0335
Motion-Robust, Free-Breathing, High-SNR Liver Fat Quantification Using a Variable Flip Angle Approach and Motion-Corrected Averaging1Department of Radiology, University of Wisconsin, Madison, Madison, WI, United States, 2Department of Medical Physics, University of Wisconsin, Madison, Madison, WI, United States, 3Department of Pediatrics, University of Wisconsin, Madison, Madison, WI, United States, 4Department of Biomedical Engineering, University of Wisconsin, Madison, Madison, WI, United States, 5Department of Medicine, University of Wisconsin, Madison, Madison, WI, United States, 6Department of Emergency Medicine, University of Wisconsin, Madison, Madison, WI, United States
Synopsis
Chemical shift-encoded (CSE)-MRI enables accurate and precise quantification of proton density fat-fraction (PDFF) in the liver. Widely used 3D multi-echo spoiled gradient echo (SGRE) CSE-MRI requires reliable breath-holding to avoid motion-related artifacts. This is a major limitation for children, the elderly, and sick patients. Free-breathing 2D sequential CSE-MRI is motion-robust, however, suffers from low signal-to-noise-ratio (SNR). To overcome these limitations, we combined variable flip angle (VFA) 2D acquisitions and nonlocal means (NLM) motion-corrected averaging. In this prospective study, free-breathing multi-repetition VFA-NLM demonstrated high SNR and reduced artifacts compared to the conventional 3D-SGRE, while preserving accuracy of PDFF quantification.
INTRODUCTION
Chemical shift encoded (CSE)-MRI methods enable mapping of proton density fat-fraction (PDFF), a biomarker of triglyceride concentration1 with applications in the assessment of non-alcoholic fatty liver disease (NAFLD)1. Current CSE-MRI methods are typically based on 3D multi-echo spoiled gradient echo (SGRE) acquisitions2. Unfortunately, reliable breath-holding is necessary to avoid motion-related artifacts. This is problematic in children and many patients, where breath-holding may be limited or not possible. 2D sequential CSE-MRI is inherently motion-robust due to its very short temporal footprint and can be reliably acquired during free-breathing3. However, the use of low flip angles with linear phase encoding to avoid T1-related bias, leads to low signal-to-noise-ratio (SNR) with 2D sequential techniques. A recently introduced centric encoding variable flip angle (VFA) acquisition approach improves SNR, avoiding T1 bias through a novel variable flip angle schedule4. In order to further improve SNR, several repetitions may be acquired during free-breathing and averaged. However, this averaging will result in blurring and bias due to the presence of motion between repetitions. Recently, nonlocal means (NLM) methods have been shown to enable motion-corrected averaging of multi-repetition 2D CSE acquisitions, enabling additional SNR gains while minimizing blurring5. However, it is unknown whether NLM can be synergistically combined with VFA-based 2D CSE-MRI. Thus, the purpose of this work is to demonstrate the feasibility of a VFA CSE-MRI strategy, combined with NLM-based motion corrected averaging to obtain free-breathing, high-quality, high SNR liver PDFF quantification in children and adults.METHODS
Technique: This study evaluated a combination of VFA and NLM techniques. A novel 2D sequential CSE-MRI technique with centric encoding and VFA was recently developed and validated4, which provides optimized SNR, low T1 bias, and low blurring in liver fat quantification. NLM-based motion-corrected averaging was applied across multiple repetitions of the acquired multi-echo complex CSE-MRI data. This process was performed jointly for all acquired echo times. The algorithm was designed to find the most similar pixel in each of the different slices and repetitions based on a neighborhood similarity metric and perform weighted averaging across repetitions based on this metric.Subjects: 15 subjects (mean age 23 years, age range 11-48 years; mean BMI 27.1, range 17.3-35.3) were imaged on a clinical 3T MRI system (MR750, GE Healthcare Waukesha, WI) using a 32-channel phased-array torso coil. In this prospective, IRB approved study all participants provided informed assent and parents provided written informed consent.
