0522
Short-T2 MRI of Ancient Egyptian Mummified Human Tissue
Emily Louise Baadsvik1, Markus Weiger1, Romain Froidevaux1, Manuela Barbara Rösler1, David Otto Brunner1, Lena Öhrström2, Patrick Eppenberger2, Frank J. Rühli2, and Klaas Paul Pruessmann1
1Institute for Biomedical Engineering, ETH Zurich and University of Zurich, Zurich, Switzerland, 2Institute of Evolutionary Medicine, University of Zurich, Zurich, Switzerland
1Institute for Biomedical Engineering, ETH Zurich and University of Zurich, Zurich, Switzerland, 2Institute of Evolutionary Medicine, University of Zurich, Zurich, Switzerland
Synopsis
Evolutionary medicine aims to study disease development over long timescales, and through the study of mummified human remains, tissue information dating back thousands of years becomes accessible. Due to their status as ancient relics, nonintrusive techniques are preferable, and to date CT imaging is the most common modality. However, CT images lack soft-tissue contrast, making complementary MRI data desirable. Due to the extensively dehydrated nature and short T2 times of mummified tissues, acquiring such data is challenging. This research explored the use of the zero echo-time sequences and a high-performance gradient in mummy MRI, yielding yet unparalleled image quality.
Introduction
The field of evolutionary medicine aims to broaden our understanding of disease development by considering pathology from a long-term perspective. Through the study of mummified human tissue timeframes of several thousand years are unlocked, but due to their scarcity and historical value, great care must be taken when examining such samples. Medical imaging modalities are therefore natural contenders, and currently computed tomography (CT) is the most widespread technique. However, CT does not provide sufficient soft-tissue contrast, and so complementary MRI data is desired1-3. Acquiring such data is challenging, both due to the dehydrated nature of artificially mummified samples and the short T2 times associated with the remaining tissues (≤ a few hundred microseconds)4. Thus mummified tissues are practically invisible to standard MRI techniques, and specialised short-T2 approaches must be used.It has previously been shown that zero echo-time (ZTE)-based sequences5 together with a high-performance gradient insert6 enable high-resolution MR imaging of samples with short T2 values7. In this work, the ability of this system was investigated for improved depiction of mummified human tissues.
Methods
Three ancient Egyptian mummy samples (1500-1100 BC) were imaged, one head, one foot and one hand1,2. For the musculoskeletal samples a custom RF solenoid coil was constructed, with a PMMA tube length of 300 mm, a diameter of 120 mm and 7 copper windings spread over 250 mm of the tube, similar to1. A single-loop surface coil of 80 mm diameter was used for initial imaging of the hand sample. The head was imaged with a 1H-free 8-channel array coil8. All images were acquired with a 3T Philips Achieva scanner (Philips Healthcare, Best, the Netherlands), but using a custom RF system9 including symmetrically biased T/R switches10. Furthermore, a high-performance gradient insert providing a strength (G) up to 200 mT/m and a slew rate up to 1200 mT/m/ms at 100 % duty cycle was used6.ZTE imaging sequences use a radial centre-out pure frequency-encoding architecture, and their defining characteristic is that the readout gradient is prepared before spin excitation in order to achieve immediate full-speed k-space encoding. However, because the RF system has a finite dead-time Δ (includes half the RF pulse duration, T/R switching and the filter group delay) before signal acquisition can begin, there is data missing from central k-space5. From the various ways of dealing with this data gap, the hybrid filling (HYFI) technique11 was used. HYFI fills the very centre of k-space with single-point Cartesian acquisition and then divides the remainder of the gap into frequency-encoded radial shells, i.e. it is a hybrid between the PETRA12 and WASPI13 techniques. In this way, it increases SNR efficiency w.r.t. PETRA while largely maintaining image quality. See Fig. 1 for sequence details.
