0755
A novel RF-resonator for penile imaging1Faculty of Physics and Engineering, ITMO University, Saint-Petersburg, Russian Federation, 2Department of Radiology, Federal Almazov North‐West Medical Research Center, Saint-Petersburg, Russian Federation, 31st urology department, City Center of Endourology and New Technologies, Saint-Petersburg, Russian Federation
Synopsis
We present a new design of a radiofrequency resonator for urological applications. The resonator functions by inductively coupling to the body coil of a 1.5 T MR-scanner. This configuration of the Tx-Rx path allows increasing the transmission efficiency and signal to noise ratio (SNR) while reducing the specific absorption rate (SAR). Phantom and in-vivo imaging shows that the resonator provides around 100-fold SAR reduction and 10-fold transmission efficiency increase. Phantom imaging shows doubled SNR compared to the commercial flexible 4-element Rx coil. In-vivo imaging shows only a 50% increase in SNR, improved patient positioning and reduced the artifacts rate.
Introduction
MR imaging of the male reproductive system pathologies is a rare occurrence in clinical practice, often due to the weak fit of the standard radiofrequency (RF) coils to imaging of the penis. In order to diagnose penis-associated disorders (e.g., fractures1, Peyronie disease2 etc.) with MRI a surface coils is commonly used with the patient in supine position while penis is being fixed to the lower patient body3, which leads to the compression of the tissues, a decrease in blood flow and an uncomfortable position for the patient, provoking increased motion artifacts. In the present study, these problems have been sought to be overcome by developing a new RF resonator based on the birdcage coil operation principles4. The study presents some of the results obtained during simulation and in-vivo imaging to show that the proposed resonator in combination with a scanner body coil (BC) improves patient positioning, signal-to-noise ratio (SNR) and RF-safety.Methods
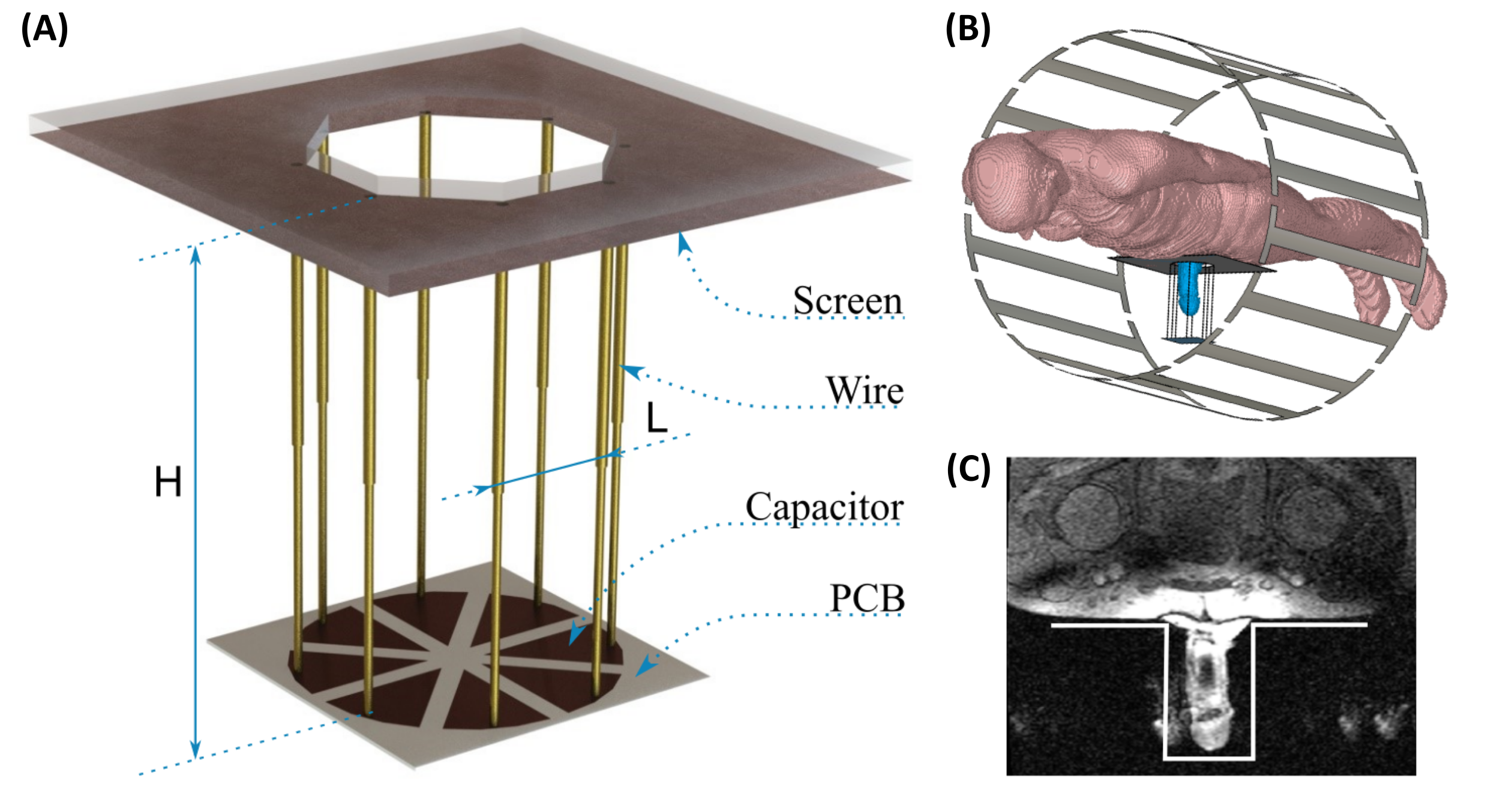
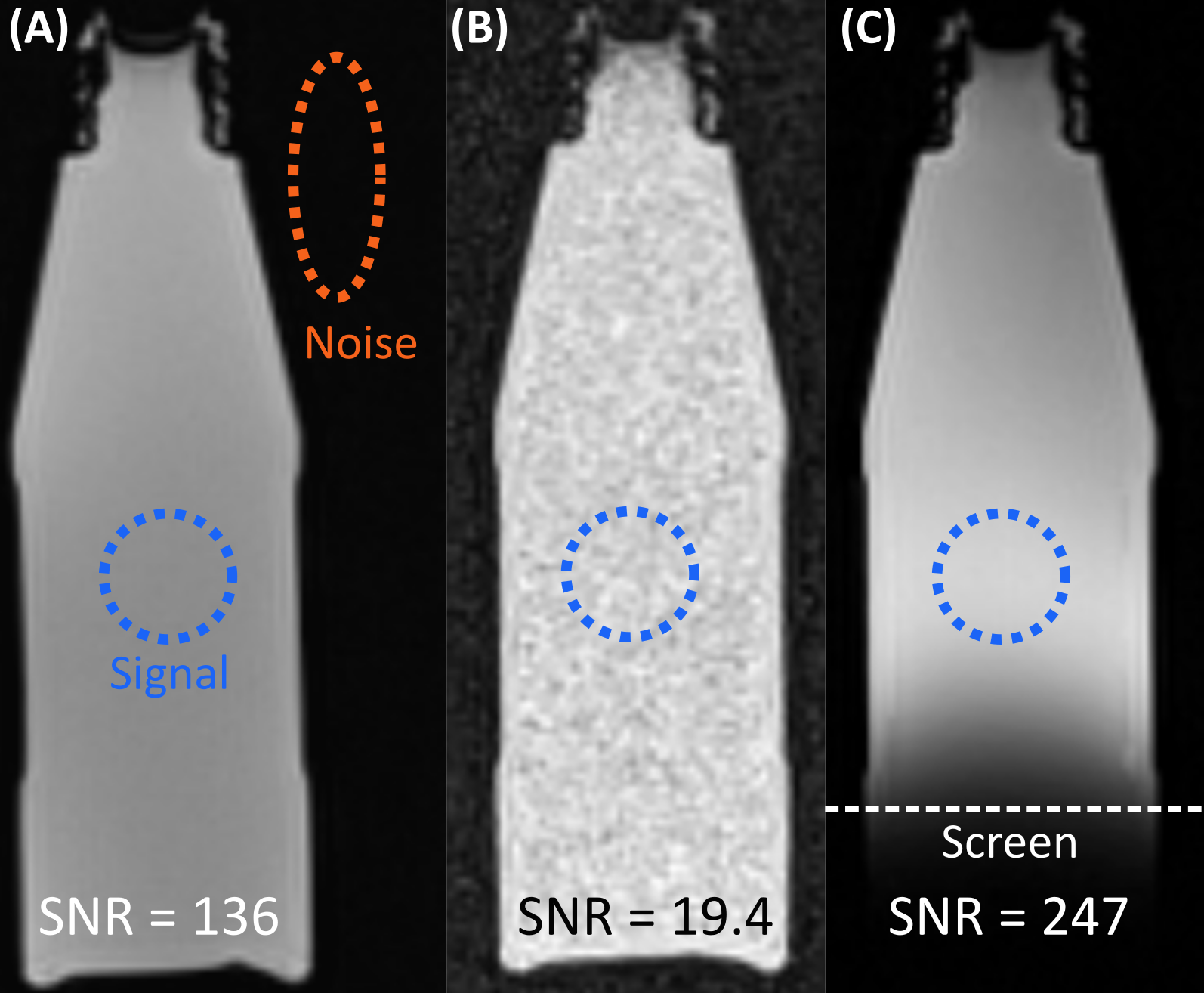
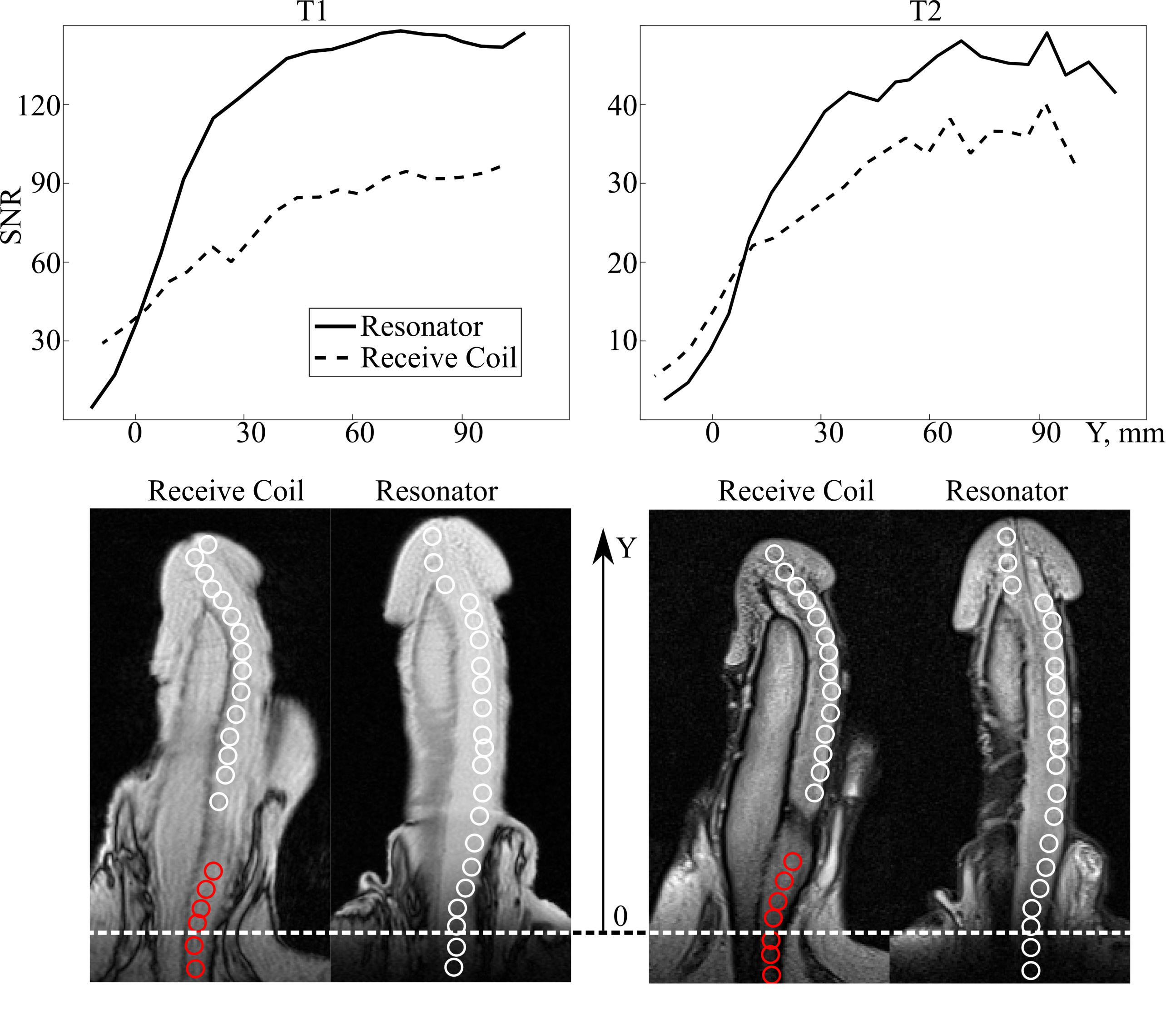
The resonator (Figure 1 A) design was based on a low-pass birdcage coil and includes 8 legs (wires) and 8 capacitors, two circle end rings of the birdcage coil are formed in the current design by a metal screen and full metallization on the opposite sides of the PCB (Rogers RO4003, thickness 0.508mm, permittivity of 3.38 