MRI Acquisition: Multi-echo 3D and 2D CSE-MRI data were acquired to obtain PDFF maps. Three subsets of a single 2D acquisition with 10 repetitions were explored, VFA with a single repetition (VFA), VFA-NLM with 5 repetitions (VFA-NLM 5 REP) and VFA-NLM with all 10 repetitions (VFA-NLM 10 REP). Detailed acquisition parameters are listed in Table 1.
Reconstruction and Statistical Analysis: Source CSE-MRI data with multiple repetitions were processed using an NLM-based motion corrected averaging algorithm. The resulting echo images were subsequently processed using a confounder-corrected PDFF mapping algorithm6. All reconstruction and processing was implemented using MATLAB (MathWorks, Natick, MA). A region of interest (ROI) was placed in each of the nine liver Couinaud segments to measure mean and standard deviation of PDFF using OsiriX (OsiriX Lite). For each subject, ROI measurements were averaged across all segments to obtain an overall measure of liver PDFF, and a measure of standard deviation. Linear regression and Bland-Altman analysis were performed to compare PDFF from different techniques (VFA, VFA-NLM 5 REP, VFA-NLM 10 REP) to the reference (3D CSE-MRI). Further, in order to assess SNR performance, PDFF standard deviation distribution was plotted across different techniques and two-sided Student’s t-test was performed to compare each technique with the reference technique. All statistical analysis was performed using Python.
RESULTS
As shown in Figure 1, free-breathing VFA, VFA-NLM-5 REP and VFA-NLM-10 REP showed similar liver PDFF measurements, with high correlation and narrow limits of agreement compared to the 3D CSE-MRI reference. VFA showed similar SNR to 3D CSE-MRI (p=0.88). Importantly, VFA-NLM was observed to improve SNR with increasing number of repetitions (p<0.05 for VFA-NLM 5 REP, p<0.01 VFA-NLM 5 REP) in comparison to 3D CSE-MRI (Figure 2 and 3). In addition to the excellent noise reduction, the proposed VFA-NLM approach avoided motion artifacts and preserved image sharpness at tissue and vessel boundaries. Using VFA-NLM 10 REP, a striking reduction of motion-related artifacts was observed (Figure 3 and 4) in comparison to 3D CSE-MRI. Additionally, VFA-NLM 10 REP demonstrated improved visibility of organ boundaries, intrahepatic vessels (Figure 4).DISCUSSION AND CONCLUSION
This study reports on a novel free-breathing PDFF mapping strategy evaluated in 15 subjects. The combination of multi-repetition VFA with NLM-based motion-corrected averaging enabled free-breathing fat quantification that is accurate, has high SNR performance and minimal artifacts, overcoming the limitations of standard breath-held CSE-MRI methods. VFA-NLM is a promising method for fat quantification especially in children and may have broad applications in patients who are incapable of sustaining a prolonged breath-hold.Acknowledgements
The authors wish to acknowledge support from the NIH (UL1TR00427, R01-DK117354, R01-DK083380, R01-DK088925, R01-DK100651, K24-DK102595). Further, we wish to acknowledge GE Healthcare and Bracco Diagnostics, who provides research support to the University of Wisconsin. Finally, Dr. Reeder is a Romnes Faculty Fellow, and has received an award provided by the University of Wisconsin-Madison Office of the Vice Chancellor for Research and Graduate Education with funding from the Wisconsin Alumni Research Foundation.References
1. Caussy C, Reeder SB, Sirlin CB, Loomba R. Noninvasive, Quantitative Assessment of Liver Fat by MRI-PDFF as an Endpoint in NASH Trials. Hepatology. Wiley-Blackwell; 2018 Aug;68(2):763–72.
2. Yokoo T, Bydder M, Hamilton G, Middleton MS, Gamst AC, Wolfson T, et al. Nonalcoholic fatty liver disease: diagnostic and fat-grading accuracy of low-flip-angle multiecho gradient-recalled-echo MR imaging at 1.5 T. Radiology. Radiological Society of North America; 2009 Apr;251(1):67–76.
