0455
Pilot tone–based respiratory motion correction for 2D myocardial T1 mapping1Physikalisch-Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany, 2Siemens Healthcare, Erlangen, Germany, 3Division of Imaging Sciences and Biomedical Engineering, King's College London, London, Germany, 4Biomedical Engineering and Einstein Center Digital Future, Technische Universität Berlin, Berlin, Germany
Synopsis
Respiratory heart motion during T1 data acquisition can lead to strong motion artefacts, compromising the quality of reconstructed T1 maps. Commonly, breathhold techniques are used to minimize respiratory motion but they suffer from low scan efficiency and require patient cooperation. Here, we propose a Pilot tone-based respiratory motion correction approach for free-breathing myocardial T1 mapping. First, through-plane motion is corrected for by performing prospective slice tracking online during data acquisition. Second, in-plane motion is corrected for retrospectively by applying a phase shift to k-space data before image reconstruction. The feasibility of the proposed approach was demonstrated in four healthy volunteers.
Introduction
Myocardial T1 mapping is a promising technique to detect fibrosis and diffuse cardiomyopathies1-2. Commonly, multiple 2D slices are acquired for this purpose, each in a different breathhold. The repeated breathholding can be challenging especially for cardiac patients, and the maximum possible breathhold duration limits the achievable image resolution. Although T1 mapping during free-breathing has been demonstrated, these methods rely on the retrospective separation of respiratory motion and contrast dynamics3. This requires a complex image reconstruction scheme and might be challenging for strong through-plane motion.We propose a method that prospectively corrects for respiratory motion using a quantitative respiratory surrogate signal (pilot tone, PT) to adapt the slice position in real-time and track the motion of the heart during breathing. This ensures that data at different inversion times is acquired at the same position in the heart during the entire respiratory cycle. In addition to this prospective through-plane motion correction, in-plane motion correction is carried out during image reconstruction also based on the quantitative PT signal. The feasibility of our motion correction approach was demonstrated on four healthy volunteers.
Methods
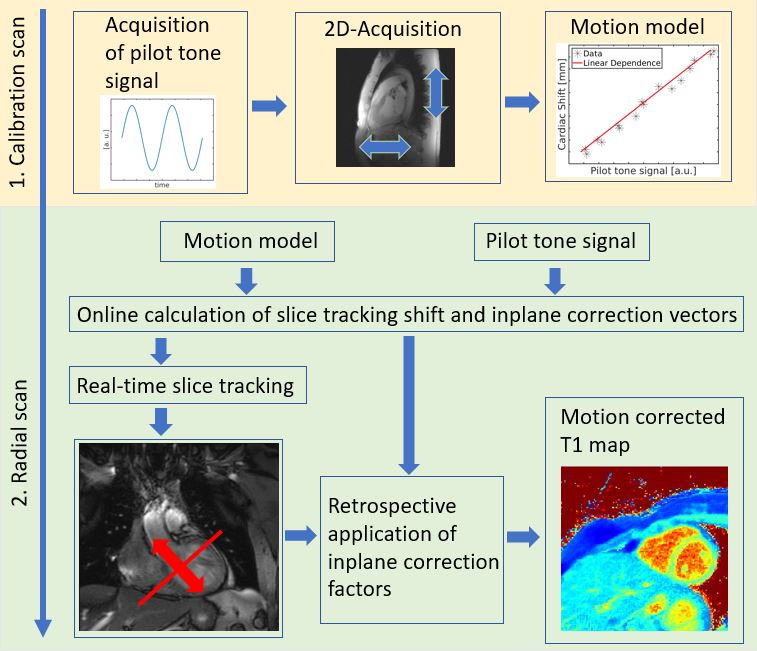
All measurements were performed with inhouse-built sequences on a 3T scanner (MAGNETOM Verio, Siemens Healthcare, Erlangen, Germany) on four healthy volunteers (2 female, 2 male, age 34±28 years) after approval of the local ethics board was obtained. Similar to previous applications for respiratory gating and cardiac triggering4-5, an additional PT signal was generated using a commercial RF-synthesizer (Hewlett Packard) connected to an inhouse-built non-resonant coil, which was placed close to the bore of the scanner. An overview of the calibration and motion correction method is given in Figure 1.In a first step, a calibration scan is used to estimate a motion model which transforms the qualitative PT signal into a quantitative motion surrogate describing the respiratory movement of the heart in mm. After calibration, the PT signal can then be used for respiratory motion correction of the diagnostic T1 mapping scan.
