0570
Differentiating benign from malignant breast lesions: a feasibility study with synthetic MRI1The second affiliated hospital of xi 'an jiaotong university, xi an, China, 2MR Research, GE Healthcare, Beijing, China
Synopsis
In this study, we aim to investigate the feasibility of quantitative measurements obtained from magnetic resonance image compilation (MAGIC) MRI technology in the breast lesions and to further evaluate the application value of quantitative measurements in differentiating malignant from benign breast lesions. It was concluded that quantitative T2 relaxation time and PD value measured by MAGIC-MRI sequence can be applied in the breast lesions. The measured lower quantitative T2 and PD value is closely related to breast malignancy, which worth further study.
Introduction
Breast cancer is the most common malignant tumor in women[1]. Early detection and early diagnosis can effectively improve the survival rate of breast cancer patients[2]. Magnetic resonance imaging(MRI) has a higher sensitivity , comparing to mammography and ultrasound [3]. However, differential diagnosis of benign and malignant breast lesion requires dynamic contrast-enhanced (DCE) MR imaging, which is costly, time consuming, and even risky for certain populations, given the recent discovery that gadolinium has been found to accumulate in the brain [4]. Diffusion weighted imaging has controversial specificity for the significant overlap between malignant and benign lesions. Biopsy is invasive and can’t assess comprehensively for the heterogenous breast cancer. Furthermore, all of the aforementioned techniques are subjective. On the contrary, the quantitative measures from recent proposed synthetic MR imaging technique, termed as magnetic resonance image compilation (MAGIC), is simple, noninvasive, comprehensive, objective and time-effective. MAGIC-MRI can obtain the tissues’ quantitative maps of T1,T2 relaxation time and proton-weighted image (PD) in about six minutes. The purpose of this study is to preliminarily investigate the performance of quantitative measurements derived from MAGIC-MRI in patients with breast lesions and to further assess the application value of quantitative measurements in differentiating malignant from benign breast lesions.Material and Methods
From May 2019 to Oct 2019, 83 patients(82 female, 1 male), ranging from 23 to 75 years old (46.9±10.6years) were retrospectively included in our study. All breast lesions were confirmed by biopsy, surgical pathology or clinical diagnosis. Among them, 36 pathological confirmed patients were further divided into benign and malignant groups (9 benign,27 malignant), ranging from 29 to 75 years old (48.6±11.1years). All subjects underwent MR exams on a 3.0T whole body scanner (Signa Pioneer, GE Healthcare, WI, US) with an 8-channle breast coil. Scanning sequence included axial (Ax) T2 and T1 weighted imaging, Ax diffusion imaging, Ax MAGIC and DCE imaging. The MAGIC parameters were as follows: TR=6000ms, two echo times (TEs, 21.6 and 108 ms), four delay times (146, 546, 1879, and 3879 ms), Bandwidth=25kHz, number of average=1, FOV=34cm×34cm, slice thickness/gap=5/1mm, 31 axial slices, echo train length=16, matrix=320×224, SENSE acceleration factor=2, and scanning time = 6.01mins. The quantitative measurements, including T1, T2 and PD maps were generated from the raw data produced by MAGIC imaging sequence using a vendor-provided program (MAGiC, version 100.1.1). The region of interest (ROI) was prescribed to cover the largest area of the breast lesion. Statistical analysis of two independent sample t tests was selected was selected providing the data satisfies the normal distribution, otherwise Kruskal-Wallis was used.Results
