0301
Possibility of the Reduction of Gd Dose using Spiral Spin-Echo Method for Contrast Enhanced Scans at 3.0T
Ravi Varma Dandu1, Rithika Varma Dandu2, Karthick Raj Rajendran3, Narayana Rolla4, and Indrajit Saha5
1Citi Neuro Centre, Hyderabad, India, 2RV College of Engineering, Bengaluru, India, 3Philips Healthcare, Eindhoven, Netherlands, 4Philips Healthcare, Bangalore, India, 5Philips Healthcare, Gurgaon, India
1Citi Neuro Centre, Hyderabad, India, 2RV College of Engineering, Bengaluru, India, 3Philips Healthcare, Eindhoven, Netherlands, 4Philips Healthcare, Bangalore, India, 5Philips Healthcare, Gurgaon, India
Synopsis
This study compares the performance of spin echo T1 with spiral k-space filling and three other techniques, for post contrast T1-weighted imaging of the brain. The lesion enhancement in each technique was evaluated after incremental fractional doses of gadolinium injection. The enhancement achieved on T1-FFE and T1-TSE techniques with full dose contrast could be achieved with 50% to 75% dose contrast in spiral imaging. Spiral imaging can thus be used to reduce the dose of injected contrast medium (by at least 25% and up to 50%) without compromising on the diagnostic quality of the post contrast study.
Introduction
In routine clinical radiology practice, patients with brain tumors are generally injected with Gadolinium based contrast agents (GBCA) for confirmed diagnosis. Considering the potential risks of repeated gadolinium injections, it is desirable to reduce the dose of injected GBCA without compromising on the diagnostic accuracy1. Post contrast T1 weighted imaging can be performed with a variety of spin-echo (SE) and gradient-echo based pulse sequences; however, Though the enhancement effect of GBCAs is better in SE, the longer scan times associated such sequences prevent their use for post contrast imaging at 3T2,3. On the other hand, Spiral k-space filling for acquisition of MR signal has the potential to provide