While immediate k-space encoding is vital for short-T2 imaging, to avoid resolution loss it is also necessary to complete each acquisition before significant signal decay14. In a frequency-encoding scheme, we therefore rely on a strong gradient to cover k-space swiftly. To investigate this effect on images of mummified tissue, the gradient insert was used with increasing gradient strengths from the conventional 31 mT/m up to the maximum of 200 mT/m.
Results
Fig. 2 shows HYFI images of the hand sample for different values of system dead-time (equivalent to TE) and gradient strength, using both the surface and solenoid coils. A CT image is also included for comparison. This sample was previously imaged with other short-T2 sequences1 at a resolution (Δr) of (0.9 mm)3, but these images exhibit severe blurring and image degradation. We see that while an increase in G up to around 100 mT/m significantly improves the image quality, as expected from7, increasing it further yields diminishing returns. Increasing the dead-time reduces the blurry image background, which is explained by attributing the background signal to T2 components too short to be encoded even with this protocol: The longer we delay acquisition, the more these components have decayed. The solenoid coil offers uniform sensitivity throughout the sample but requires longer scan times than the surface coil.Fig. 3 contains a more detailed look at the main images of the hand sample presented in Fig. 2. The top row focuses on different dead-time images, while the bottom row emphasises the different features that can be resolved. Fig. 4 has the same general layout as Fig. 3, but for the foot sample. Indicative sample constituents can be identified from the different dead-time images.
Fig. 5 illustrates the resolvable features in the head sample. CT data is included for comparison. While both CT and HYFI capture the same general tissues (bones, tendons, skin), the mummification substances in the skin (Fig. 2, brightest signal) are isointense w.r.t. surrounding tissues in CT, while in MRI they exhibit varying contrast.
Discussion and Conclusion
Our results further demonstrate the capabilities of the HYFI sequence and high-performance gradient in short-T2 MRI, and the acquired images have higher resolution and greater image quality than any existing work in the field. These images can be used to identify details of the mummification process and aid researchers with intricate knowledge of anatomy, tissue properties and pathology in studying the differences between these ancient samples and modern humans.Acknowledgements
No acknowledgement found.References
- Özen AC, Ludwig U, Öhrström LM, Rühli FJ, Bock M. Comparison of ultrashort echo time sequences for MRI of an ancient mummified human hand. Magnetic Resonance in Medicine. 2016;75(2):701-708
- Öhrström LM, von Waldburg H, Speier P, Bock M, Suri RE, Rühli FJ. Scenes from the past: MR imaging versus CT of ancient Peruvian and Egyptian mummified tissues. RadioGraphics. 2013;33(1):291-296
- Giovannetti G, Guerrini A, Carnieri E, Salvadori PA. Magnetic resonance imaging for the study of mummies. Magnetic Resonance Imaging. 2016;34(6):785-794
- Posh JC. Technical limitations on the use of traditional magnetic resonance imaging in the evaluation of mummified remains: A view from a hands-on radiologic technologist’s perspective. Anatomical Record. 2015;298(6):1116-1124.
