0326
Free Breathing Dynamic Contrast Enhanced MR Imaging of the Hepatopancreatobiliary lesions with improved 3D Stack-of-Stars k-space trajectory
Takayuki Masui1, Motoyuki Katayama1, Yuji Iwadate2, Naoyuki Takei2, Mitsuharu Miyoshi2, Masako Sasaki1, Takahiro Yamada1, Ty Cashen3, Sagar Mandava4, and Kang Wang5
1Radiology, Seirei Hamamatsu General Hospital, Hamamatsu, Japan, 2Global MR Applications and Workflow, GE Healthcare, Hino, Japan, 3Global MR Applications and Workflow, GE Healthcare, Madison, WI, United States, 4GE Healthcare, Tucson, AZ, United States, 5GE Healthcare, Waukesha, WI, United States
1Radiology, Seirei Hamamatsu General Hospital, Hamamatsu, Japan, 2Global MR Applications and Workflow, GE Healthcare, Hino, Japan, 3Global MR Applications and Workflow, GE Healthcare, Madison, WI, United States, 4GE Healthcare, Tucson, AZ, United States, 5GE Healthcare, Waukesha, WI, United States
Synopsis
The feasibility of dynamic Gd-contrast study for evaluation of hepatopancreatobiliary lesions under free breathing was demonstrated. Superb image quality with high temporal resolutions could be obtained using a stack-of-stars k-space trajectory with golden angle ordering a CG-SENSE algorithm that supports parallel imaging and soft-gating for accelerated motion robust imaging. Selective recognition of vasculatures and lesions in the liver and pancreas can be made with this technique, which may be equivalent to fast breath-hold dynamic contrast image in young and old aged population.
Introdcution
Breath-hold dynamic contrast MR study has provided information of characterization of abdominal lesions. To obtain higher temporal and spatial resolution images, faster imaging technique has been desired. A stack-of-stars k-space trajectory with golden angle ordering (SOS) has been used for free breathing dynamic contrast study(1). Still image quality and contrast resolution might not be satisfactory due to the inherent features of radial k-space sampling comparing breath-held fast imaging especially with Cartesian trajectory. Recently 3D imaging technique using SOS for improved temporal resolution and signal to noise ration(SNR) has been developed to evaluate upper abdominal regions (LAVA-Star, GEHC) with administration of nonspecific Gd-chelate. Accordingly, the purpose was to evaluate feasibility of free breathing dynamic contrast study using LAVA-Star with nonspecific Gd-chelate for evaluations of hepatopancreatobiliary regions.Materials and Methods
The current study was approved by the institutional review board and informed consent was obtained from all the patients. Population: A total of twenty patients (12men, 8 women, mean 71years old) who underwent Gd contrast enhanced MR imaging for the evaluation of hepatopancreatobiliary lesions. Pathologies were as follows; pancreatic cystic lesions 8 cases, Pancreatic cancer 1, Hepatic Cysts 5, Gall Bladder(GB): Cholecystitis GB stone 1, Adenomyomatosis 2, Normal 3. MR imaging: MR imaging was performed on a 3T system (Discovery 750, GEHC) using 32 channel phased array multicoil. Dynamic contrast 3D imaging covering the liver and pancreas in a transverse plane was performed using LAVA-Star pulse sequence, a stack-of-stars k-space trajectory with golden angle ordering and intermittent fat suppression pulse. High temporal resolution dynamic image phases were reconstructed using a CG-SENSE algorithm that supports parallel imaging and soft-gating for accelerated motion robust imaging. A low rank filter was also applied to the temporal datasets to suppress streaking artifact and improve overall SNR. The following parameters were used; TR 2.5ms, TE1.2ms, no rap factor 1.5, ARC factor 2, Matrix 288x180, FOV350mm, slice thickness 3-4mm/-1.5-2mm, 180spokes per phase. After obtaining MASK imaging, continuous acquisition of data were made for 90sec after the injection of the nonspecific Gd-chelate (Gadobutrol, 0.1mmol/kg body weight, injection rate 1mL/sec) followed by saline flash (20mL, 2mL/sec). Resultantly, approximately 120images /phase were reconstructed with temporal resolution of 5seconds in total of 18-20 phases. Evaluations: In all cases, precontrast images, images in the phase for the right ventricle(RV), left ventricle(LV), in the arterial phase(in hepatic artery was dominantly enhanced), and portal phase (80-90 seconds after contrast injection), were selected. Those images were evaluated regarding image quality, blurring and streaking artifacts using five-point scale (1 non-diagnostic or sever artifacts to 5 excellent quality or no blurring). Selective recognition of enhanced vasculature and pancreas was also evaluated, respectively. Subjective recognition of lesions was made: Liver lesion: Cystic, without enhancement compared with surrounding hepatic parenchyma; Solid, with massive or nodular enhancement; Pancreas; Cystic, Low SI without massive enhancement; Solid, dominant enhancement.Results
Over all, image quality was good except in the phases in which the contrast medium dominantly staying in the RV and LV, causing prominent streaking artifacts (Fig 1). Precontrast images showed acceptable image quality (Fig 1-2) indicating high signal intensity of the pancreatic parenchyma. Stable image quality with less blurring was recognized (Fig 1 and 2). Selective enhancement of the hepatic artery was recognized in all cases without concurrent enhancement of the portal veins and hepatic veins. Selective enhancement of other portal and hepatic venous vasculatures and the pancreatic parenchyma was noted in call cases.All the solid and cystic lesions in the liver, pancreatic cystic and solid lesions were correctly identified. Pancreas, Cystic lesions including intraductal papillary mucinous neoplasm (IPMN) 8/8cases, Liver, Hepatic Cysts; 5/5. GB adenomyomatosis 2/2.
