0589
Diffusion Kurtosis Imaging of Cervical Carcinoma: Correlation between Imaging Parameters and Histological Findings1Department of Radiology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical, Beijing, China, 2GE healthcare, China, Beijing, China
Synopsis
Cervical cancer is the leading cause of death in gynecological malignancy around the world. The most important prognostic factors include stage at diagnosis, histological subtype, tumor differentiation and et al, which are critical to make the optimal treatment strategies. However, there are still huge challenges in accurate assessment tumor characteristics even by clinical examination and biopsy. DWI has showed promising results in assessment tumor characteristics in cervical cancer. Diffusion kurtosis imaging (DKI), an extension of DWI, is more sensitive to tissue heterogeneity and water exchange. This study demonstrated that DKI-derived parameters are helpful in assessment histological features of cervical cancer.
Purpose
To prospectively investigate the additional value of diffusion kurtosis imaging (DKI) in characterization of cervical carcinoma.Method
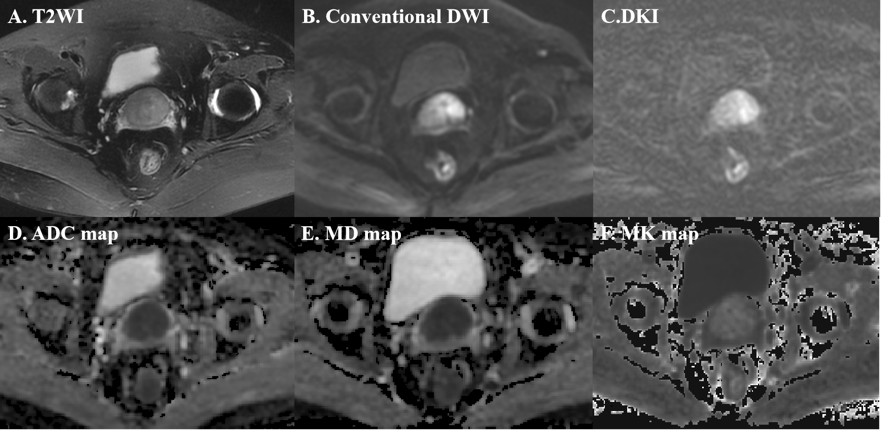
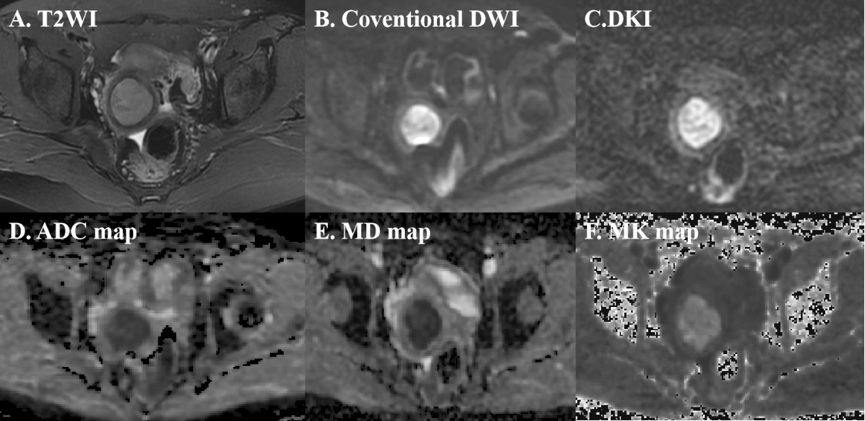
Sixty-three consecutive patients with histological-confirmed cervical cancer underwent pelvic MRI with DKI with 3 b values (0, 1000 and 2000s/mm2) prior to receiving any tumor related treatment at 3.0T MR scanner(GE Discovery 750, USA). ADC values derived from 0 and 1000s/mm2 and parameters derived from DKI including MD, a corrected apparent diffusion coefficient, and MK, the deviation of the signal decay from a monoexponential model were measured using the Function tool DKI program independently. A two-way analysis of variance (ANOVA, SPSS version 21.0, USA) was used to assess differences between histological subtypes (squamous cell carcinoma: n=44; adenocarcinoma: n=19) and grades of tumors (low grade: n=32; high grade: n=31) for each of these parameters. The Spearman correlation analysis was used to evaluate the correlation between these parameters and tumor FIGO stage, then the significant parameters were compared between groups of early stage (FIGO IB-IIA: n=24) and advanced stage (FIGO IIB and above: n=39). ROC was performed to obtain the area under the receiver operating characteristic curve (AUC) to assess the diagnostic capacities of these parameters in characterization of cervical carcinoma.Result
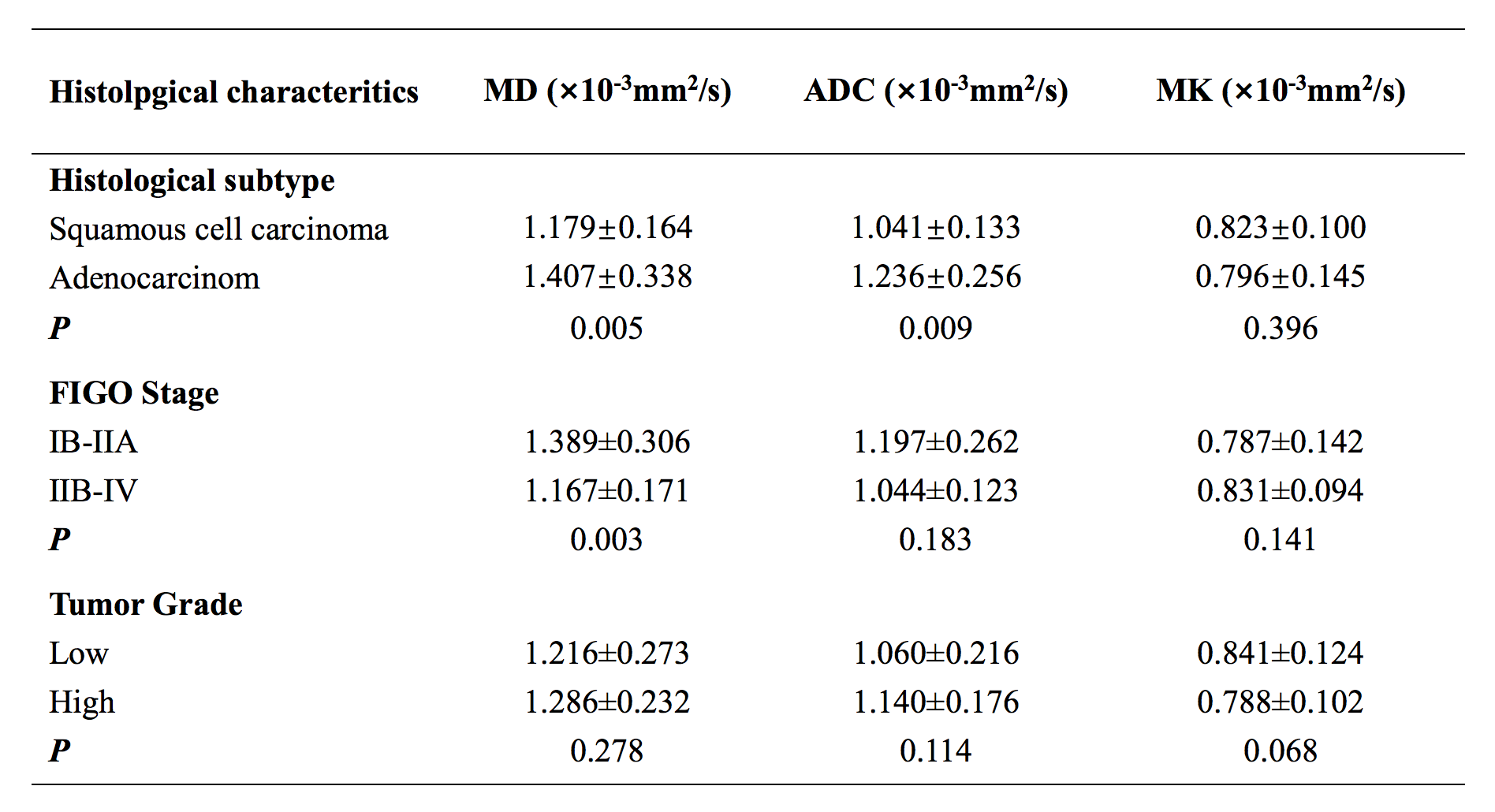