- Weiger M, Pruessmann KP. MRI with zero echo time. Encyclopedia of Magnetic Resonance (John Wiley and Sons, Ltd, 2012)
- Weiger M, Overweg J, Rösler MB, Froidevaux R, Hennel F, Wilm BJ, Penn A, Sturzenegger U, Schuth W, Mathlener M, Borgo M, Börnert P, Leussler C, Luechinger R, Dietrich BE, Reber J, Brunner DO, Schmid T, Vionnet L, Pruessmann KP. A high-performance gradient insert for rapid and short-T2 imaging at full duty cycle. Magnetic Resonance in Medicine. 2018;79(6):3256-3266
- Froidevaux R, Weiger M, Rösler MB, Brunner DO, Wilm B, Dietrich B, Reber J, Pruessmann KP. Pushing the limits of short-T2 MRI: 200 mT/m gradient strength and 2 MHz bandwidth. Proceedings of the 26th Annual Scientific Meeting of ISMRM (Paris, France, 2018)
- Rösler MB, Leussler C, Brunner DO, Schmid T, Weiger M, Hennel F, Luechinger RC, Pruessmann KP. A head transmit-receive array for a high performance gradient insert. Proceedings of the 27th Annual Meeting of ISMRM (Montreal, Canada, 2019)
- Dietrich BE, Brunner DO, Wilm BJ, Barmet C, Gross S, Kasper L, Haeberlin M, Schmid T, Vannesjo SJ, Pruessmann KP. A field camera for MR sequence monitoring and system analysis. Magnetic Resonance in Medicine. 2016;75:1831-1840
- Brunner DO, Furrer L, Weiger M, Baumberger W, Schmid T, Reber J, Dietrich BE, Wilm BJ, Froidevaux R, Pruessmann KP. Symmetrically biased T/R switches for NMR and MRI with microsecond dead time. Journal of Magnetic Resonance. 2016;263:147-155
- Froidevaux R, Weiger M, Rösler MB, Brunner DO, Pruessmann KP. HYFI: Hybrid filling of the dead-time gap for faster zero echo time imaging. Proceedings of the 27th Annual Meeting of ISMRM (Montreal, Canada, 2019)
- Grodzki DM, Jakob PM, Heismann B. Ultrashort echo time imaging using pointwise encoding time reduction with radial acquisition (PETRA). Magnetic Resonance in Medicine. 2012;67(2):510-518
- Wu Y, Dai G, Ackerman JL, Hrovat MI, Glimcher MJ, Snyder BD, Nazarian A, Chesler D. Water- and fat-suppressed proton projection MRI (WASPI) of rat femur bone. Magnetic Resonance in Medicine. 2007;57(3):554-567
- Weiger M, Pruessmann KP. Short-T2 MRI: Principles and recent advances. Progress in Nuclear Magnetic Resonance Spectroscopy. 2019
Figures
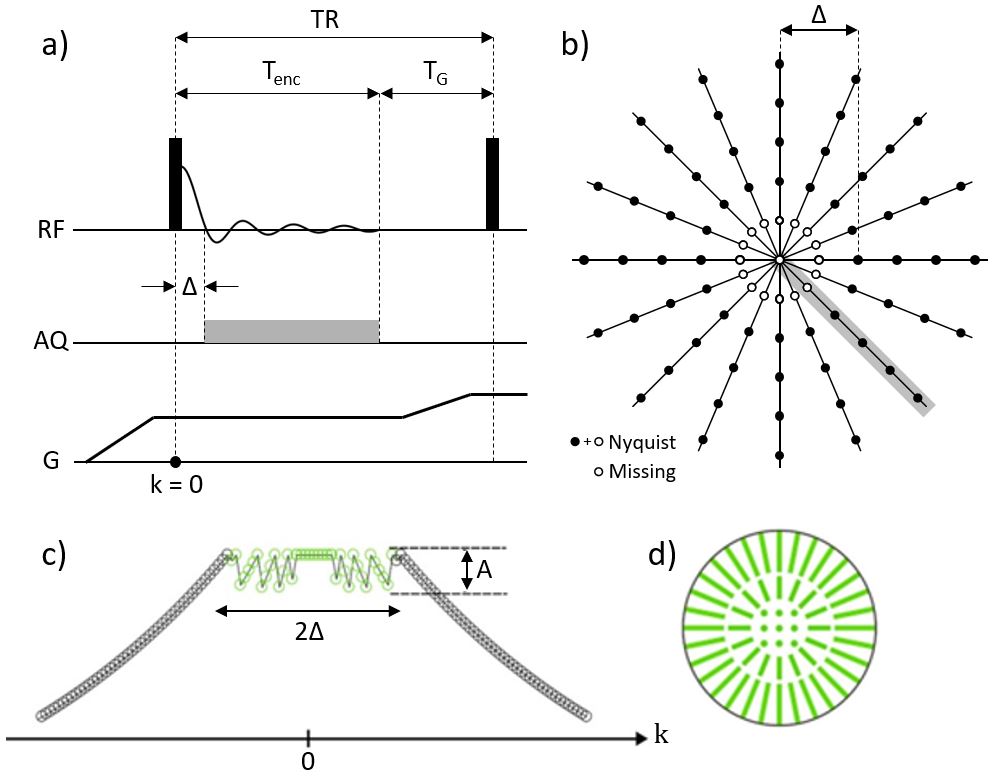
Fig.