For calibration, 2D ECG-triggered data was acquired over 60 cardiac cycles in sagittal view with FOV = (320×320)mm2, voxel size = (1.7×1.7×8)mm3, TE/TR = 3.22/5.7ms and FA = 5°. An online image registration was performed to calculate the heart displacement along head-feet and anterior-posterior directions. This was used to calibrate the simultaneously acquired PT signal to the estimated motion. After the calibration, a quantitative surrogate for respiratory motion exists, providing –in real time– two types of corrections: a through-plane and an in-plane shift vector.
Correspondingly, the motion correction approach then consists of two steps. First, online prospective PT slice tracking was applied to compensate for through-plane motion of the heart during acquisition, i.e. the location of the excited slice was adapted for each TR6. Second, a phase shift was retrospectively applied to k-space data during reconstruction to account for in-plane motion.
T1 mapping data was acquired continuously during 15s in short-axis view using a 2D golden-angle-radial trajectory leading to 3080 radial lines with the same scan parameters as for the calibration scan, but with additional inversion pulses applied every 2.1s independent of the heart rate7-8. Diastolic images at different inversion times were reconstructed with an iterative non-cartesian SENSE reconstruction scheme. A three-parameter fit (M0, T1, flip angle) was used to obtain T1 maps.
To evaluate the performance of the proposed method, T1 mapping was performed with and without motion correction during free-breathing and during breathhold for reference.
Results and Discussion
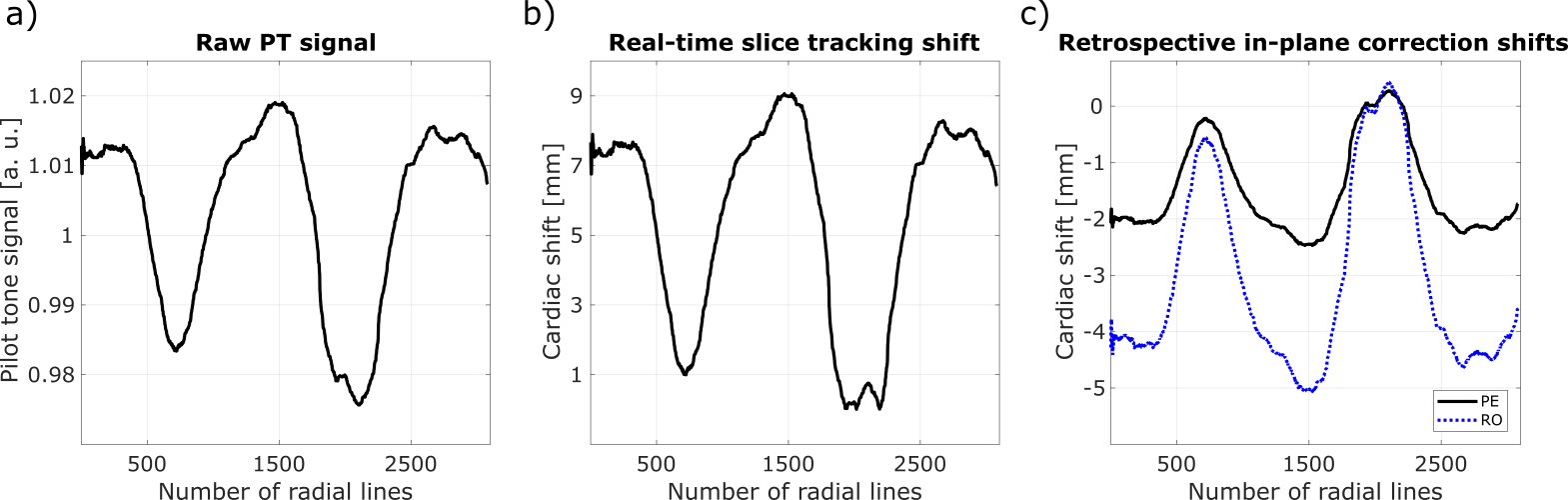
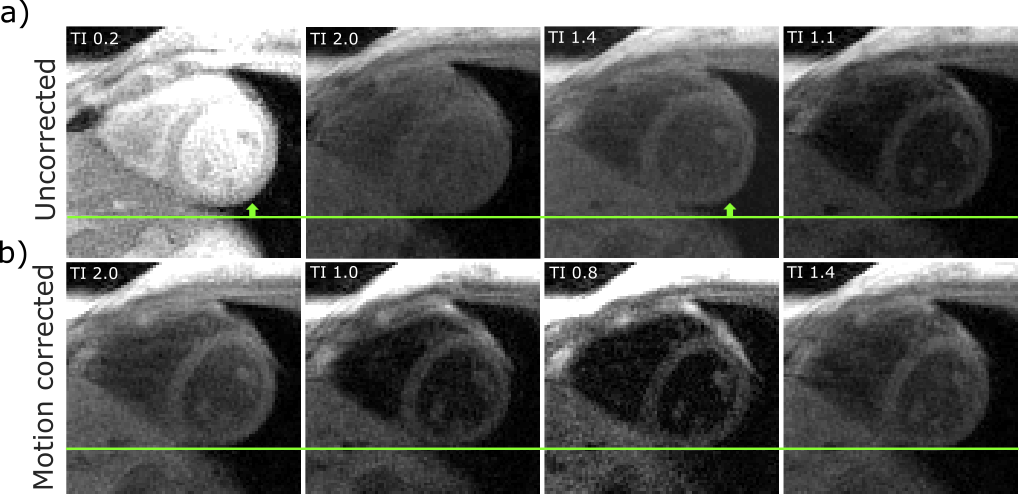
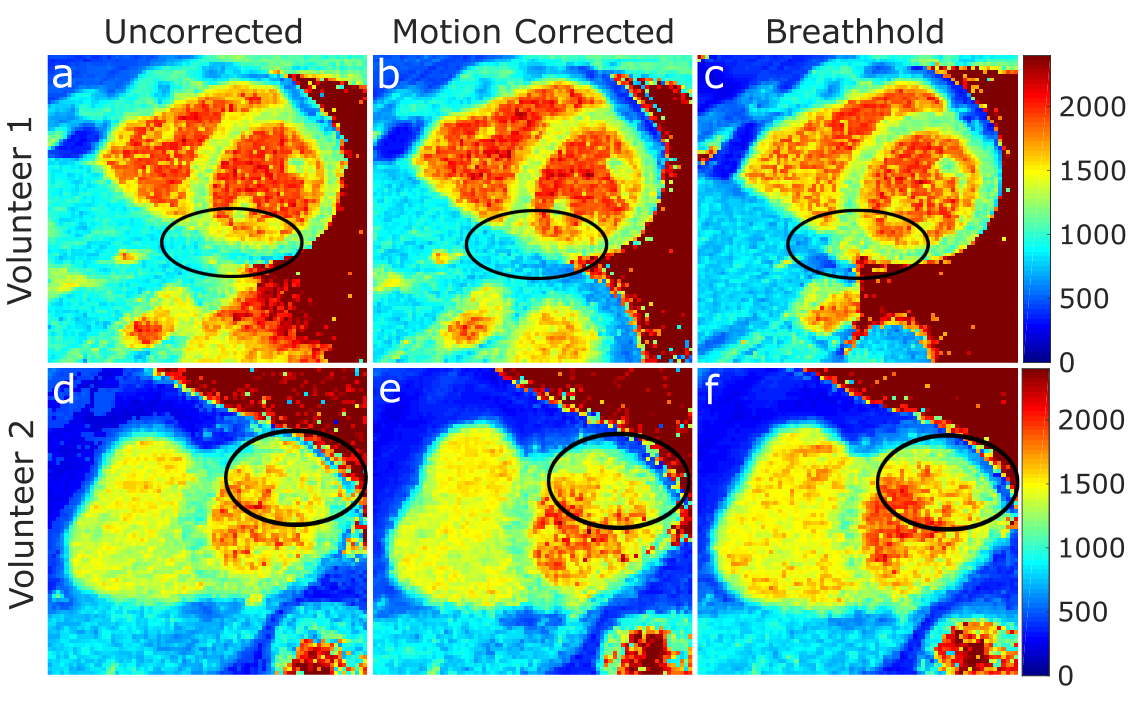
Figure 2 shows the raw PT signal and the quantitative motion displacement derived from the PT signal and the motion model. Cardiac shifts of up to 10mm for through-plane and 5mm in-plane were found. For visualization, images of different respiratory states were reconstructed showing the heart motion during radial acquisition of 15s with and without motion correction [Fig. 3]. Figure 4 shows T1 maps of two healthy volunteers during free-breathing and breathhold. Respiratory motion leads to higher variations of the T1 estimates in the myocardium [Fig. 4 a, d)] compared to the motion corrected scans [Fig. 4 b, e)]. After motion correction, breathing artefacts were strongly reduced and the visibility of the myocardium and fat structures was improved. Difficulties in performing a breathhold resulted in blurring around the myocardium for one volunteer [Fig. 4 f)].Conclusion
Here, we present a correction approach to compensate for respiratory heart motion in myocardial T1 mapping during free-breathing. A PT signal was correlated to respiratory motion of the heart, and slice tracking could then be performed during T1 measurements. Additional in-plane motion was compensated for retrospectively during image reconstruction. We demonstrated that our proposed method results in improved image quality of myocardial T1 maps.Acknowledgements
