0535
3D Flow Compensated Interleaved EPI with Partial Fourier Acquisition: A Feasibility Study for Fast Intracranial TOF-MRA1Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China
Synopsis
As commonly used for intracranial vasculature, 3D TOF usually requires long acquisition time. In this study, we implemented a 3D-iEPI sequence with partial flow compensation, combined with partial Fourier acquisition to further reduce the flow artifacts. In specific, each interleave is sequentially acquired twice with alternating readout polarities to reduce the systematic inconsistencies between odd and even echoes. We explored the feasibility of such a sequence for fast intracranial TOF-MRA and demonstrated that the proposed sequence can reduce the acquisition time by approximately a factor of 2 with comparable vasculature depiction to 3D-GRE, which is promising for future applications.
INTRODUCTION
As widely used in non-contrast MR angiography (MRA) in clinical setting, the Time-of-flight (TOF) is conventionally implemented with the 2D or 3D-GRE sequence, in which the 3D-GRE is most commonly used for intracranial vasculature due to well depiction of arterial trees1. The background signal from stationary tissue is suppressed by rapid slab-selective RF excitation pulses, while the venous signal is suppressed using a saturation band on the venous side of the imaging volume. By reducing the number of RF pulses for a saturation band, segmented TOF has been proposed to increase the acquisition efficiency and alleviate the SAR problem with equivalent contrast and suppression effects in venous regions preserved as in the conventional methods2. Alternatively, the multi-echo acquisition such as EPI can achieve similar or even higher scan efficiency, as compared to the segmented TOF. However, flow artifacts are more complicated by EPI than GRE3, therefore, improvements in EPI based TOF-MRA sequence can be essential for reduction of flow artifacts. To our knowledge, there are no reports on TOF-MRA of intracranial vasculature with 3D-iEPI. Therefore, in this study, we implemented a first order gradient nulling (GMN) based partial flow compensation in 3D-iEPI4, combined with partial Fourier acquisition in phase direction, for reduction of the TE and flow artifacts5. We demonstrated the application of the proposed sequence on intracranial TOF-MRA, providing a substantial reduction in scan time compared to standard 3D-GRE, whilst maintaining well vasculature depiction.METHODS
In the proposed sequence (Fig.1), two shots of EPI acquisitions with partial coverage of k-space and alternating readout polarities were acquired sequentially to reduce phase oscillates in odd and even echoes and minimize the motion influence. Furthermore, compared with our previous flow compensation implementation4, the prephaser and partition encoding gradients were moved next to the readout for further reduction of flow artifacts. All measurements were performed on a commercial 1.5T scanner (MAGNETOM Aera, Siemens Healthcare GmbH, Erlangen, Germany) equipped with a 20-channel head/neck coil. Experimental data was obtained from a healthy volunteer using a standard 3D-GRE based TOF, a prototype flow compensated 3D-iEPI based TOF without and with alternating readout. The imaging parameters were shown in Table 1. Standard multiple overlapping thin slab acquisition (MOTSA)6 was used in both sequences. After data collection, all MRA images were displayed using a maximum intensity projection (MIP) algorithm.RESULTS
The preliminary in-vivo results show that, with flow compensation and partial Fourier acquisition, the 3D-iEPI sequence provides significant acquisition time reduction, as well as comparable vasculature depiction, compared to conventional TOF-MRA (Fig.2). Both 3D-GRE (Fig.2a) and 3D-iEPI (Fig.2b and Fig.2c) show comparable intracranial vasculature representation. In addition, no obvious flow artifacts were observed in 3D-iEPI with flow compensation and partial Fourier acquisition. That partial Fourier acquisition can not only alleviate the phase encode flow artifacts but also reduce the TE to be comparable with that in 3D-GRE, which can increase the vessel intensity7. Although the SNR loss in the magnitude images of 3D-iEPI sequence is inevitable, it has less effect on vessel signals and thus, the corresponding MIP images are similar to those from the 3D-GRE. It should be noticed that, both ghost artifacts and background suppression can be improved if alternating readout scheme applied (Fig. 2c), the latter one may be due to the reduced motion effect from the inherent short-term average in such alternating readout scheme. Moreover, some arteries were better resolved in TOF images by 3D-iEPI sequence, e.g. external carotid artery branch.DISCUSSION
In order to reduce the flow artifacts in 3D-iEPI, we implemented a partial flow compensation scheme to fully flow compensated the center echo in each shot, and utilized partial Fourier in phase encoding direction to further reduce the flow artifacts and minimize the TE. No obvious distortion and blurring artifacts were observed in the in-vivo experiments, which can be due to the short echo train used in the 3D-iEPI. By taking advantage of the highly efficient multi-echo acquisition, the proposed 3D-iEPI based TOF-MRA can provide a significant reduction in both SAR and san time, while maintaining similar vasculature representation compared to conventional 3D-GRE. However, the pulsatile or disordered flow can lead to ghosting or signal loss in the vessel due to B0 inhomogeneityl7, which can be more severe in EPI sequence. Less EPI factor in combination of partial Fourier acquisition can alleviate such artifacts but probably produce slightly more blurring and ringing. Evaluation of the diagnostic performance of 3D-iEPI TOF-MRA in patients would be needed in future study.CONCLUSION
We demonstrated that a flow compensated 3D-iEPI with partial Fourier acquisition allows approximate 2-fold reduction in acquisition time with comparable artery angiogram to 3D-GRE, which is promising for TOF-MRA applications.Acknowledgements
No acknowledgement found.References
1. Hartung MP, et al. Magnetic resonance angiography: current status and future directions. J Cardiovasc Magn Reson 2011; 13:19.