greater signal and faster scans with minimal artefacts. This method can be coupled with SE T1-w sequences for the acquisition of excellent T1 weighted images with relatively higher SNR at shorter scan times4. The purpose of this study is to evaluate whether the Spiral spin-echo T1 MRI can help in lowering down the dose of injected GBCA for brain tumours.Methods
In this study, pre and post contrast T1-w imaging were performed in 32 patients with enhancing brain lesions using 2D spiral SE T1 technique and one of the traditional T1 techniques: 2D-T1 Fast Field Echo (2D-T1 FFE), 2D-T1 Turbo Spin Echo (2D-T1 TSE) or 3D T1 Turbo Field Echo (3D-T1 TFE). Imaging was performed using a 32-element head coil on a 3.0T MRI (Ingenia at R5.6 software release, Philips Healthcare, Best, Netherlands). The calculated dose of contrast medium was injected in four divided doses. One set of traditional T1 acquisition and SE spiral T1 acquisition was performed before the injection of contrast and one minute after each divided dose of contrast (to allow for enhancement and equilibrium) - Figure 1. The imaging parameters are summarized in Figure 2.Images from the precontrast and split-dose post-contrast images (25%, 50%, 75%, and 100% contrast dose) of the traditional and spiral acquisitions were loaded simultaneously into Intellispace Portal Workstation (Philips, Best, Netherlands). After excluding movement between different image sets, an ellipsoidal region of interest (ROI) was drawn manually on the final post contrast (100% dose) spiral T1 image. Homogenously enhancing part of the lesion far from the skull base, without vascular channels or pulsation artefacts was chosen for ROI placement. ROI were also drawn in the grey matter and white matter. The ROIs were copied onto the precontrast images and other phases of post contrast study (25%, 50% and 75% dose); as well as corresponding images acquired using the traditional T1 technique. The signal intensities and standard deviations were tabulated. The variations in lesion signal intensity produced by different image acquisition strategies were removed by taking Lesion-WM ratio using the WM signal in the same slice:
Lesion-WM Ratio = SILesion/SIWM
The following metrics were calculated:
a. Grey matter – White matter CNR: CNRWM-GM = (SIWM – SIGM) / SDWM
b. Enhancement ratio for each dose was calculated as ratio of Lesion-WM Ratio between that dose and plain study : Enhancement Ratio = Lesion - WM RatioDose / Lesion - WM RatioPlain
c. Lesion Contrast – Noise Ratio for each dose: Lesion CNR = (SILesion - SIWM) / SDWM
(CNR = Contrast – Noise Ratio, GM = Grey Matter, WM = White Matter, SI = Signal Intensity, SD = Standard Deviation)
Results
The GM – WM CNR was consistently higher in spiral SE T1 as compared to 2D-T1 FFE and 2D-T1 TSE . On post contrast imaging, spiral SE imaging showed greater enhancement ratios as compared to 2D-T1 FFE and 2D-T1 TSE for all doses. The enhancement ratio in spiral imaging with 50% to 75% dose of contrast injection was superior to that achieved on T1-FFE or T1-TSE sequences with full dose contrast (Figure 3). Spiral SE T1 imaging however, showed inferior grey – white matter contrast to noise ratio and poorer enhancement as compared with 3D-T1 TFE technique. Calculated lesion – WM CNR was higher with spiral imaging than with T1-FFE or T1-TFE. However, T1-TSE imaging and spiral imaging demonstrated similar lesion- WM CNR; presumably due to lower noise levels in the TSE technique.(Figure 4)Discussion
Spiral imaging uses a unique k-space traversal which gives excellent signal to noise ratio. Thus, spiral SE T1 imaging permitted acquisition of T1 images with higher spatial resolution than any of the traditional T1 imaging techniques in equivalent scan times. The T1 contrast achieved with 2D spiral SE T1 imaging was superior to 2D T1-FFE or 2D T1-TSE imaging, resulting in greater lesion enhancement on post contrast study. Spiral imaging can thus be used to reduce the dose of injected contrast medium (by atleast 25% and up to 50%) without compromising on the diagnostic quality of the post contrast study. 