The MD and ADC values were significantly lower in squamous cell carcinoma than adenocarcinoma (P=0.005 and 0.009, respectively), but no significant differences were found between tumor grade (P=0.460). Only MD value was inversely related to tumor FIGO stage (r=-0.317, P=0.011) and there was significantly differences for MD value between tumor with early stage and advanced stage (P=0.003). Moreover, no differences were observed in MK for different pathological features tested. The ADC values showed better diagnostic performance in differentiation of tumor histological subtype with AUC of 0.749 at the optimal cut-off of 1.19×10-3mm2/s. An optimal cut-off MD values of 1.27×10-3mm2/s for distinguishing early stage and advanced stage in cervical carcinoma has a sensitivity of 79.49% , the specificity of 66.67% and the accuracy of 74.62%.Discussion and Conclusion
The significant differences of MD and ADC values were observed in this study between squamous cell carcinoma and adenocarcinoma indicating that these parameters were sensitive to microstructure properties of tumors, which was consistent to some previous studies. In addition, only MD was significantly lower in tumor with advanced stage than those with early stage in cervical carcinoma likely related to the more restricted water diffusion in advanced stage tumor with more cellular packed tumor environment, which added value over conventional DWI for staging cervical carcinoma. Overall, MD and ADC provide further and more complementary information in differentiating histological subtype and FIGO stage for cervical carcinoma aiding in confidence in diagnosis and staging tumor in clinic.Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.References
[1] Wang M, Perucho J, Chan Q, et al. Diffusion Kurtosis Imaging in the Assessment of Cervical Carcinoma[J]. Acad Radiol,2019.
[2] Zhu L, Pan Z, Ma Q, et al. Diffusion Kurtosis Imaging Study of Rectal Adenocarcinoma Associated with Histopathologic Prognostic Factors: Preliminary Findings[J]. Radiology,2017,284(1):66-76.
[3] Wang P, Thapa D, Wu G, et al. A study on diffusion and kurtosis features of cervical cancer based on non-Gaussian diffusion weighted model[J]. Magn Reson Imaging,2018,47:60-66.
[4] Bai Y, Lin Y, Tian J, et al. Grading of Gliomas by Using Monoexponential, Biexponential, and Stretched Exponential Diffusion-weighted MR Imaging and Diffusion Kurtosis MR Imaging[J]. Radiology,2016,278(2):496-504.
Figures