0300
A comprehensive multi-shot EPI protocol for high-quality clinical brain imaging in 3 minutes1Radiology, Massachusetts General Hospital, Boston, MA, United States, 2Siemens Medical Solutions, Boston, MA, United States, 3Massachusetts General Hospital, Boston, MA, United States, 4Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
A comprehensive 3 minute whole-brain MRI exam based on multi-shot echoplanar imaging (ms-EPI) was optimized and evaluated in 5 patients with different clinical pathologies. This approach minimizes artifacts associated with single-shot echoplanar imaging, and provides image quality similar to that of a 10-minute clinical reference protocol based on turbo spin-echo imaging.
Introduction
A variety of approaches have been evaluated to efficiently obtain a comprehensive multi-contrast accelerated brain MR exam. Approaches using 2D turbo spin-echo (TSE) sequences and conventional parallel imaging (GRAPPA) have been validated [1,2], but suffer from substantial SNR losses if pushed to higher acceleration factors (e.g., greater than 2-3), limiting the acceleration that can be achieved and resulting in acquisition times of approximately 5 minutes to obtain all desired contrasts [1]. Alternatively, an approach consisting entirely of single-shot multi-contrast echo-planar imaging (ss-EPI) sequences has been recently proposed to achieve higher acceleration, providing all the desired contrasts in 60-90 seconds [3,4]. However, ss-EPI images suffer from geometric distortion near the skull base and paranasal sinuses, and the long echo train duration required by ss-EPI leads to T2* mediated blurring and signal dropout. Furthermore, while the integration of multiple sequences into a single scan reduces acquisition times, it places restrictions on protocol design [3]. In this study, we evaluated a comprehensive brain MRI acquisition based on multi-shot echo-planar imaging (ms-EPI) sequences that minimizes artifacts and produces clinically acceptable images in under 3 minutes.Methods
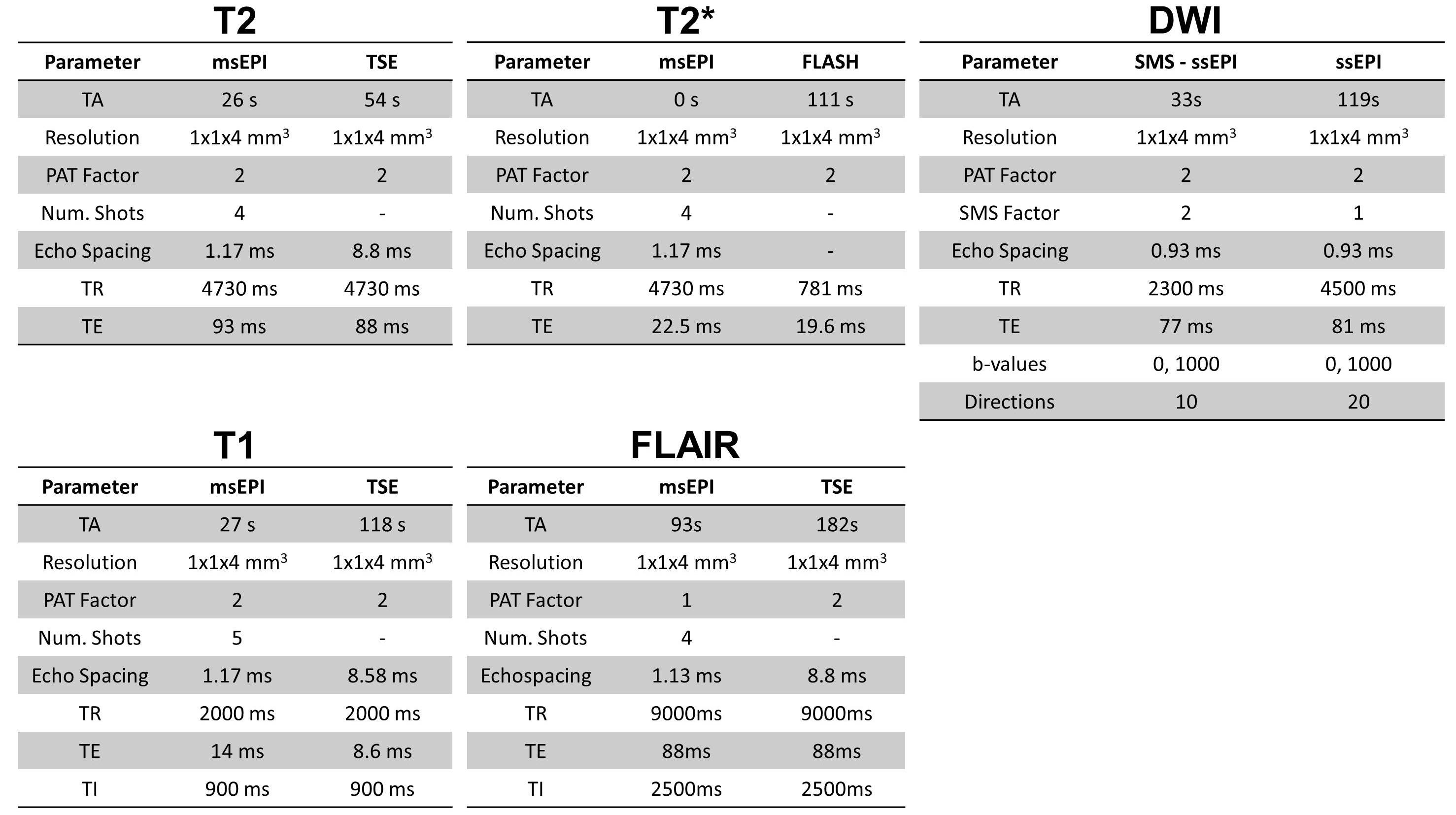
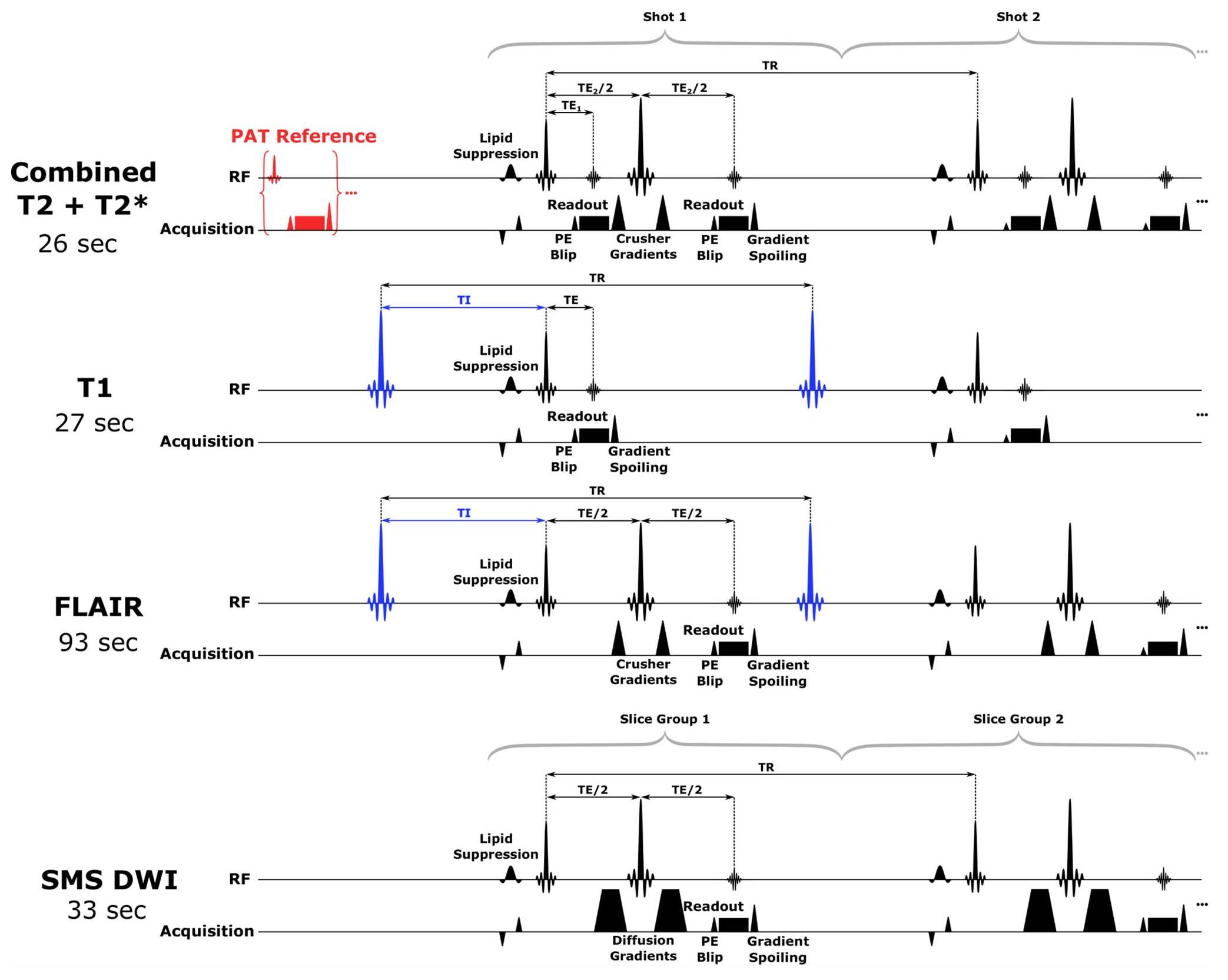
This study was approved by the Institutional Review Board (IRB) and was Health Insurance Portability and Accountability Act (HIPAA) compliant. Five patients (3 male, 2 female, ages 61 