1: a) ZTE sequence diagram, showing the dead time (Δ)
between signal creation and acquisition (AQ), gradient encoding of duration Tenc
and the time TG used for spoiling and preparing the gradient for the
next TR. b) ZTE k-space acquisition geometry. The grey line marks the
acquisition within one TR. c) HYFI decay behaviour. The maximum T2* decay
allowed in the data gap is determined by the parameter A. d) HYFI acquisition
geometry in the data gap: A mix of Cartesian single-point and radial acquisitions.
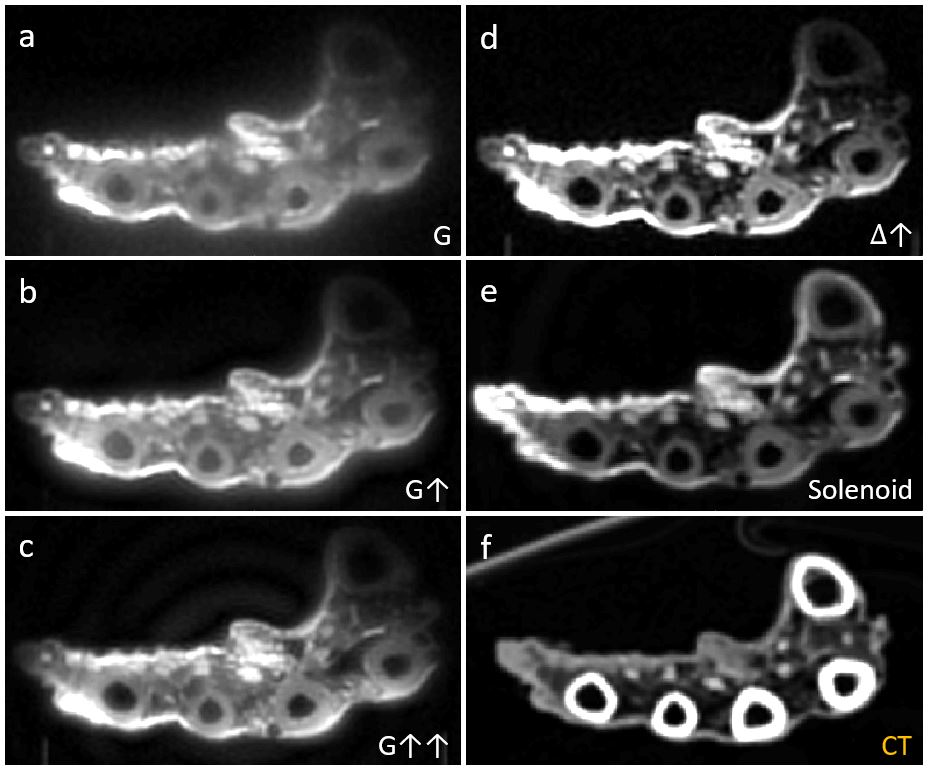
Fig.
2: ZTE images of the hand sample, comparing gradient strengths, dead-times (Δ)
and RF coils. a) G = 31 mT/m, Δ = 12 us, scan time = 10 mins, b) G = 98 mT/m, Δ
= 10 us, scan time = 32 mins, c) G = 196 mT/m, Δ = 10 us, scan time = 1 hr 5
mins, d) G = 98 mT/m, Δ = 30 us, scan time = 35 mins, e) G = 98 mT/m, Δ
= 30 us, scan time = 1 hr 44 mins, f) CT image. All MRI images were acquired
with the surface coil except e, which was acquired with the solenoid coil. Δr
= (0.6 mm)3, TR = 1 ms.