Discussions
Dynamic contrast MR imaging with high temporal resolutions under free breathing could be successfully obtained for the evaluation of the liver and pancreas. Feasibility of this technique could be demonstrated. With LAVA-Star pulse sequence, dynamic contrast images in phases were reconstructed using a CG-SENSE algorithm for accelerated motion robust imaging and a low rank filter. The images with high temporal resolution and high SNR with fewer artifacts selectively visualized the hepatic arteries, portal veins, pancreatic parenchyma and cystic and solid lesions in the pancreas.Limitation: Study population was small. To characterize the various lesions in the liver and pancreas, we may perform the study in larger population.
Conclusion: Using LAVA-Star with improved features, dynamic contrast MR study for hepatopancreatobiliary lesions under free breathing can be performed with high image quality and recognitions of lesions and vasculartures.
Acknowledgements
References
1)Z. Zhou, Magn Reson Med 78:2290–2298, 2017.Figures
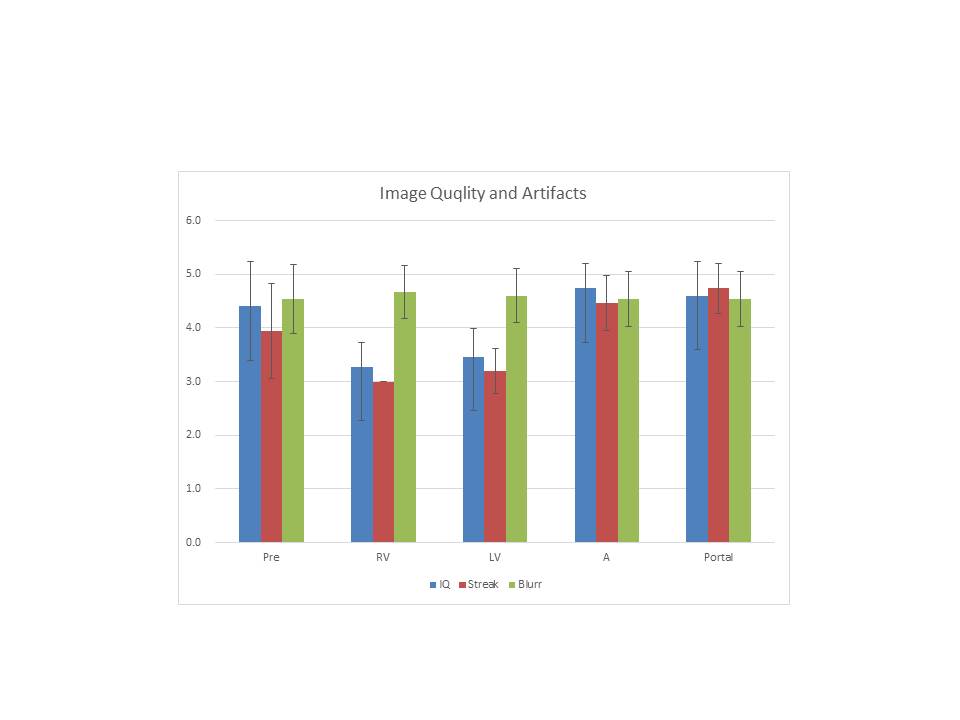
Image Quality and Artifacts
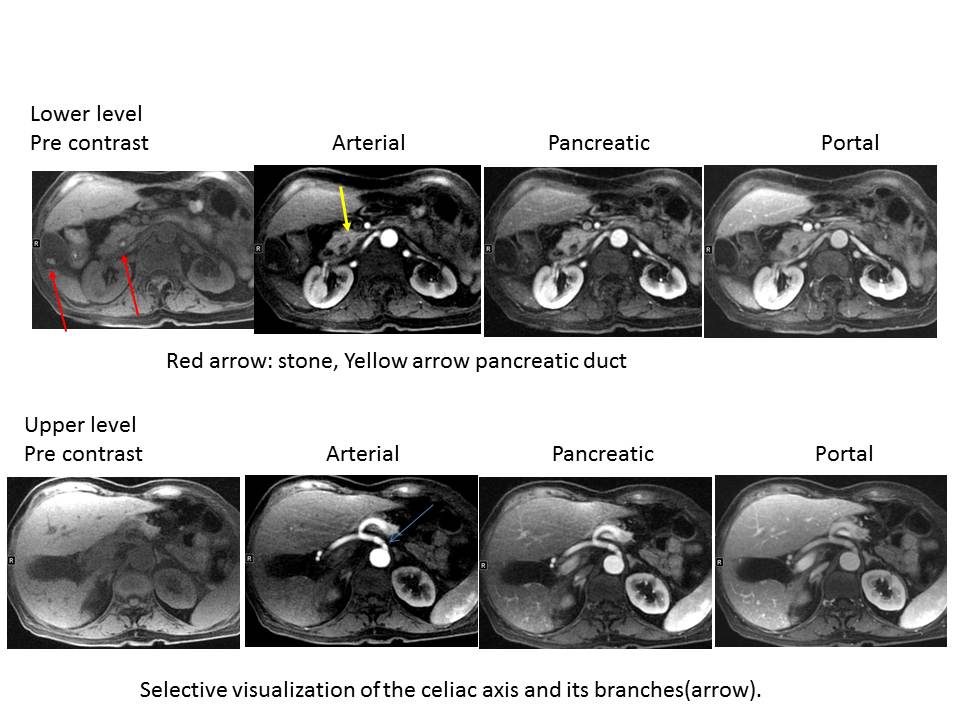
GB&Bile duct stone, 70years old, Woman