There are totally 74 patients (73female,1male) whose breast lesions could be measured on quantitative maps, while 8 patients are excluded due to their lesions may be hyperplasia with smaller than 0.5cm and another 1 patient for the lesion are scattered with less than 0.5cm after neoadjuvant. The characteristics of the parameters are shown in table 1. Among them, 36 patients are divided into benign and malignant groups (9 benign,27 malignant, Figure 1A,B) to investigate the differential diagnostic value of T1, T2 and PD (Table 2). Of these, 28 lesions are masses and 8 lesions are non-masses. Our results indicate the value of T2 and PD are significantly different between benign and malignant breast lesions (p<0.01) and their diagnostic efficacies are shown in table 1,figure 2. The areas under the receiver operating characteristic curve (AUC) for T2 and PD values are 0.91 and 0.94 respectively. The T2 is with the higher sensitivity while the PD value’s specificity is higher(1.00,0.96 respectively). However, T1 value does not demonstrate significant difference between benign and malignant lesions.Discussion and Conclusion
Main finding in our study is that quantitative T2 relaxation time and PD values derived fromMAGIC MRI can be applied in patients with breast lesions, which is in accordance with studyconducted by YongsIk and his colleagues. However, we included both benign and malignantlesions, while they only investigated cancers[5]. In our study, both the T2 and PD value havesignificant potential in identifying benign from malignant breast lesions. Observed mean T2relaxation time of malignant breast lesion was lower than that of benign lesions, 84.8 vs 118.5 ms. We speculate that large size of cancer cells with abundant cytoplasm, lymphocyte/plasma cellinfiltrations and necrotic materials in the intercellular space might cause reduced extracellularspace and reduced free water content, which could account for the shorter T2 relaxation time inmalignant breast lesions. Our results are consistent with Li et, al, [6]. However, we assessed notonly the mass lessons but also the non-mass lesions. One of the major limitations in our study isthe relatively small number of lesions. Hence future study with bigger cohort of subject iswarranted. To conclude, quantitative measurements obtained from MAGIC-MRI can be applied inthe breast lesions and differentiating benign from malignant breast lesions.Acknowledgements
No acknowledgement found.References
[1] Freddie B, Jacques F, Isabelle S, et al. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries [J].CA Cancer J Clin, 2018, 68(6):394-424.
[2] Byers T, Wender RC, Jemal A, et al. The American Cancer Society challenge goal to reduce US cancer mortality by 50% between 1990 and 2015: Results and reflections [J].CA Cancer J Clin, 2016, 66(5):359-369.
[3] Santamaría G, Bargalló X, Fernández PL, et al. Neoadjuvant Systemic Therapy in Breast Cancer: Association of Contrast-enhanced MR Imaging Findings, Diffusion-weighted Imaging Findings, and Tumor Subtype with Tumor Response. Radiology. 2017 Jun;283(3):663-672.
[4] Kanda T, Nakai Y, Oba H, Toyoda K, Kitajima K, Furui S. Gadolinium deposition in the brain. Magn Reson Imaging 2016;34(10):1346–1350.
[5]Jung Y, Gho SM, Back SN, et al. The feasibility of synthetic MrI in breast cancer patients: comparison of T2 relaxation time with multiecho spin echo T2 mapping method. Br J Radiol. 2018 Sep 21:20180479
[6]Liu 1, Yin B, Shek K, et al. Role of quantitative analysis of T2 relaxation time in differentiating benign from malignant breast lesionsInt Med Res. 2018 May;46(5):1928-1935.