2. Zhang ZH, et al. Segmented TOF at 7T MRI: Techniques and clinical applications. Magn Reson Imaging 2015; 33:1042-1050.
3. Butts K, et al. Analysis of flow effects in echo-planar imaging. J. Magn. Reason Imaging 1992; 2:285-293.
4. Liu W, et al. 3D Flow Compensated Interleaved EPI for a Fast High-Resolution Susceptibility-Weighted Imaging at 1.5T. Proc. Intl. Soc. Mag. Reason. Med 2019; 27:3326.
5. Luk Pat GT, et al. Reducing flow artifacts in echo-planar imaging. Magn Reson Med 1997; 37: 436-447.
6. Parker DL, et al. MR angiography by multiple thin slab 3D acquisition. Magn Reson Med 1991; 17:434-451.
7. Drangova M, et al. Artifacts and signal loss due to flow in the presence of B0 inhomogeneity. Magn Reson Med 1996; 35:126-130.
Figures
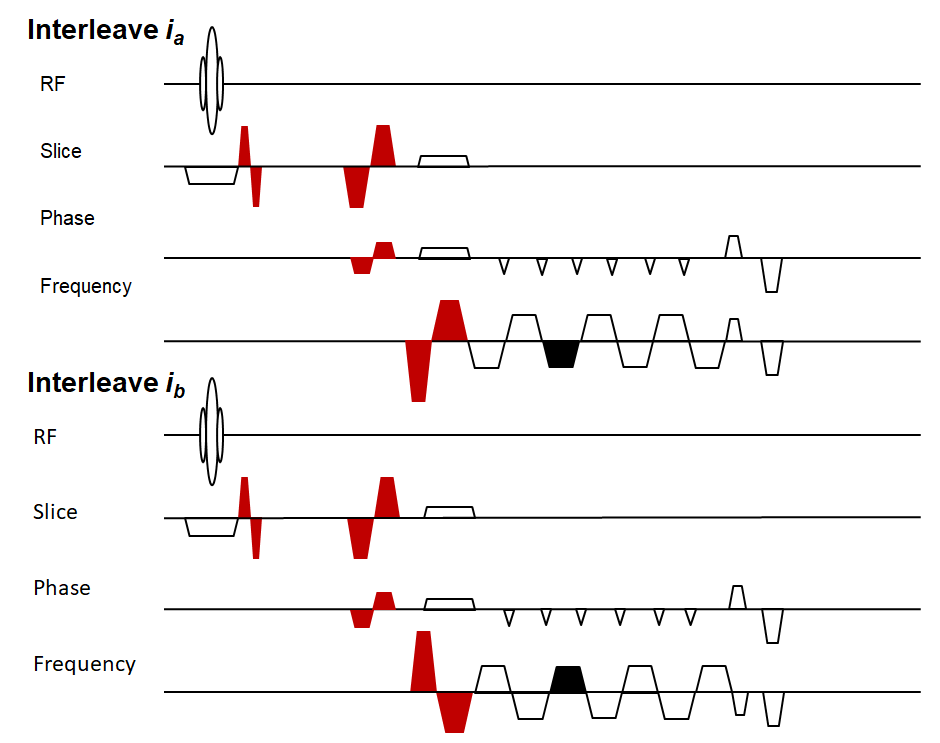

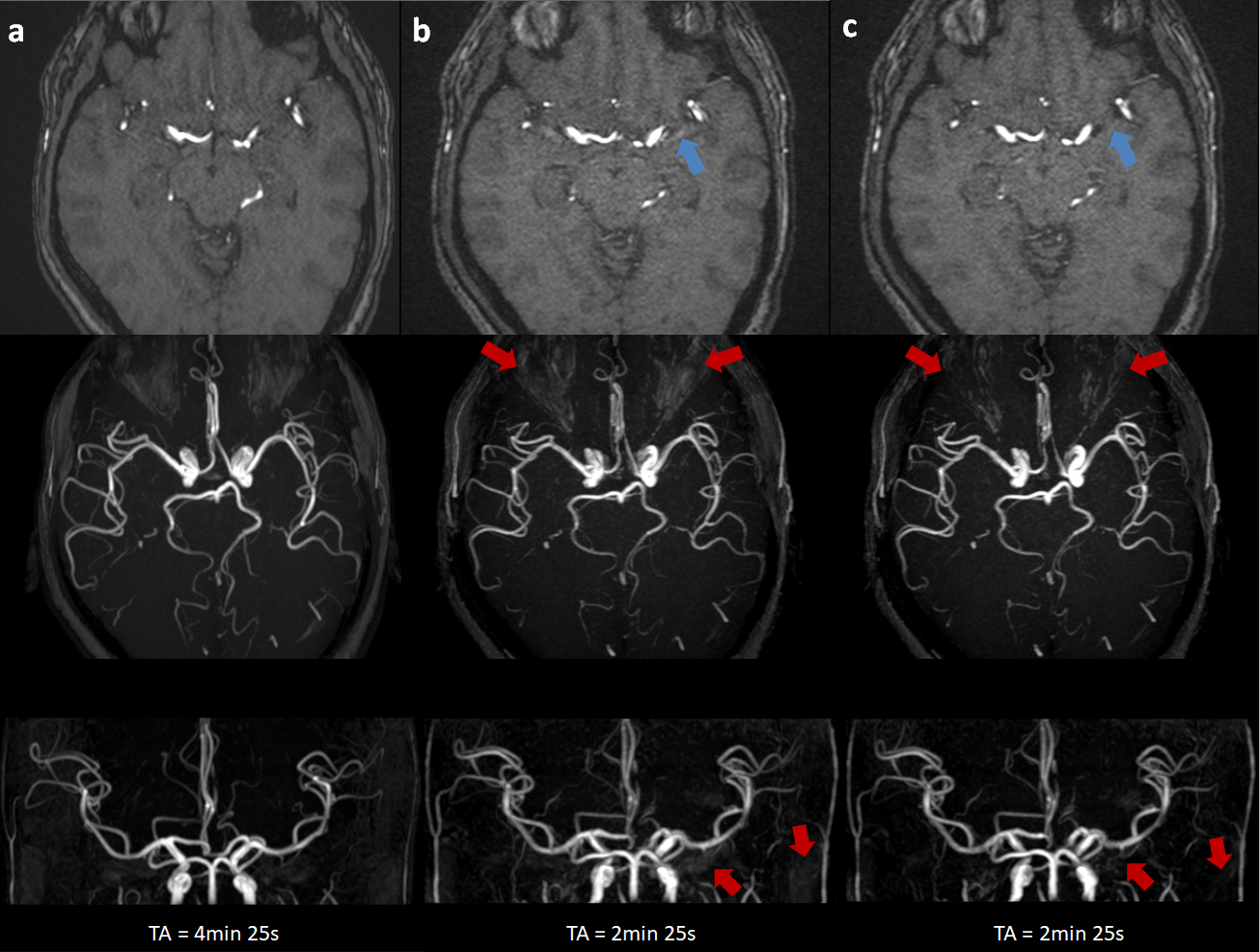
Figure. 2 Comparison of TOF images acquired with 3D-GRE and 3D-iEPI respectively. (a) Conventional 3D GRE based TOF magnitude image and corresponding MIPs. Acquisition time = 4min 25s; (b-c) 3D-iEPI based TOF magnitude image and corresponding MIPs, without and with alternating readout scheme respectively. Average = 2 and acquisition time = 2min 25s. Similar vasculature depiction are seen in the MIPs from both sequences. Slight ghost artifacts are shown in (b) and mitigated in (c), pointed by blue arrows. A better suppression of background tissues shown in (c), pointed by red arrows.