3. Pooler BD, Hernando D, Ruby JA, Ishii H, Shimakawa A, Reeder SB. Validation of a motion-robust 2D sequential technique for quantification of hepatic proton density fat fraction during free breathing. J Magn Reson Imaging. John Wiley & Sons, Ltd; 2018 Dec;48(6):1578–85.
4. Zhao R, Zhang Y, Wang X, Johnson KM, Reeder SB, Hernando D. Motion-Robust, High-SNR Fat Quantification using a Variable Flip Angle Approach. 27th ISMRM Annual Meeting 2019; pp. 1–2. https://www.ismrm.org/19/program files/O23.htm.
5. Luo, Huiwen, Curtis Wiens, Ann Shimakawa, Scott B Reeder, Kevin M Johnson, and Diego Hernando. “A Novel Fat and Iron Quantification Technique with Non-Rigid Motion-Corrected Averaging Based on Non- Local Means,” Proc. Intl. Soc. Mag. Reson. Med. 25 (2017): 1019.
6. Zhang X, Hou G, Ma J, et al. Denoising MR images using nonlocal means filter with combined patch and pixel similarity. PLoS One. 2014;9(6):e100240. Published 2014 Jun 16. doi:10.1371/journal.pone.0100240
7. Hernando D, Kellman P, Halder JP, Liang ZP. Robust water/fat separation in the presence of large field inhomogeneities using a graph cut algorithm. Magnetic resonance in medicine: official journal of the Society of Magnetic Resonance in Medicine/Society of Magnetic Resonance in Medicine.2010; 63(1):79-90
Figures
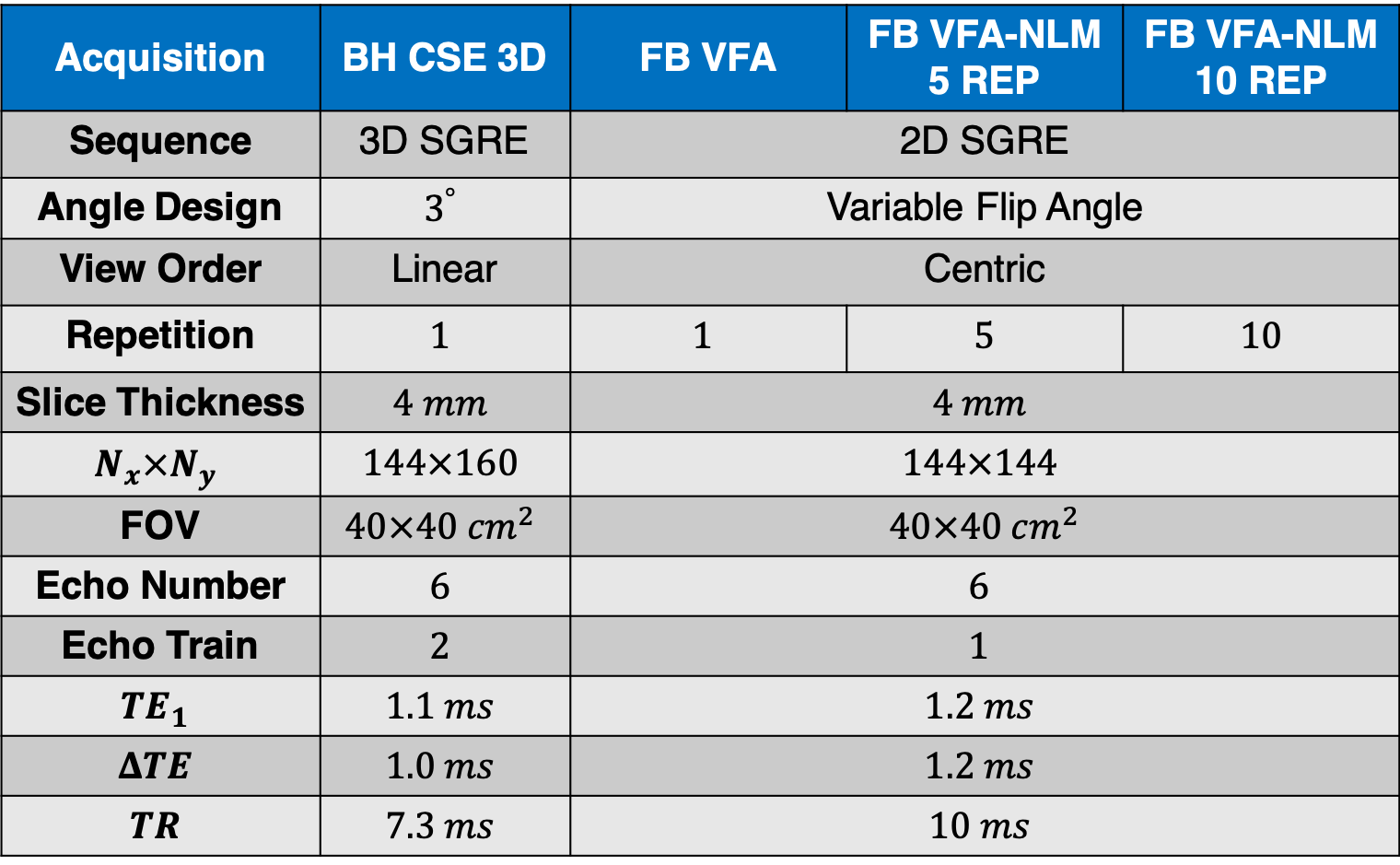
