracting path and an expansive path2, was used in the MARC. The number of filers at each convolutional network and learning rate were optimized by a grid search method. The mean absolute error and Adam was used as loss function and optimizer, respectively. In this study, respiratory motion artifacts were simulated and added on the images without motion artifacts so as to generate images with various patterns of motion artifacts. In the network training, the subtraction image between with and without motion artifacts was set as target image and the image with the simulated motion artifacts was set as the source image, respectively, (Fig. 1a). A total of 74328 training datasets were generated from 22 patients. To remove motion artifacts, MARC algorithm was applied to the image with actual motion artifacts to extract motion artifacts, and then the final image without motion artifacts was obtained by subtracting the extracted motion artifacts from the actual image (Fig. 1b). For the validation of MARC algorithm, 120 arterial phase images from 120 patients, which were different from the training data set, was used. All patients underwent a DCE-MRI of the liver with turbo-LAVA for the clinical purpose in our institution. A study coordinator reviewed the original arterial phase images to divide them into two groups; motion artifact present (n=22) and absent (n=98). The MARC was applied to all arterial phase images. For contrast-to-noise ratio (CNR) measurement, the regions of interests were placed on the liver, pancreas, spleen, aorta, muscle, and background in the original images and the images after applying MARC algorithm. Visual assessment was carried out by two radiologists with 15 years’ experience in abdominal MRI using a 5-point scale in which score 5 represented the highest quality. A side-by-side comparison of image quality before and after MARC was also performed to evaluate which image is preferred for the image interpretation in terms of artifacts, sharpness, and overall quality. For statistical analysis, Wilcoxon signed-rank test was used and p values smaller than 0.05 were considered to indicate a statistically significant difference.Results
The representative images were shown in Fig.2; cases with (Fig.2a) and without (Fig.2b) motion artifacts in the original image. The artifacts were reduced by applying MARC algorithm especially in the case with artifacts in the original image. The CNRs of the images after MARC tended to be higher than those of the original images before MARC, but no significant difference was observed. In the visual assessment, image quality in the cases with motion artifacts was significantly improved by applying MARC algorithm (2.77 vs 3.44, p<0.05). On the other hand, the image quality scores were nearly comparable in the cases without motion artifacts in the original image (4.74 vs 4.76 p=0.38). In the side-by-side comparison, both readers preferred the images after MARC in cases with motion artifacts in the original images in terms of artifacts, sharpness, and overall quality. (Fig. 5)Discussion
In this study, we developed MARC algorithm for a turbo-LAVA sequence, which is commonly used in the DCE-MRI. The CNRs were not altered after applying MARC algorithm, which indicated that image contrast can be retained even after MARC algorithm. Motion artifacts in the arterial phase images were visually reduced by MARC, which was confirmed by the two radiologists. Hence the MARC would be useful to salvage the image data corrupted by breath-hold failure of the patient. The limitations of this study can include; 1) diagnostic ability was not assessed by using pathological gold standard, 2) severe motion artifacts were not completed eliminated by the current version of algorithm. Further effort on the development and assessment would be required.Conclusion
The respiratory motion artifacts were reduced by MARC algorithm developed in this study without changing image contrast in contrast-enhanced arterial phase MR images of the liver.Acknowledgements
No acknowledgement found.References
- Tamada D, Kromrey ML, Ichikawa S, et al. Motion Artifact Reduction Using a Convolutional Neural Network for Dynamic Contrast Enhanced MR Imaging of the Liver. Magn Reson Med Sci. 2019; [Epub ahead of print].
- Olaf R, Philipp F, and Thomas B. U-Net: Convolutional Networks for Biomedical Image Segmentation. arXiv.org 2015; arXiv:1505.04597v1.
Figures
Figure
1: Flowchart and algorithm of MARC. For training procedure, image with
the simulated motion artifact and its motion artifact only image were used for
MARC training (Fig. 1a). For removing the actual motion artifacts, MARC
algorithm was applied to the actual image to extract motion artifact and obtain
the final image without motion artifacts (Fig. 1b).