Figures
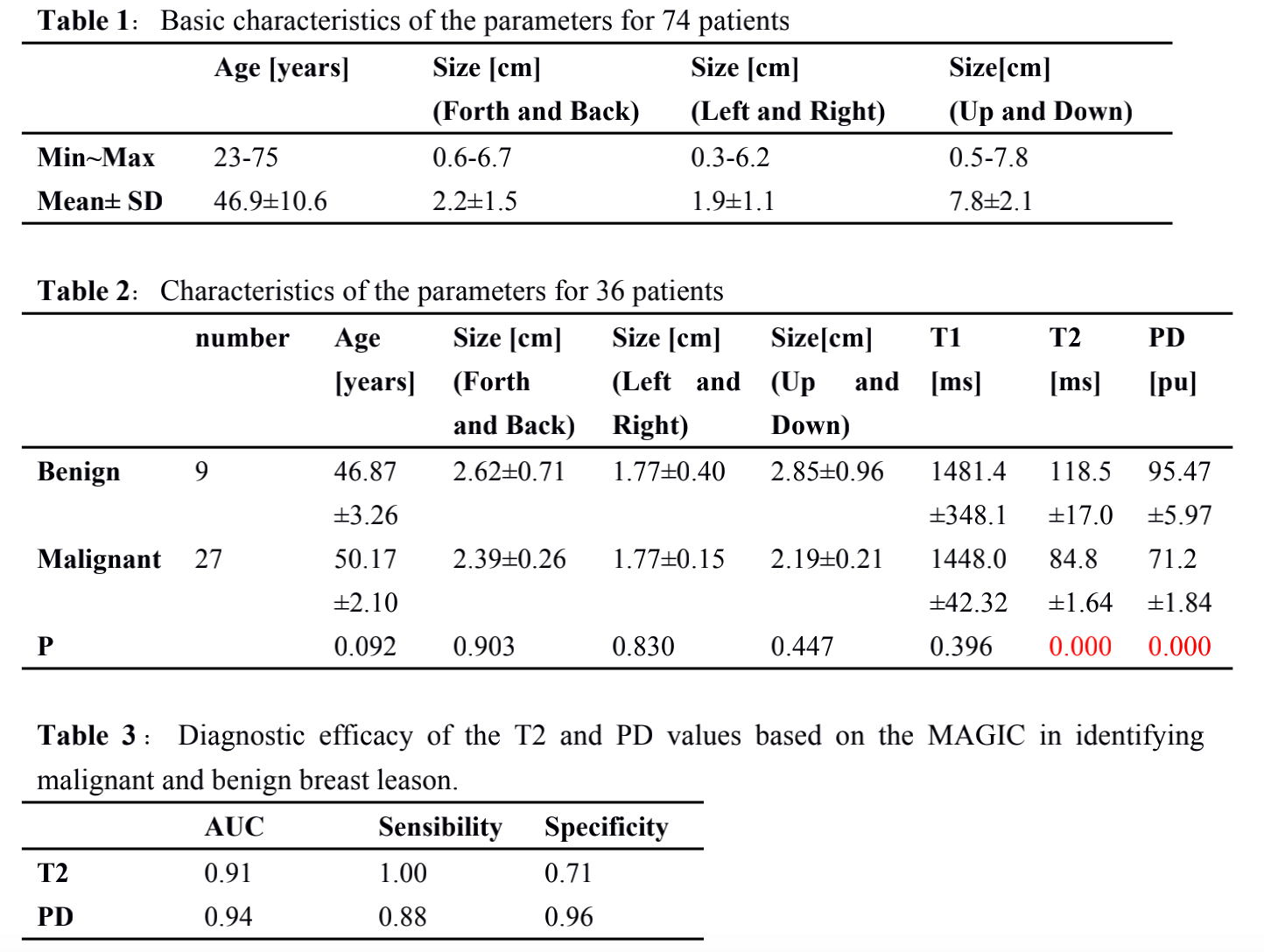
Table 1:Basic characteristics of the parameters for 74 patients
Table 2:Characteristics of the parameters for 36 patients
Table 3:Diagnostic efficacy of the T2 and PD values based on the MAGIC in identifying malignant and benign breast leason.