3D T1-TFE imaging showed better T1 contrast than spiral imaging; however, the CNR with spiral imaging was better, presumably due to higher noise levels in the TFE technique.Conclusion
Spiral SE T1 imaging shows potential in achieving excellent T1 weighted images by combining the sensitivity of Spin echo with the speed of spiral k-space filling. This technique can be used to reduce the dose of injected GBCAs by 25% or more.Acknowledgements
No acknowledgement found.References
- Layne KA, Dargan PI, Archer JRH, Wood DM. Gadolinium deposition and the potential for toxicological sequelae - A literature review of issues surrounding gadolinium-based contrast agents. Br J Clin Pharmacol 2018; 84(11):2522-2534
- Elster AD. How much contrast is enough? Dependence of enhancement on field strength and MR pulse sequence. Eur Radiol. 1997; Suppl 5: S276-S280.
- Furutani K, Harada M, Mawlan M, Nishitani H. 3-Dimensional Fast Spoiled Gradient Recalled Acquisition in Steady State Magnetic Resonance Imaging of Brain Metastasis at 3-T Magnetic Resonance Imaging. J Comput Assist Tomogr 2008;32:313-319
- Li Z, Karis JP, Pipe JG. A 2D spiral turbo-spin-echo technique. Magn Reson Med 2018; 80(5): 1989-1996
Figures
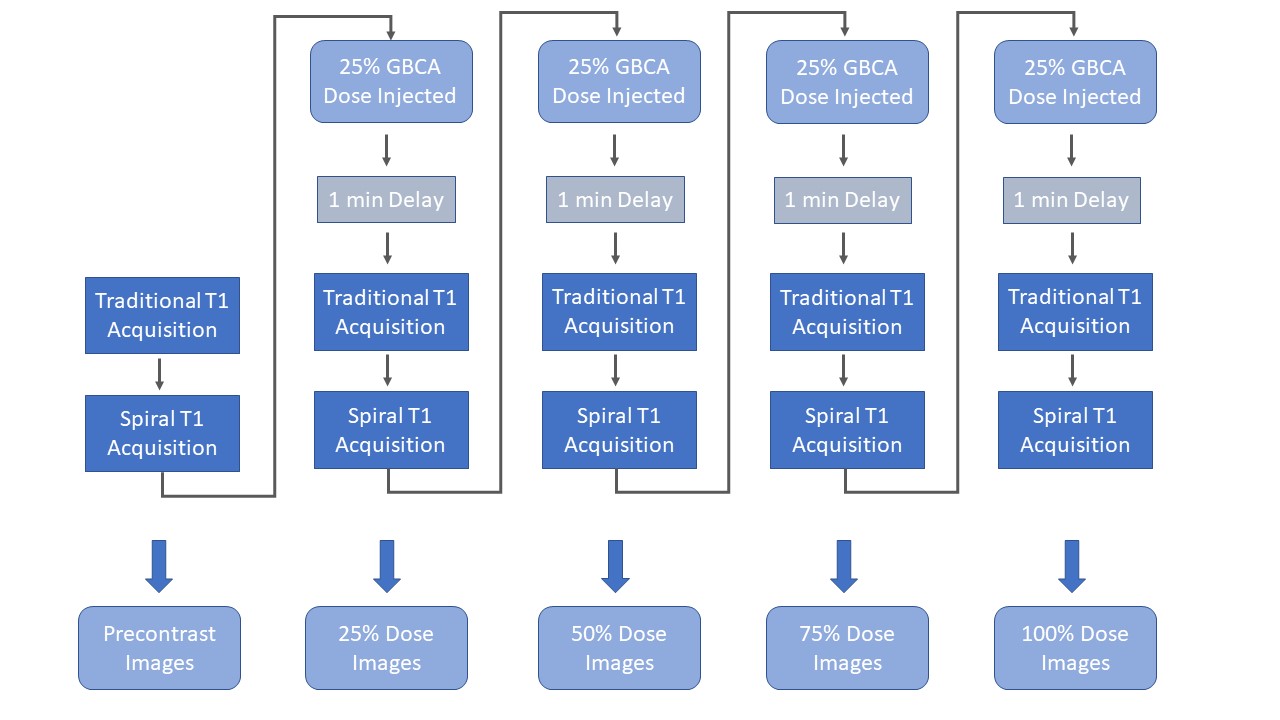
Figure 1:
Flow chart depicting the temporal sequence
of image acquisitions and split-dose contrast injections performed during the
study
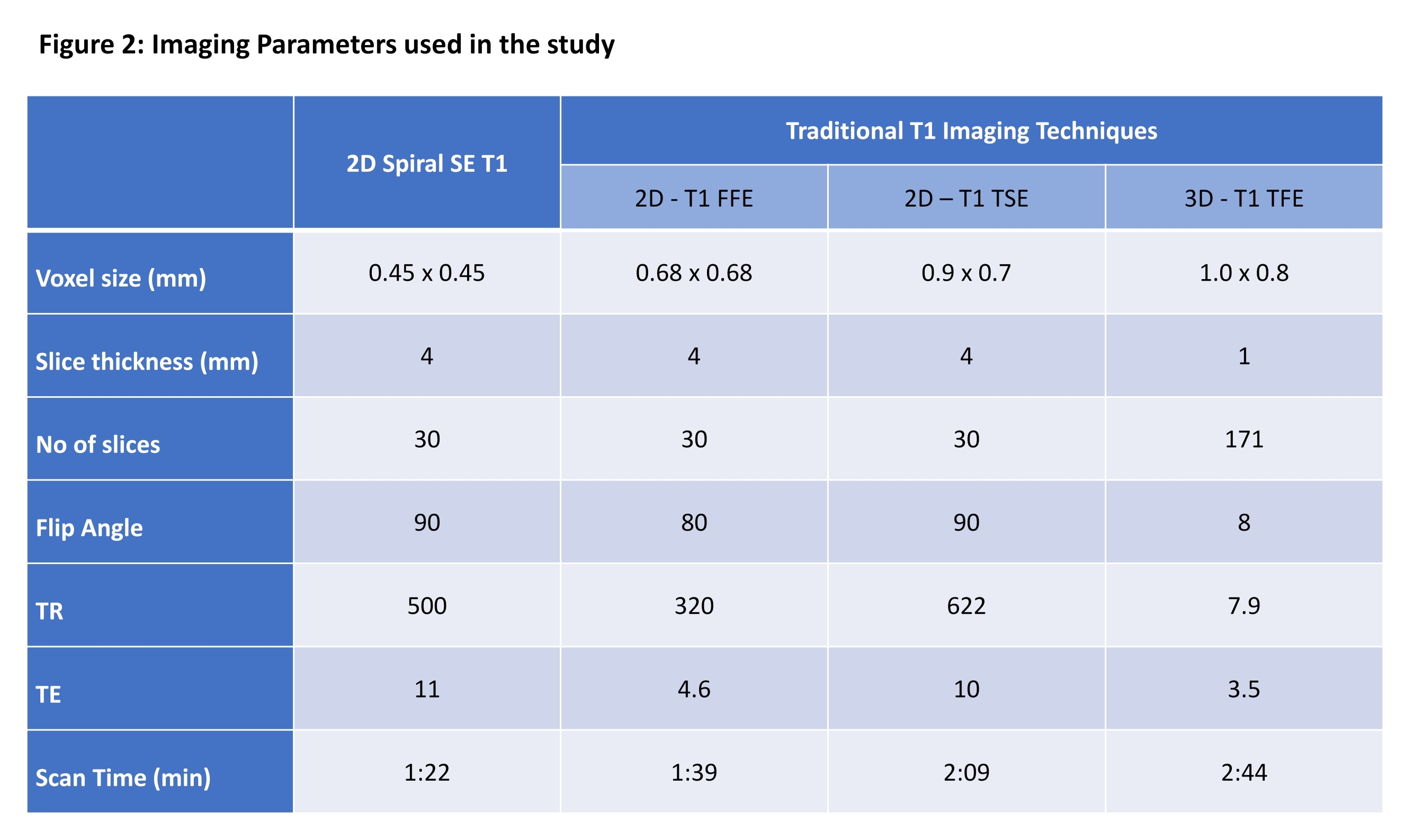
Figure 2:
Imaging
Parameters used in the study
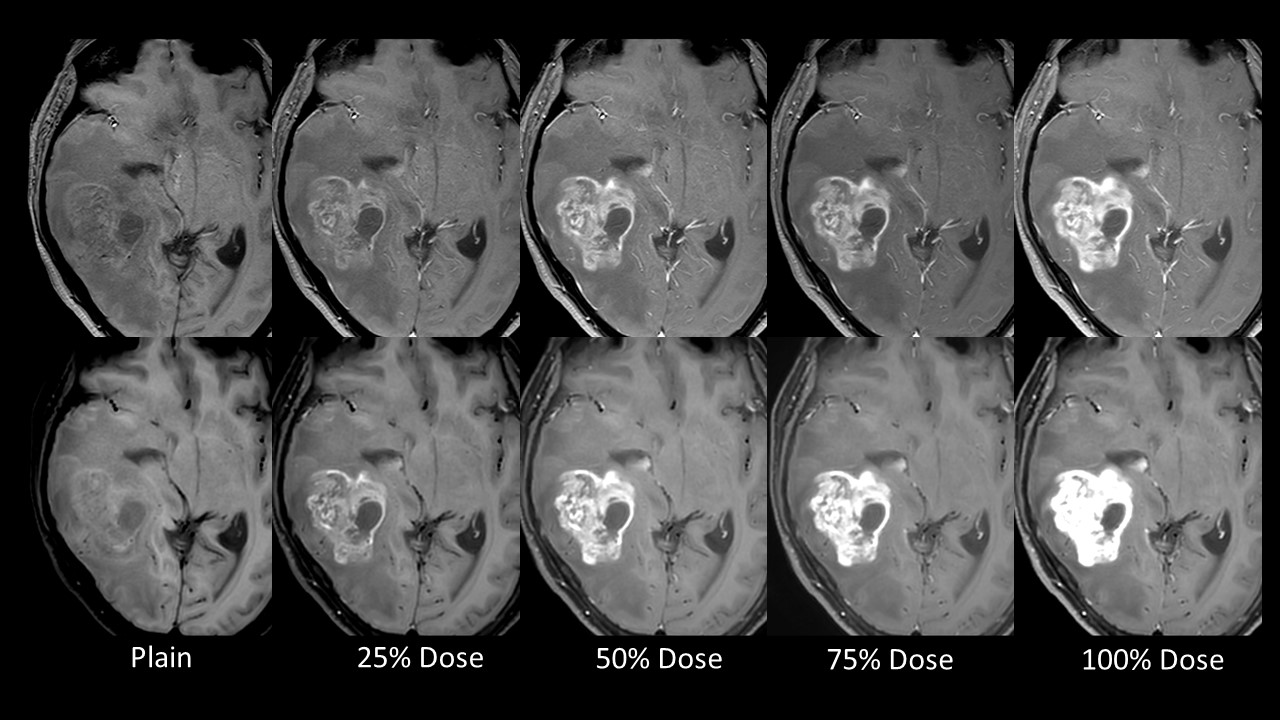
Figure 3:
Images from a patient with right
temporoparietal high-grade glioma. The upper panels depicts plain and split
dose contrast images acquired using a traditional T1 weighted technique
(T1-FFE), while the lower panel depicts the corresponding spiral images.