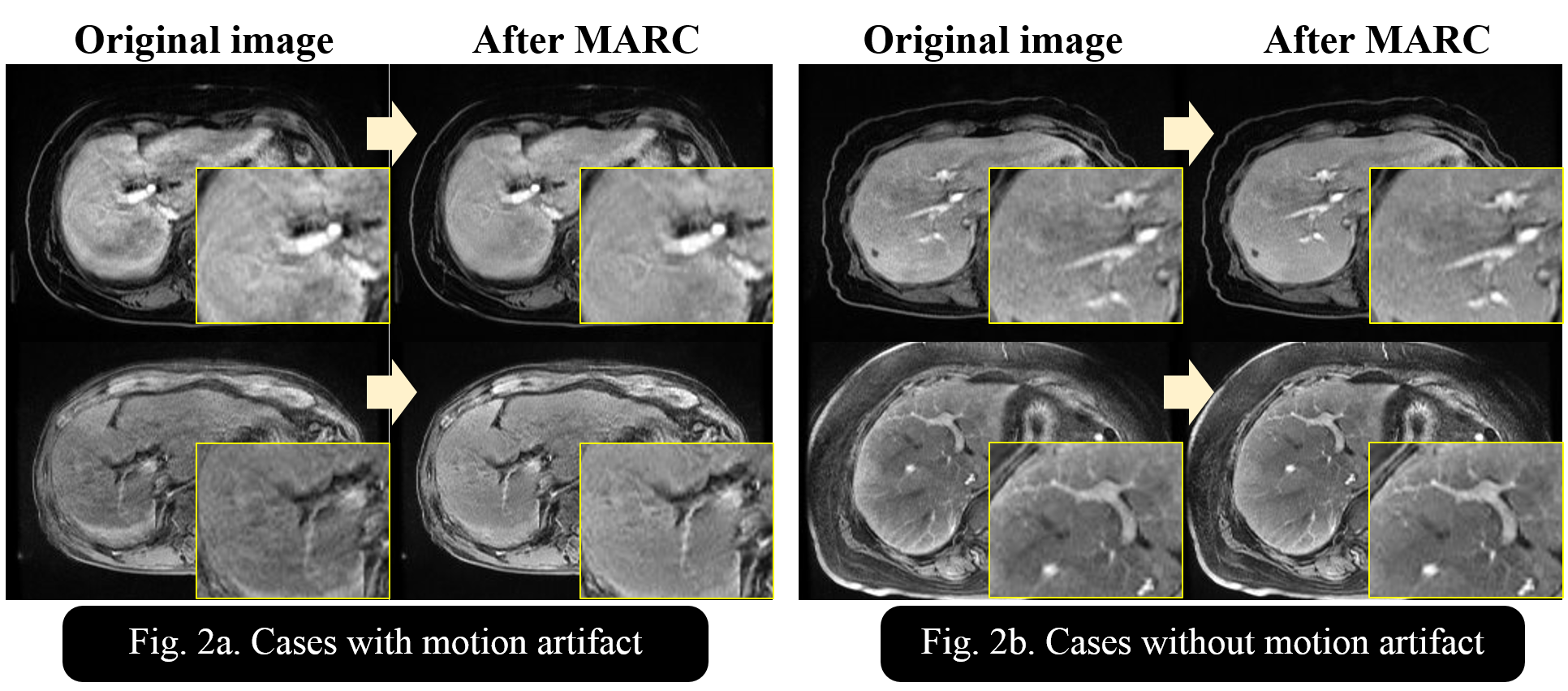
Figure 2:
The representative liver images before and after MARC in cases with (Fig. 2a)
and without (Fig. 2b) motion artifacts. Motion artifacts were obviously
reduced by applying MARC in the cases with motion artifacts.