to 77 years) with different clinical pathologies and a healthy volunteer without clinical pathology underwent brain imaging using a clinical reference protocol from our institution and an optimized fast ms-EPI protocol (Fig. 1). The healthy control underwent additional imaging using ss-EPI sequences (to demonstrate associated artifacts) and a single slice TSE FLAIR acquisition (to demonstrate the contribution of magnetization transfer to the FLAIR image contrast). All subjects provided informed written consent. The data were collected on two 3T MRI systems (MAGNETOM Prisma and MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) using a 32-channel head coil. The prototype fast acquisition was implemented (Fig. 2) and included the following sequences: T2 and T2*-weighted images obtained using a combined spin-echo and gradient-echo ms-EPI acquisition; T1-weighted images obtained using an inversion-recovery (IR) prepared gradient-echo ms-EPI acquisition; T2-FLAIR images obtained using an IR prepared spin-echo ms-EPI acquisition; and SMS ss-EPI diffusion-weighted images. Each fast sequence was preceded by a 2.5 second FLASH reference scan to increase flexibility and robustness to motion (total acquisition time for all sequences 2 min 59 sec). Images were reconstructed using a prototype reconstruction pipeline in which the data from all interleaved acquisitions was combined and reconstructed using GRAPPA. The clinical reference protocol included: Turbo Spin-Echo (TSE) T1-weighted images, T2-weighted images and FLAIR images images, FLASH gradient-echo T2*-weighted images, and ss-EPI diffusion-weighted images (total acquisition time for all sequences 9 min 45 sec). All images were reviewed by two board certified neuroradiologists.Results
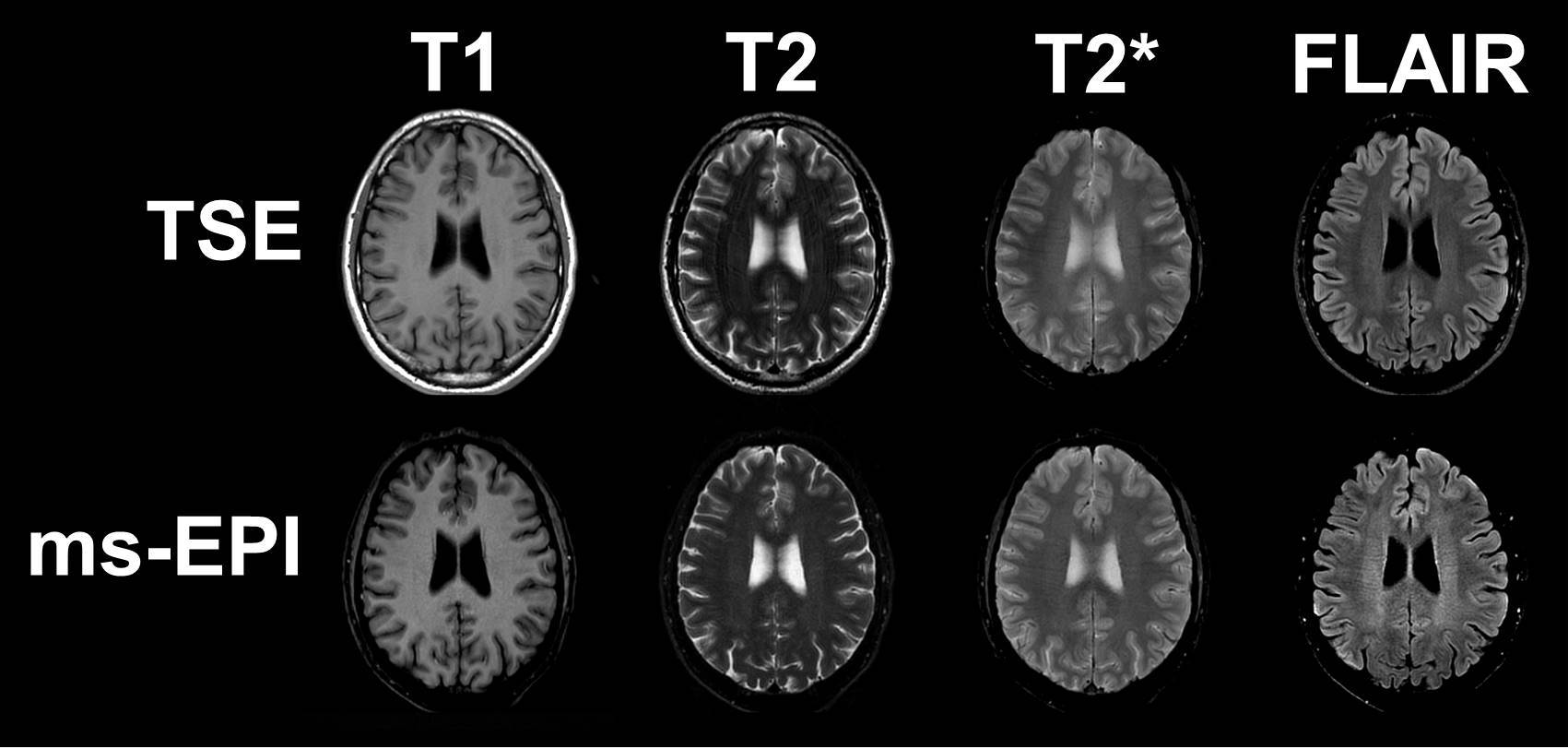
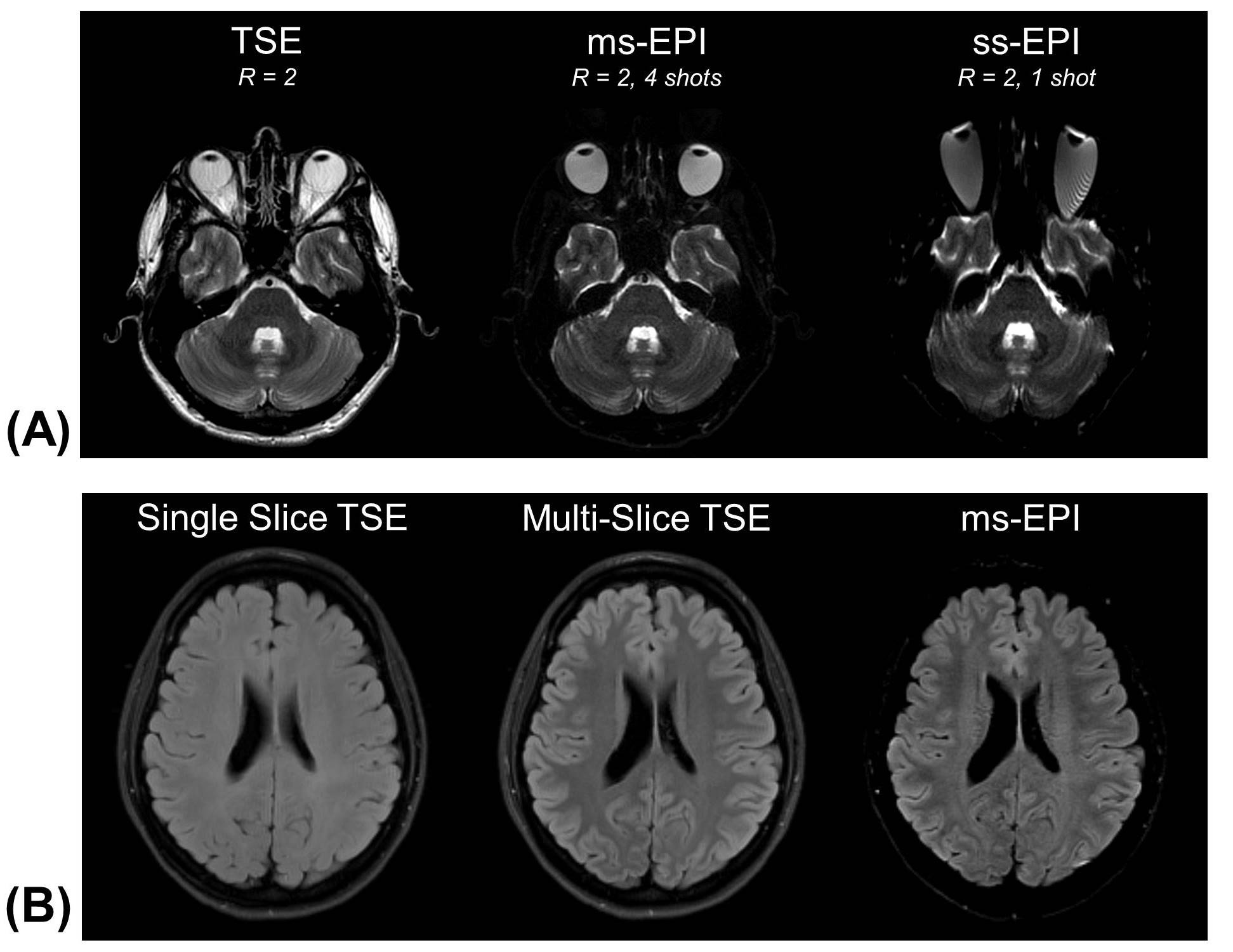
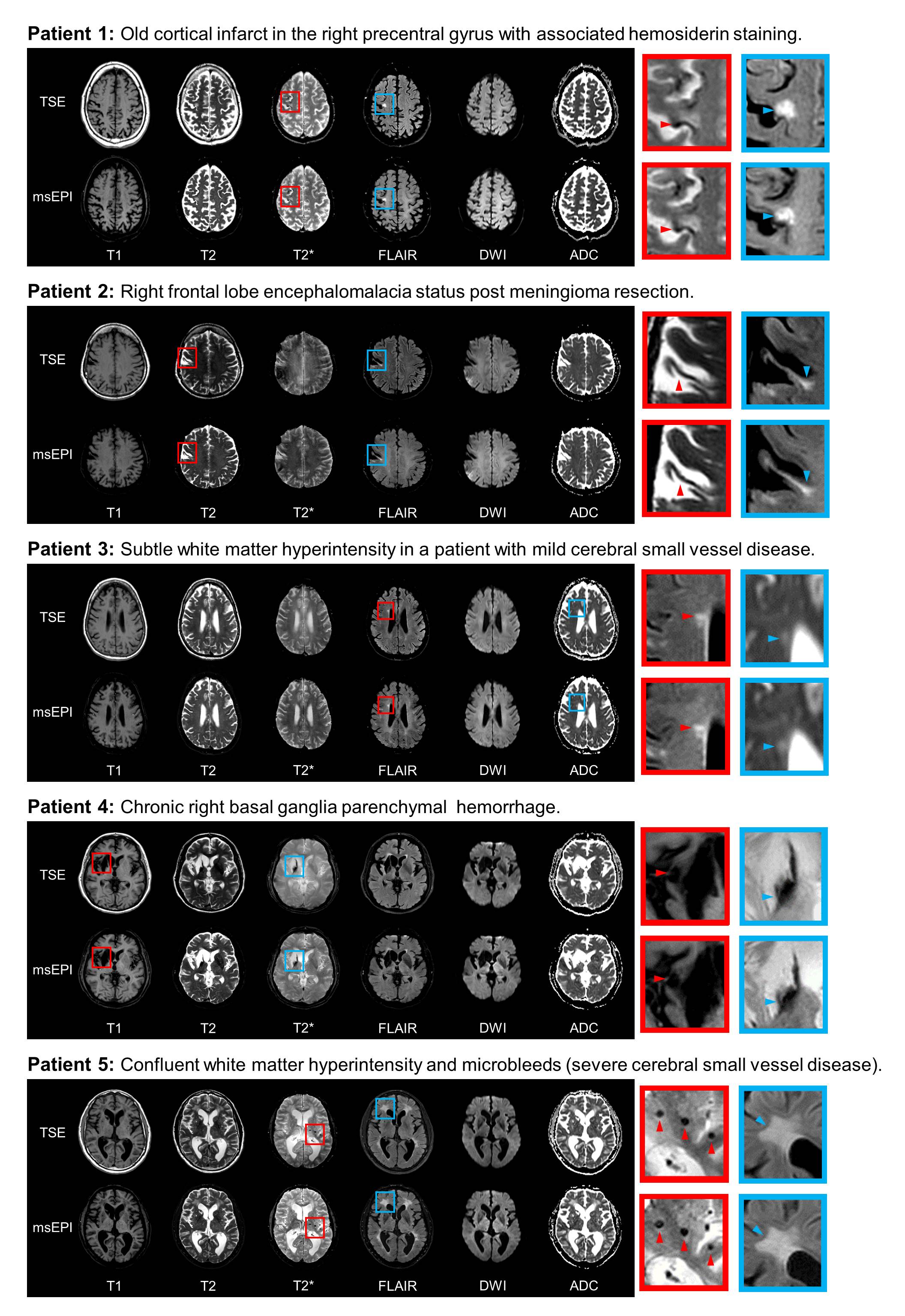
Images were successfully acquired and reconstructed using the fast ms-EPI approach for all study participants. Tissue contrast was similar between the ms-EPI images and clinical reference TSE images for normal brain tissue (Fig. 3). Optimized ms-EPI images showed reduced geometric distortion and signal dropout artifacts near the skull base relative to ss-EPI (Fig. 4A). Mild geometric distortion of the facial