Table 1 MR scan acquisition parameters used in the study.
(2D two dimensional; 3D, three dimensional; BH, breath-hold; FB, free-breathing; FOV, field of view; NLM, nonlocal means; REP, number of repetitions; TE, echo time; TR, repetition time, SGRE, spoiled gradient echo; VFA, variable flip angle)
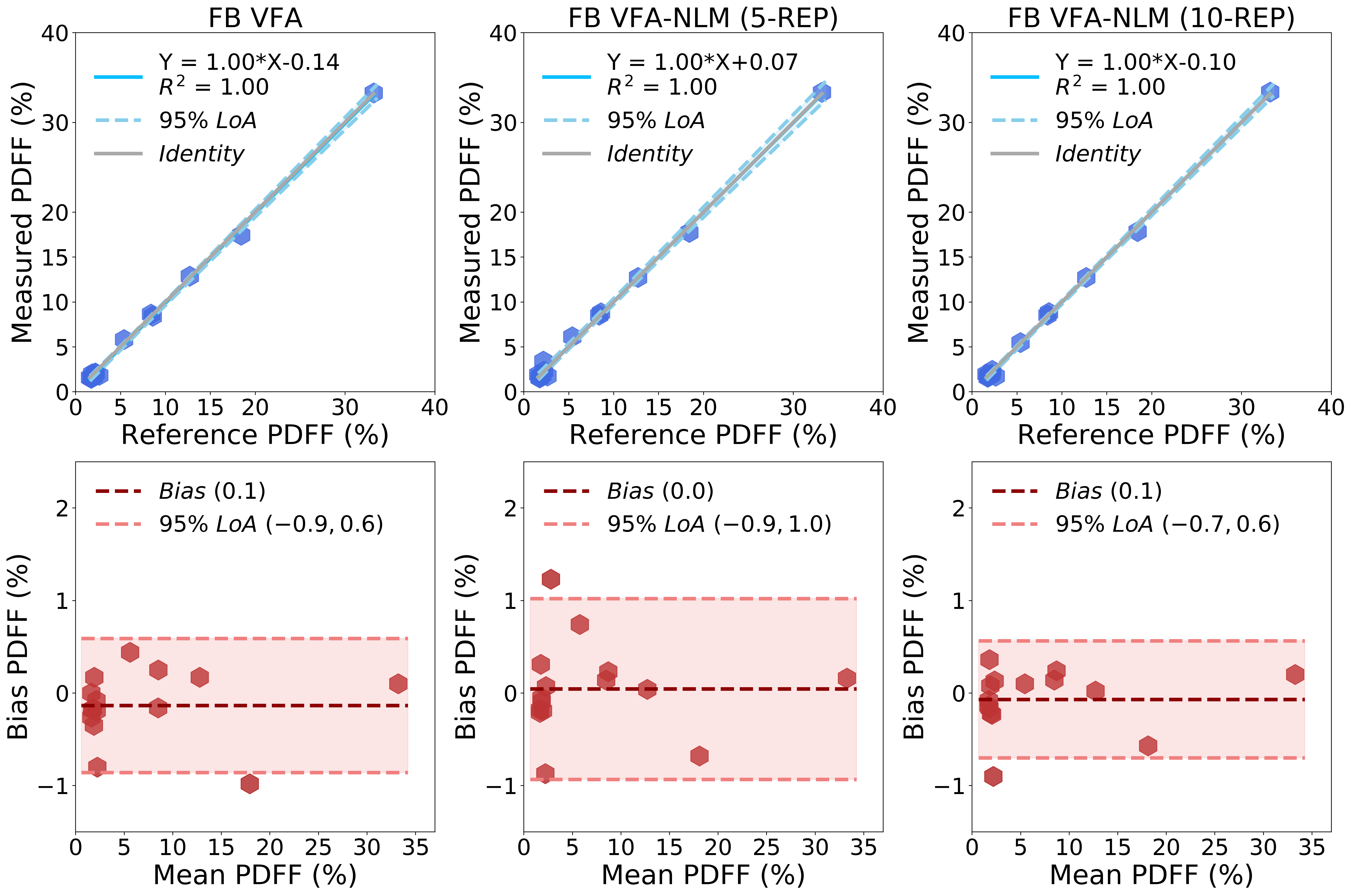
Figure 1 Free-breathing VFA-NLM provided similar PDFF measurements compared to the breath-held 3D CSE reference independently of the number of repetitions.
(BH, breath-hold; FB, free-breathing; NLM, nonlocal means; REP, number of repetitions; PDFF, proton density fat-fraction; SNR, signal to noise ratio; VFA, variable flip angle)
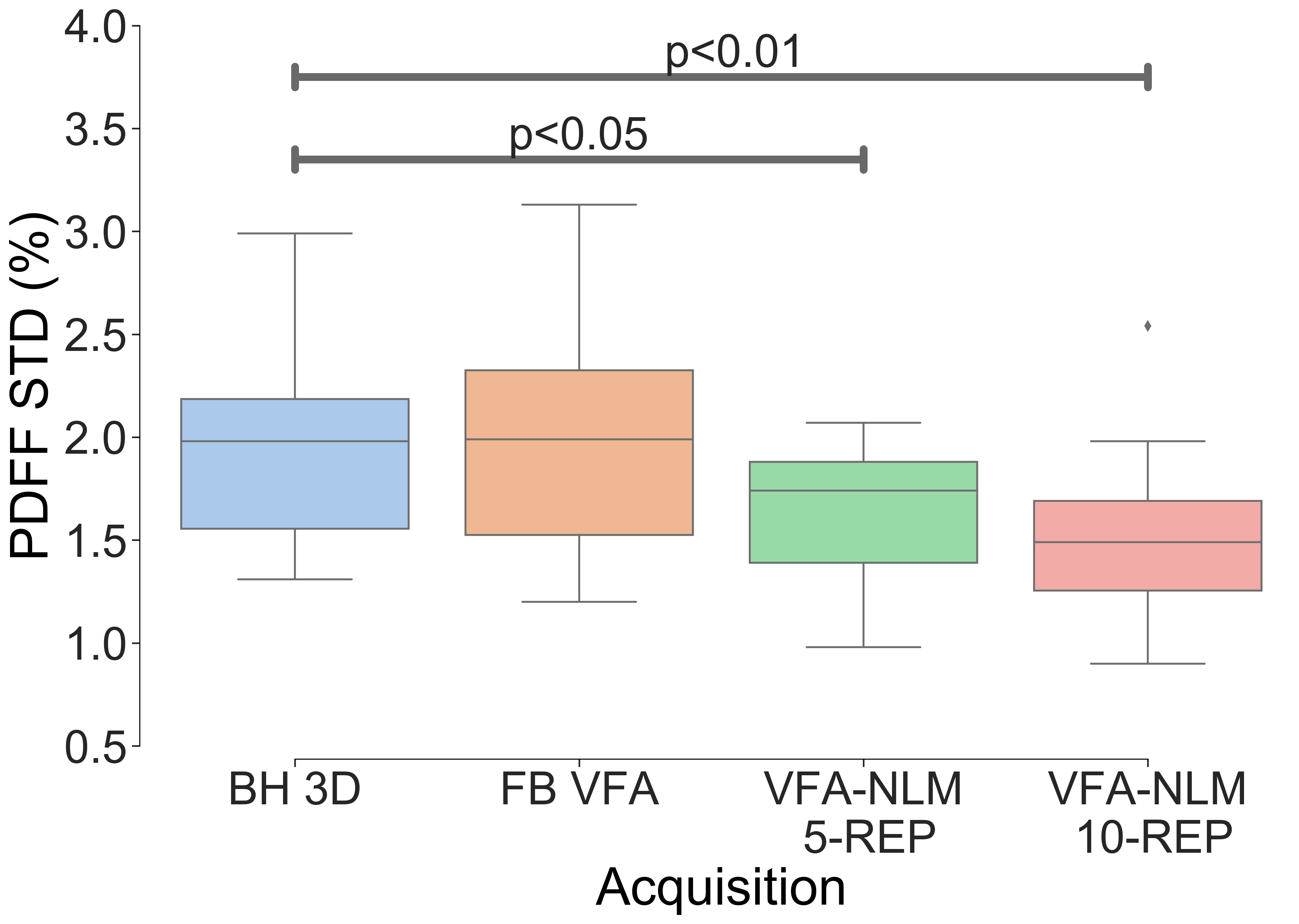