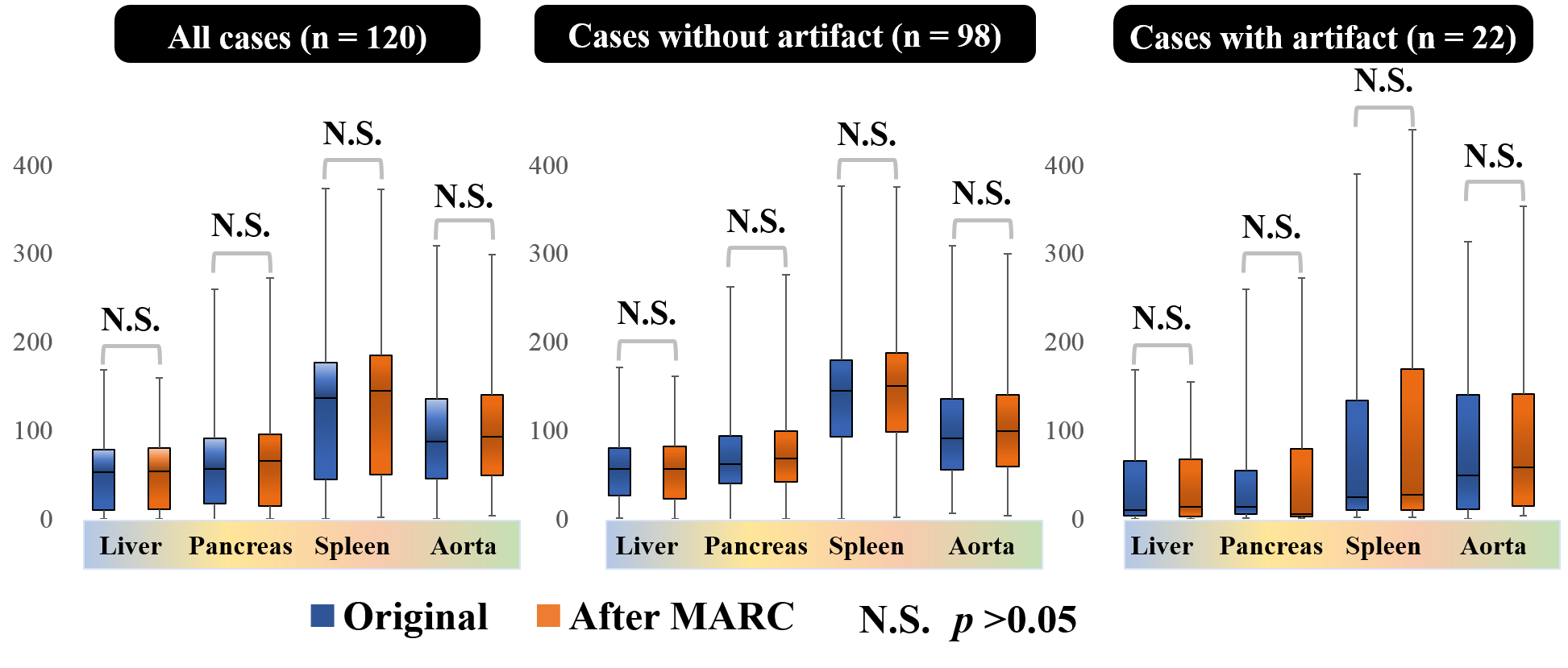
Figure 3:
Contrast-to-noise ratios (CNRs) before and after MARC at liver, pancreas,
spleen and aorta. It is suggested that MARC algorithm does not change the
image contrast.