No acknowledgement found.References
[1] Schelbert EB, et al.,2016. State of the art: clinical applications of cardiac T1 mapping. Radiology. 2016; 278: 658– 676.
[2] Von Knobelsdorff‐Brenkenhoff F, et al., 2012. Cardiovascular magnetic resonance imaging in ischemic heart disease. J Magn Reson Imaging. 2012; 36:20–38.
[3] Shaw JL, et al., 2018. Free‐breathing, non‐ECG, continuous myocardial T1 mapping with cardiovascular magnetic resonance multitasking. Magn Reson Med, 2019; 81(4):2450-2463.
[4] Speier S, et al., 2015. PT-Nav: A Novel Respiratory Navigation Method for Continuous Acquisition Based on Modulation of a Pilot Tone in the MR-Receiver. ESMRMB 129:97-98, 2015. DOI: 10.1007/s10334-015-0487-2.
[5] Bacher M, et al., 2018. Model-Based Lag Free Processing of Pilot Tone Navigator Data Enables Prospective Cardiac Triggering. Proc. ISMRM 2018, #2960.
[6] Ludwig J, et al., 2019. Pilot tone-based prospective respiratory motion correction for 2D cine cardiac MRI. Proc. ISMRM 2019 #0073.
[7] Becker KM, et al., 2018. Simultaneous high-resolution cardiac T1 mapping and cine imaging using model-based iterative image reconstruction. Magn Reson Med, 2019; 81(2):1080-1091.
[8] Becker KM, et al., 2019. Fast myocardial T1 mapping using cardiac motion correction. Magn Reson Med, 2020; 83(2):438-451.
Figures