Figure 2 In comparison to the breath-held 3D CSE reference, free-breathing multi-repetition VFA-NLM technique provides enhanced signal-to-noise ratio, which improves with increasing numbers of repetitions.
(3D, three dimensional; BH, breath-hold; FB, free-breathing; NLM, nonlocal means; PDFF, proton density fat-fraction; REP, number of repetitions; STD, standard deviation, VFA, variable flip angle)
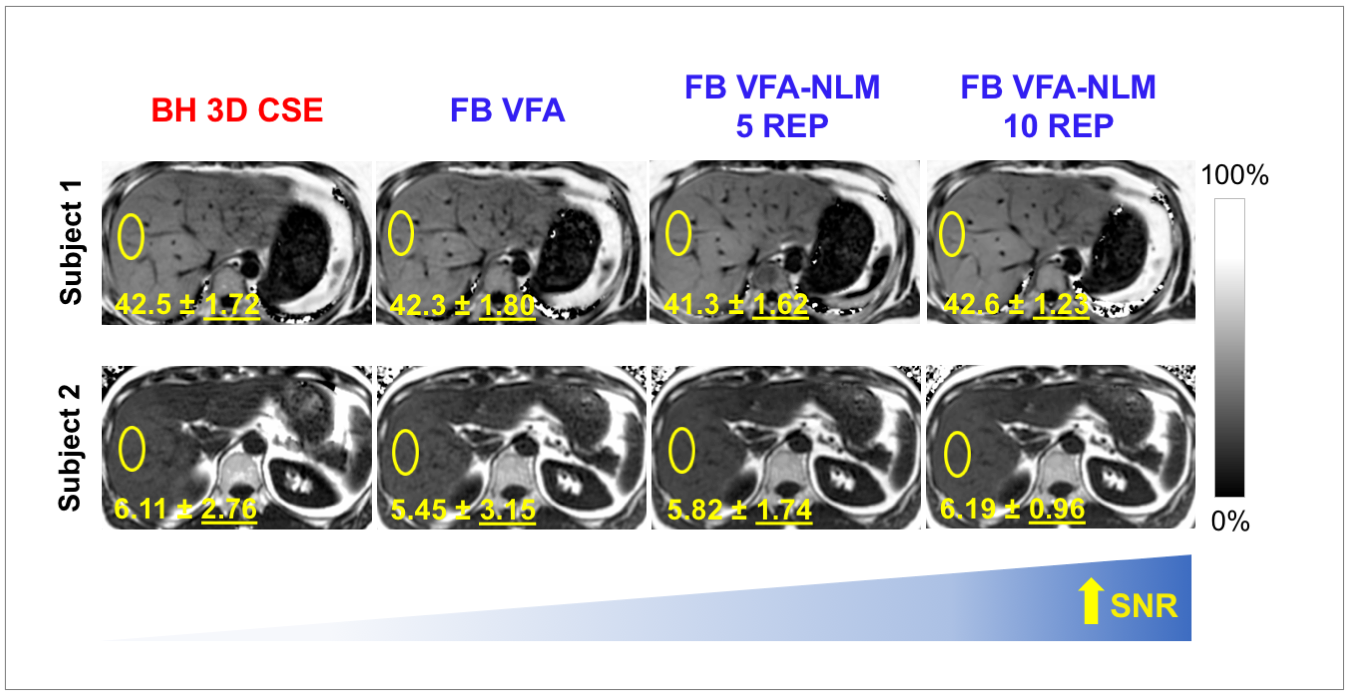
Figure 3 Representative PDFF maps from two subjects with and without fatty liver demonstrating the increased signal-to-noise ratio with increasing number of VFA-NLM repetitions.