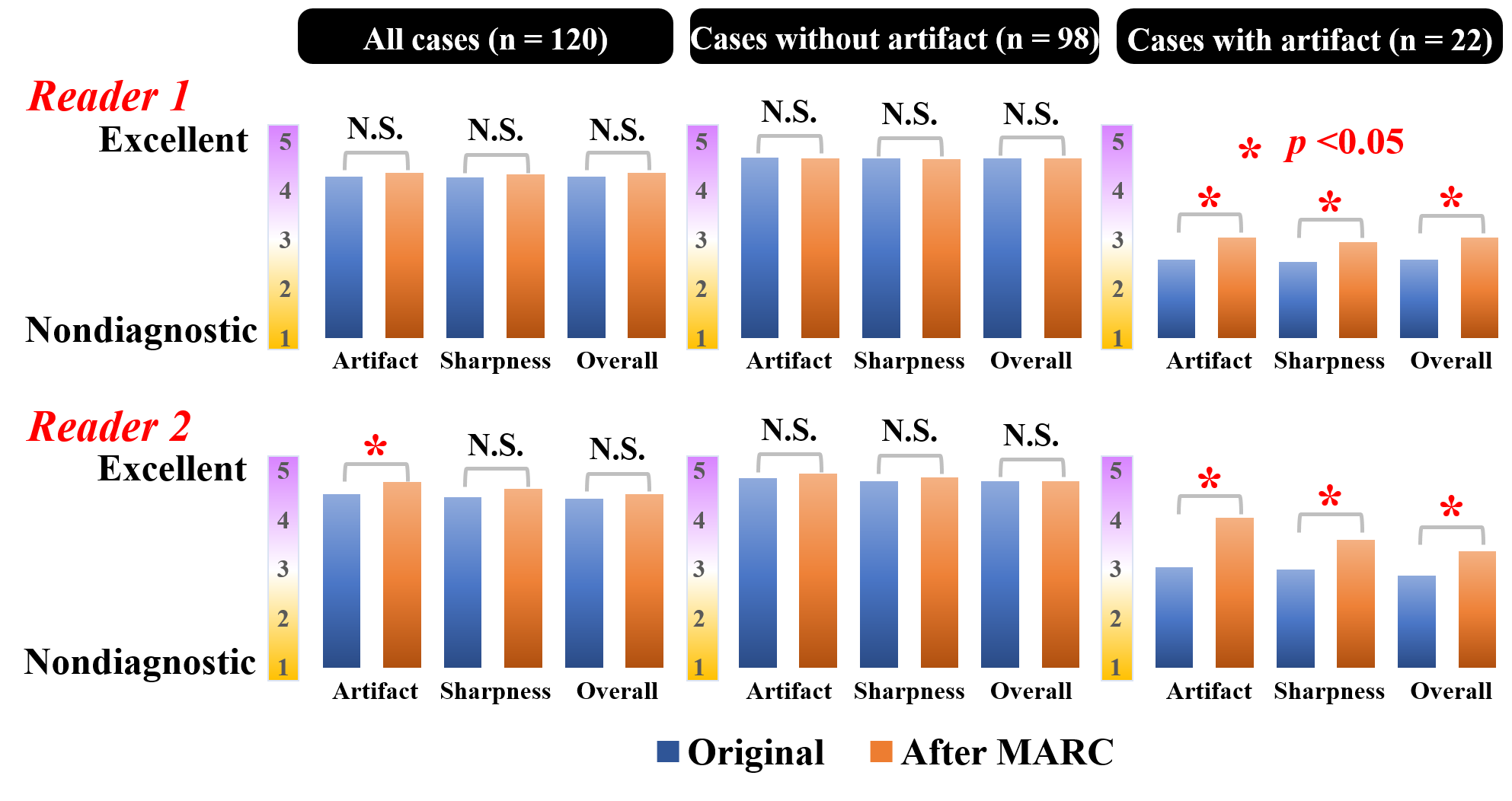
Figure 4:
Image quality scores assessed by two radiologists. In the cases with
motion artifacts, the image after MARC shows the significantly better score
compared with that before MARC.