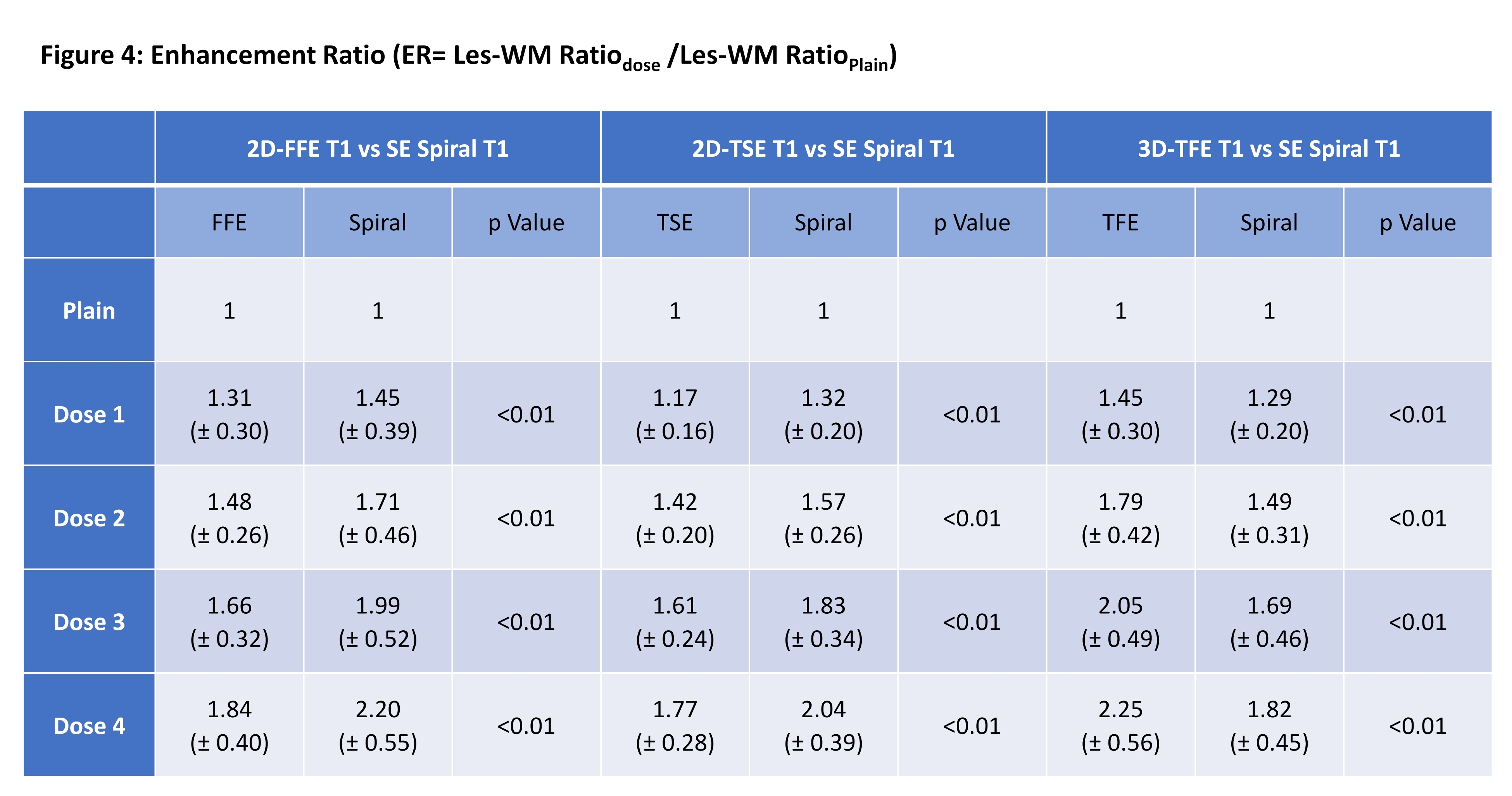
Figure 4:
Enhancement Ratio obtained in the study