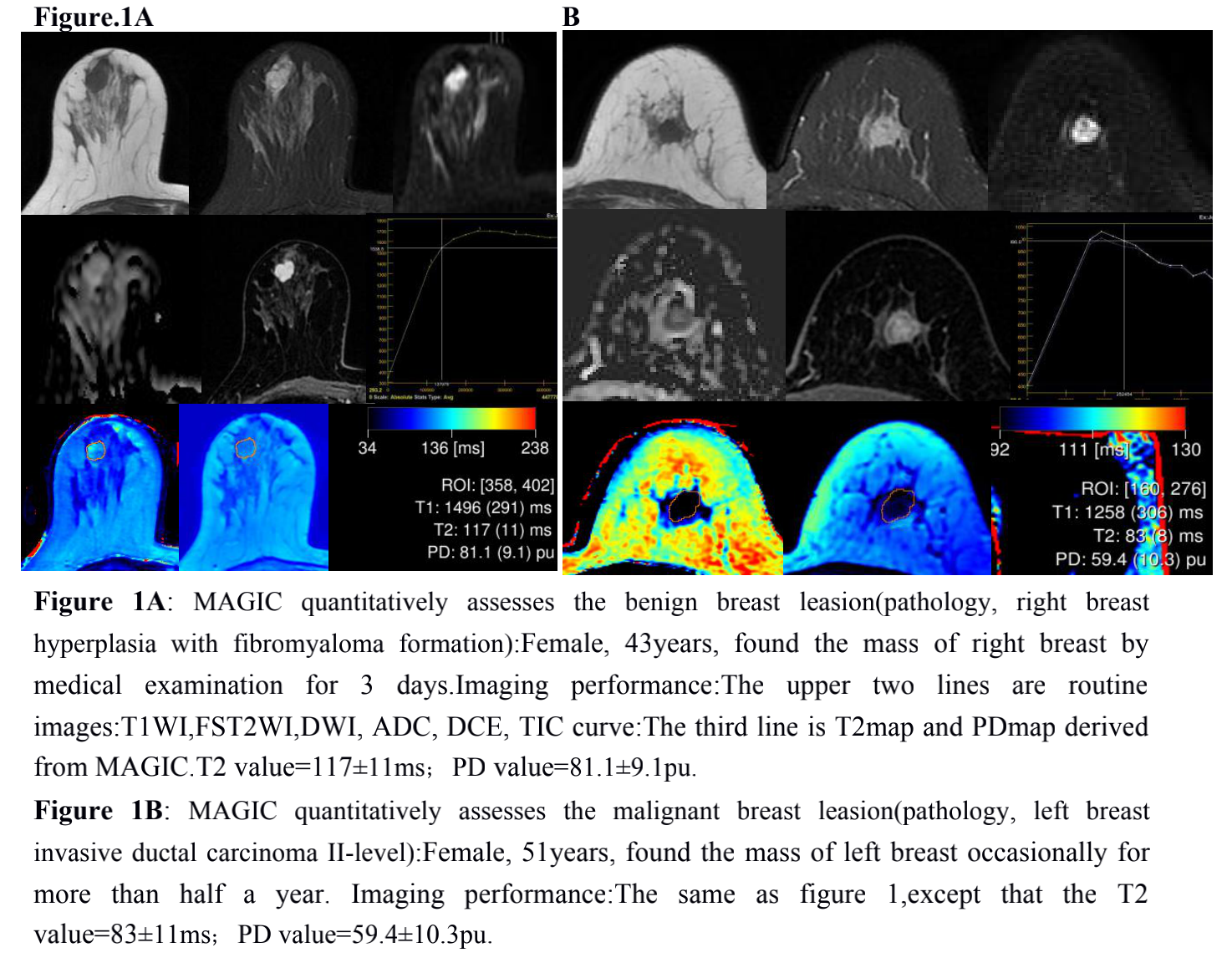
Figure 1A: MAGIC quantitatively assesses the benign breast leasion:T2 value=117±11ms;PD value=81.1±9.1pu.
Figure 1B: MAGIC quantitatively assesses the malignant breast leasion:T2 value=83±11ms;PD value=59.4±10.3pu.