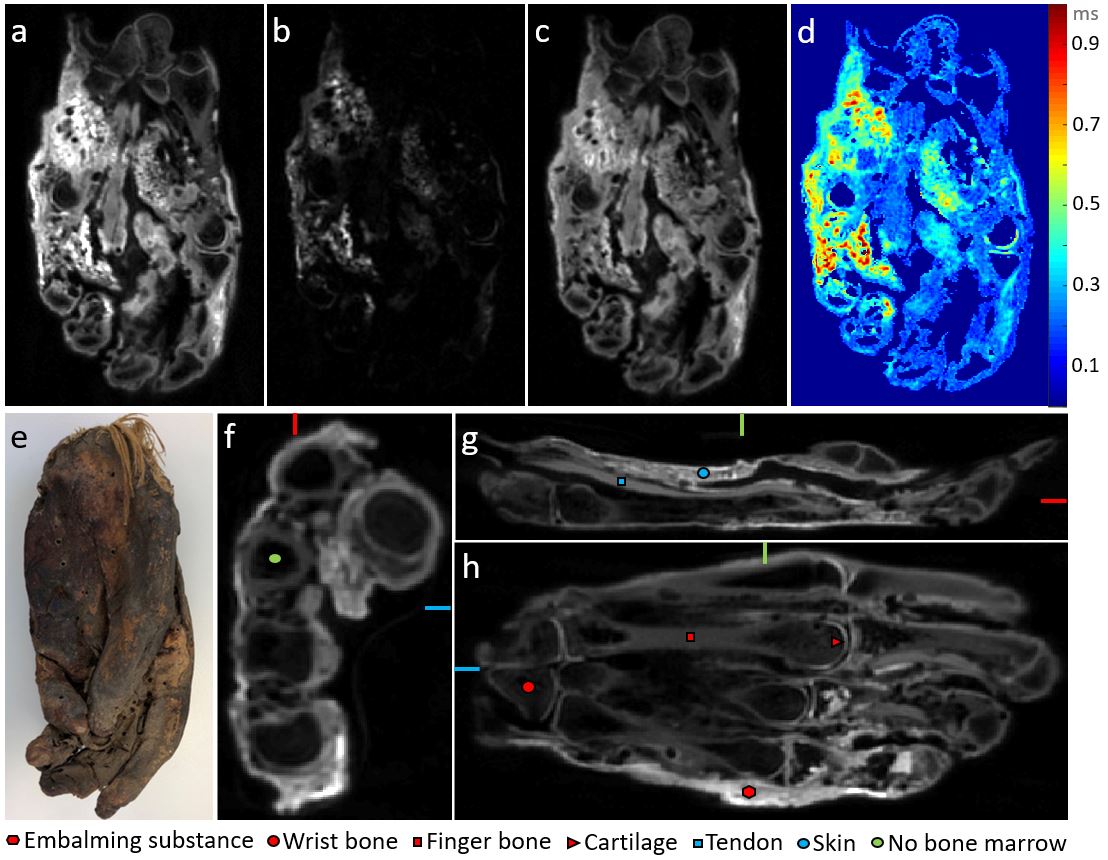
Fig.
3: Solenoid coil images of the hand sample. a) Same data set as in Fig. 2e, b) Δ
= TE = 612 us, G = 31 mT/m, scan time = 2 hrs 12 mins, c) subtraction image:
shortΔ - longΔ → longer-T2 tissues suppressed, d) T2* map. e) Sample photo, f-h)
perpendicular slices from the short-Δ data set in a) showing
interesting features. Slice location is indicated by coloured lines: The slice
with red markers is located at the position of the red lines in the other
slices etc. Δr = (0.6 mm)3, TR = 1 ms.