(3D, three dimensional; BH, breath-hold; CSE, chemical shift-encoded; FB, free-breathing; NLM, nonlocal means; REX, number of repetitions; SNR, signal to noise ratio; VFA, variable flip angle)
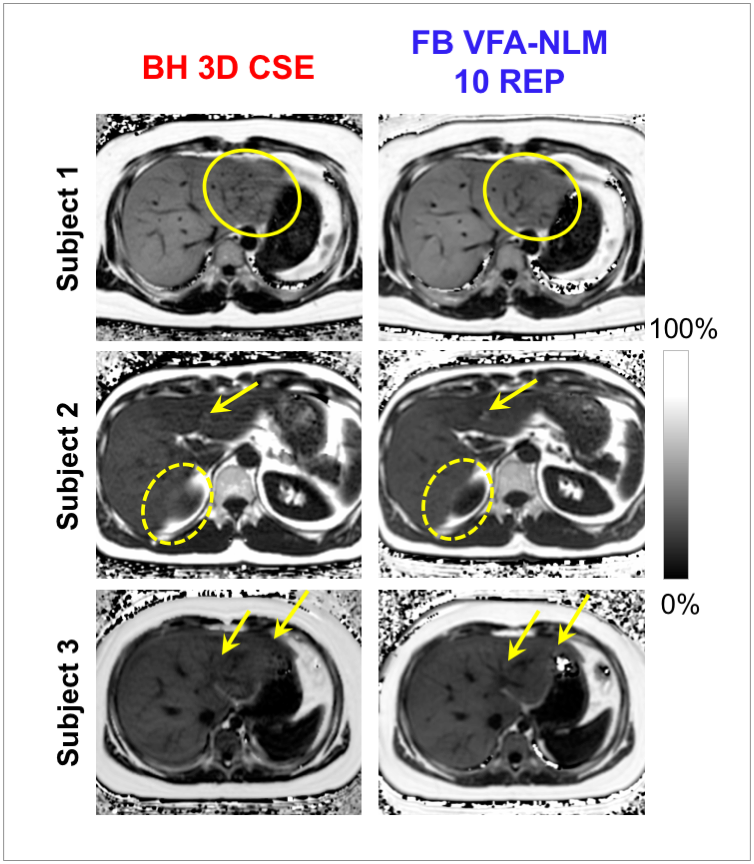
Figure 4 Representative PDFF maps demonstrating improved image quality in three subjects using multi-repetition VFA-NLM in comparison to 3D CSE. Reduction of motion blurring artifacts (marked with oval), improved visibility of image details (arrows) and better definition of organ boundaries (dashed oval) can be observed.
(3D, three dimensional; BH, breath-hold; CSE, chemical shift-encoded; FB, free-breathing; VFA, variable flip angle; NLM, nonlocal means; REP, number of repetitions)