and tan δ 0.0027). Geometrical parameters of the resonator were dictated by the operation frequency of 63.8 MHz and the target organ size. This led to the length of the wire H = 120mm, wire gap L = 33mm and structural capacity of the PCB capacitor of 27.5 pF. The tuning in experiments was provided via adjusting the length of the resonator legs implemented as telescopic brass tubes. The resonator operated via inductive coupling of the first eigenmode of the resonator (similar to magnetic dipole TE01δ) at the 63.8 MHz frequency to the BC of a 1.5 T MR-scanner. This configuration of the Tx-Rx path allowed increasing the transmission efficiency, SNR and reducing the SAR. The coil was initially simulated in CST Microwave Studio; coil tuning, field homogeneity and SAR (whole body and local maximum 1g SAR) levels were assessed. Electromagnetic (EM) simulations of the Tx-Rx path included realistic BC, voxel human model with an additional penis model and the resonator under study (Figure 1 B). Next, a human subject was scanned with the proposed coil. The study was approved by the local ethics committee and the volunteer provided written informed consent. The subject was scanned in the prone position elevated above the scanner table on a specially manufactured platform, which incorporated the designed resonator. The subject’s penis was freely lowered into the resonator cavity (Figure 1 C). MR-images were obtained on a clinical MR-scanner (1.5 T Siemens Magnetom Espree) with standard gradient (FLASH, FA = 70°, TR = 710 ms, TE = 7.2 ms, matrix 384x269, slice thickness 3 mm) and spin echo (TSE, FAexc = 90°, FAref = 150°, TR = 5300 ms, TE = 104 ms, ETL = 23, matrix 320x275, slice thickness 3 mm) pulse sequences. Three RF configurations were considered: BC for transmission and reception, BC with resonator for transmission and reception, BC for transmission and a flexible 4-element coil for reception. When the resonator was used, the power supplied to the BC was adjusted to achieve the same B1+ field in the center of the penis. The SNR was calculated by dividing average value of the signal in corpus spongiosum along the penis length by the standard deviation of noise in signal-free regions5.Results
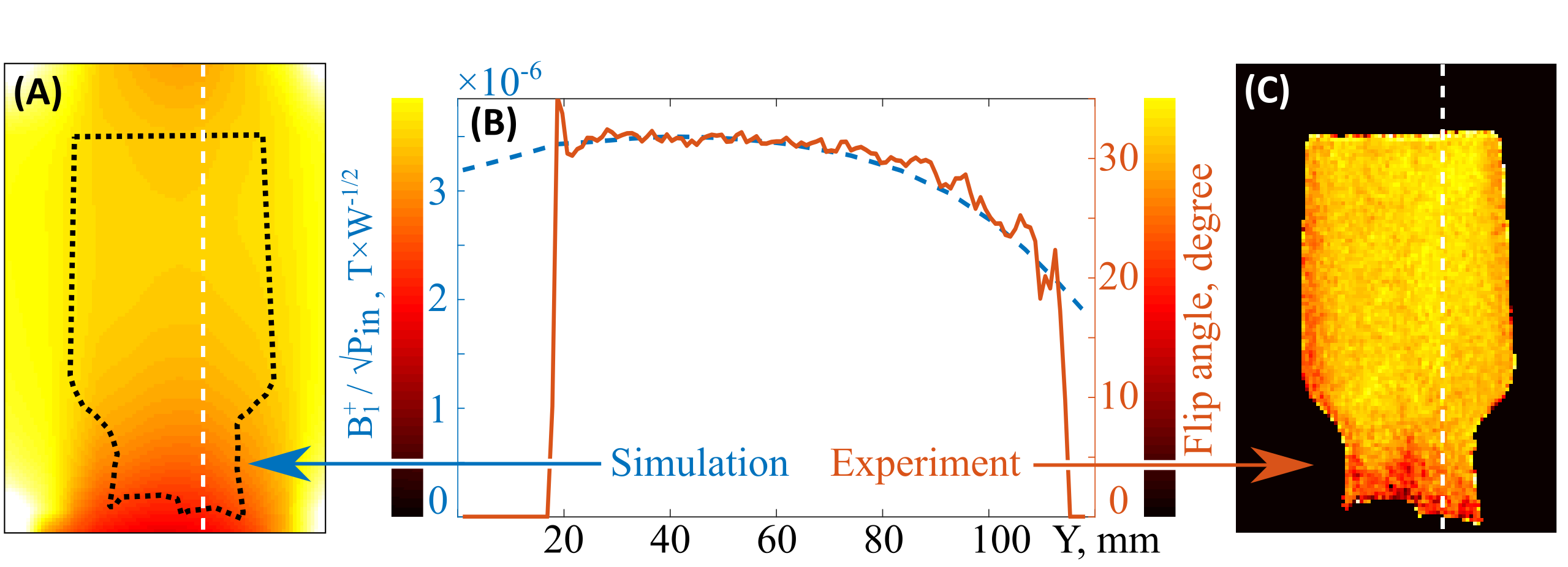
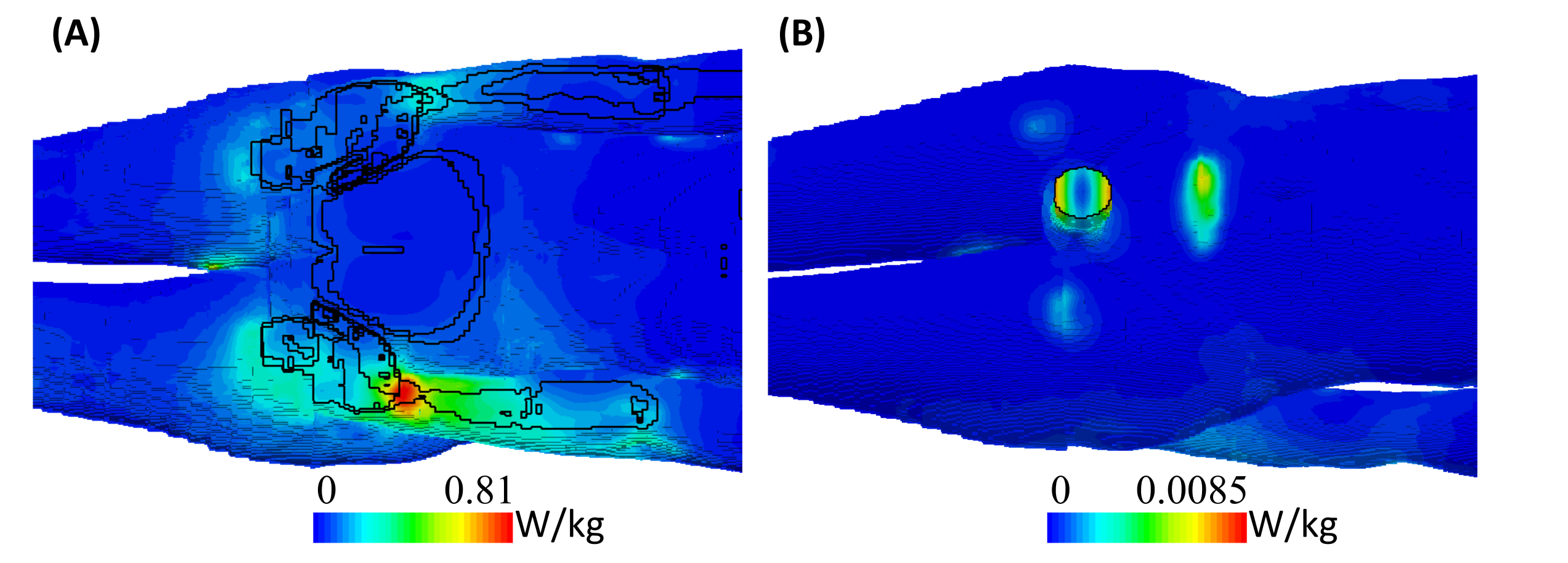