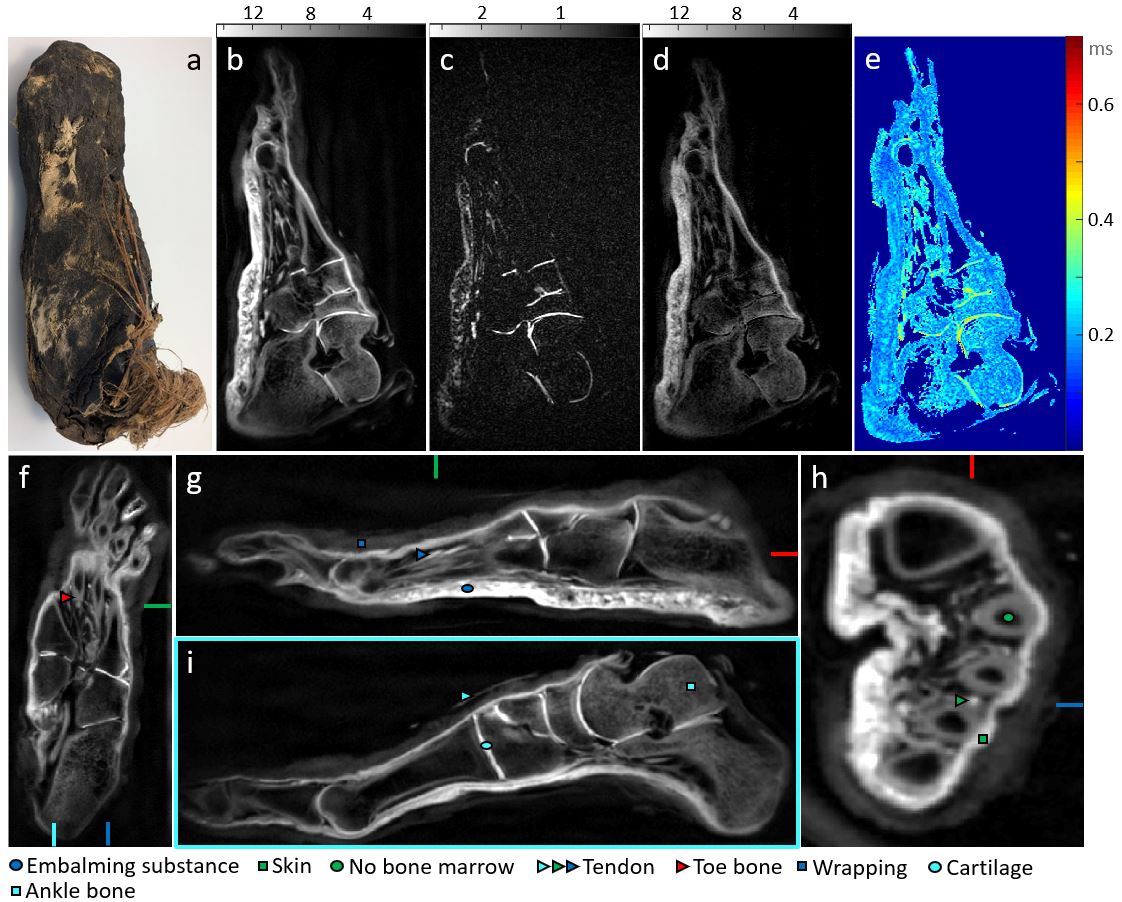
Fig.
4: Solenoid coil images of the foot sample. a) Sample photo, b) Δ
= 30 us, G = 98 mT/m, c) Δ = TE = 611 us, G = 31 mT/m, d) subtraction image:
shortΔ – 4*longΔ→ longer-T2 tissues suppressed, e) T2* map. f-h) Perpendicular slices
from the short-Δ data set in b) showing interesting features (same location marking
scheme as in Fig. 3), i) additional slice. Δr = (0.6 mm)3, TR =
1 ms, scan time = 1 hr 28 mins/1hr 33 mins for short/long Δ
respectively. Greyscale colour bars give relative image intensities.