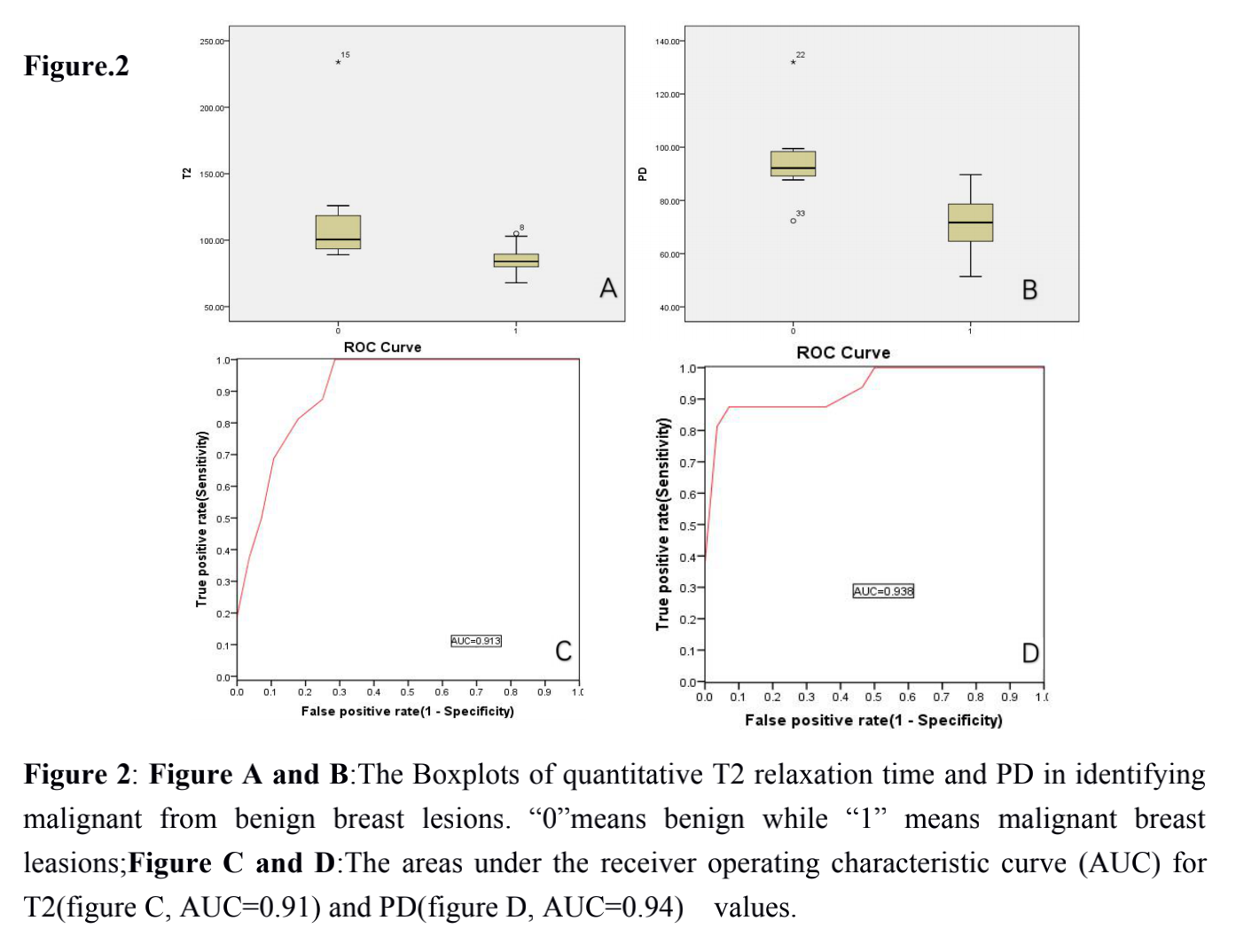
Figure 2:
Figure A and B:The Boxplots of quantitative T2 relaxation time and PD in identifying malignant from benign breast lesions. “0”means benign while “1” means malignant breast leasions;
Figure C and D:The areas under the receiver operating characteristic curve (AUC) for T2(figure C, AUC=0.91) and PD(figure D, AUC=0.94) values.