The magnetic field simulations and experimental flip angle measurements can be seen in Figure 2, showing high similarity between the simulated and experimental data (with coefficient of determination of 0.94). As can be seen, the size of the homogeneous region (i.e., where field value deviation is does not exceed 0.1 of the average field value) inside the resonator is 75 mm long. Assessment of the transmission efficiency shows a 9.8 times increase (simulation confirmed by experiment) compared to the BC-only case. Maximum (Figure 3) and whole body SAR decrease 95 and 46 times respectively. SNR measurements in phantom (Figure 4) with three different Tx-Rx path configurations show a 14-fold sensitivity gain for the resonator compared with the BC-only case, and around 2-fold increase for the resonator compared with the 4-channel flexible coil. In-vivo measurements (Figure 5) show only 27% SNR increase when comparing the resonator against the flexible 4-channel coil in T1-weighted images and 50% rise in T2-weighted images. Finally, MR-images of the penis obtained with the resonator contain fewer motion artifacts due to a more comfortable patient positioning and smaller sensitivity to flow and motion outside the imaging region.Conclusion
It was demonstrated here that using the proposed RF resonator design in urology and andrology MRI applications can improve image quality when compared to the body coil and to a more clinically relevant case of surface coils. The improved image quality can be used to provide better resolution or shorter scanning times. At the same time SAR reduction shows the scanning procedure to become safer.Acknowledgements
This work was supported by the Russian Science Foundation (Grant No. 18-79-10167)References
1. Pretorius ES, Siegelman ES, Ramchandani P, Banner MP. MR Imaging of the Penis. RadioGraphics 2013; 21(1): 283–298.
2. Helweg G, Judmaier W, Buchberger W, Wicke K, Oberhauser H, Knapp R et al. Peyronie’s disease: MR findings in 28 patients. Am J Roentgenol 1992; 158(6): 1261–1264.
3. Guler I, ödev K, Kalkan H, Simsek C, Keskin S, Kilinç M. The value of magnetic resonance imaging in the diagnosis of penile fracture. International Braz J Urol 2015; 41: 325-328
4. Hayes CE, Edelstein WA, Schenck JF, Mueller OM, Eash M. An efficient, highly homogeneous radiofrequency coil for whole-body NMR imaging at 1.5 T. J Magn Reson 1985; 63(3): 622–628.
5. Dietrich O, Raya JG, Reeder SB, Reiser MF, Schoenberg SO. Measurement of signal-to-noise ratios in MR images: Influence of multichannel coils, parallel imaging, and reconstruction filters. J Magn Reson Imaging 2007; 26(2): 375-385
Figures