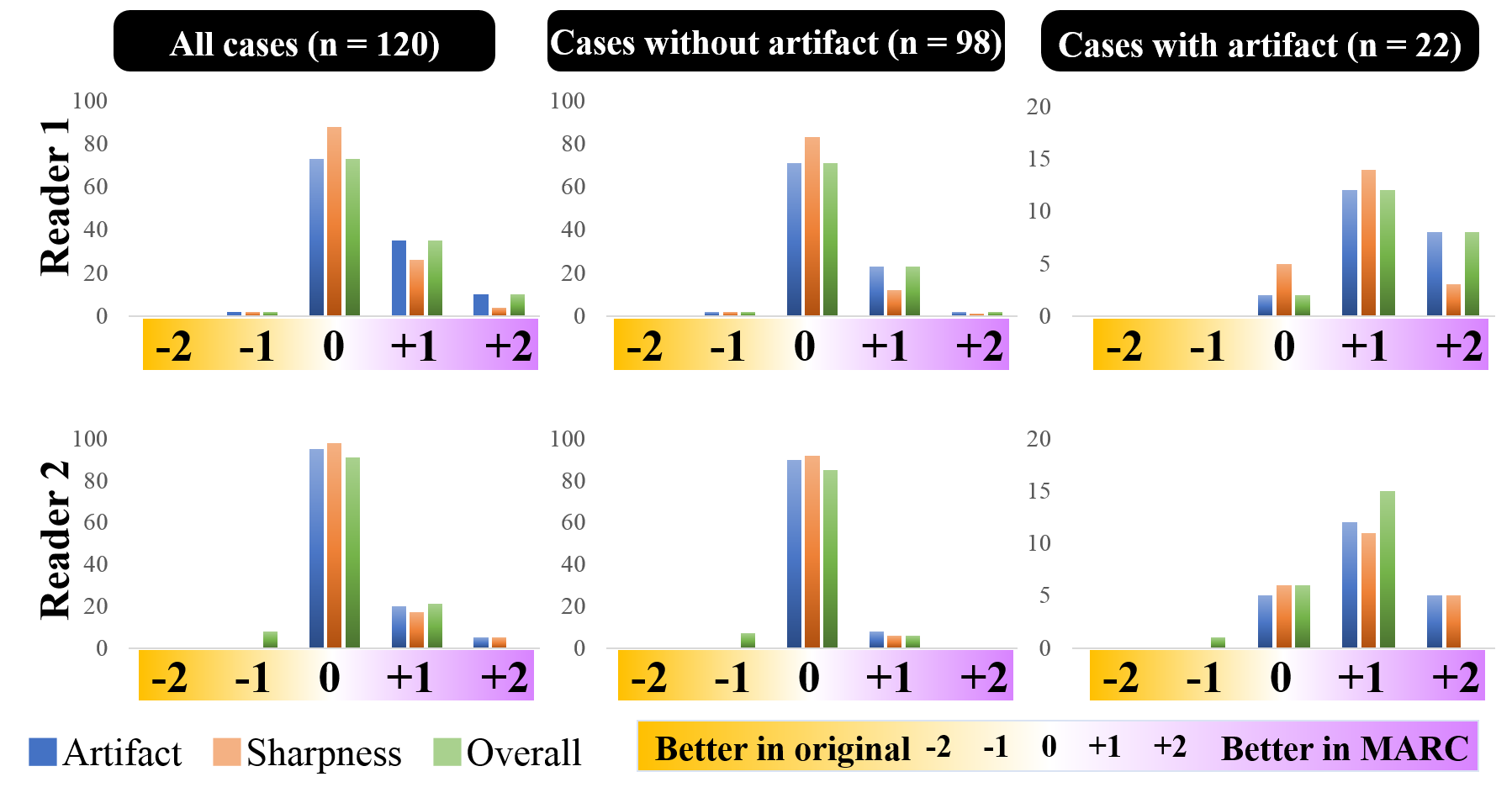
Figure 5:
Side-by-side comparison by two radiologists. Both readers preferred the
images after MARC in cases with motion artifacts in terms of artifacts,
sharpness, and overall quality.