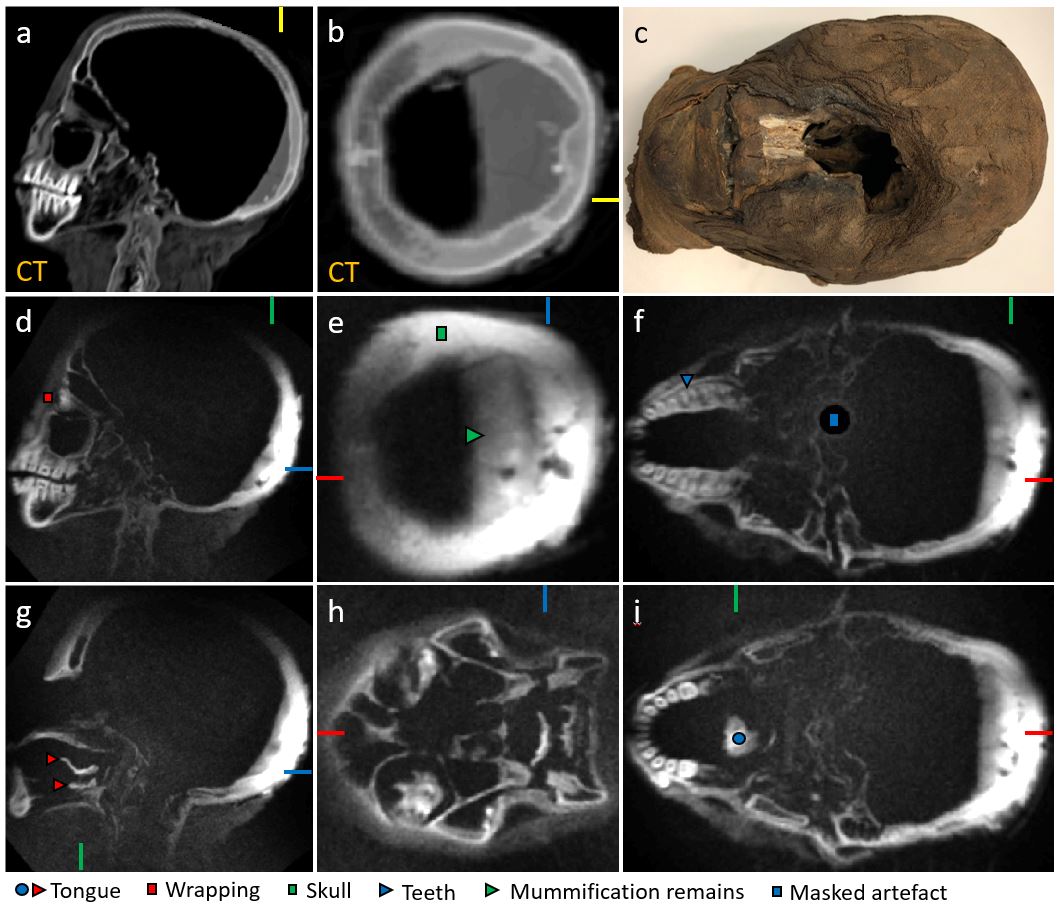
Fig.
5: Array coil images of the mummy head, intensity corrected to compensate for
coil sensitivity loss. a,b) CT images (same slices as d,e respectively): a is
an orthogonal slice at the position of the yellow line in b and vice versa, c)
sample photo. d-f and g-i) Orthogonal slices with interesting features marked.
The slice without a red line is located at the position of the red line in the
other slices in that row and so on. Δr = (1.0 mm)3, TR =
0.4 ms, scan time = 2 hrs 27 mins, Δ = 35 us, G = 89 mT/m.