soft tissues was still appreciable when compared to 2D TSE sequences. Evaluation of TSE and EPI FLAIR images showed that a substantial contribution to the brain tissue contrast in TSE FLAIR arises from magnetization transfer contrast (MTC) [6] (Fig. 4B). To achieve similar contrast in EPI FLAIR images, an MTC preparation module was included in the acquisition. The optimized ms-EPI FLAIR images (including MTC preparation) provided similar contrast between GM and WM, and similar lesion conspicuity when compared to 2D TSE FLAIR (Fig. 5). Neuroradiologist evaluation of the clinical pathology showed similar lesion conspicuity and overall diagnostic quality between the ms-EPI images and reference TSE images for all 5 patients (Fig. 5).Conclusion
Comprehensive whole-brain MRI using an ms-EPI approach is achievable in under 3 minutes, including all the desired clinical contrasts. Compared to ss-EPI imaging, this approach minimizes signal dropout and geometric distortion near the skull base and paranasal sinuses, providing diagnostic image quality approximating that of the longer 10-minute TSE based reference protocol.Acknowledgements
No acknowledgement found.References
1. Prakkamakul S, Witzel T, Huang S, Boulter D, Borja MJ, Schaefer P, Rosen B, Heberlein K, Ratai E, Gonzalez G, Rapalino O. Ultrafast Brain MRI: Clinical Deployment and Comparison to Conventional Brain MRI at 3T. J Neuroimaging. 2016 Sep;26(5):503-10.
2. Fagundes J, Longo MG, Huang SY, Rosen BR, Witzel T, Heberlein K, Gonzalez RG, Schaefer P, Rapalino O. Diagnostic Performance of a 10-Minute Gadolinium-Enhanced Brain MRI Protocol Compared with the Standard Clinical Protocol for Detection of Intracranial Enhancing Lesions. AJNR Am J Neuroradiol. 2017 Sep;38(9):1689-1694.
3. Delgado AF, Kits A, Bystam J, Kaijser M, Skorpil M, Sprenger T, Skare S. Diagnostic performance of a new multicontrast one-minute full brain exam (EPIMix) in neuroradiology: A prospective study. J Magn Reson Imaging. 2019 [Epub ahead of print].
4. Ryu KH, Choi DS, Baek HJ, Cho SB, Ha JY, Kim TB, Hwang MJ. Clinical feasibility of 1-min ultrafast brain MRI compared with routine brain MRI using synthetic MRI: a single center pilot study. J Neurol. 2019 Feb;266(2):431-439.
5. Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J, Kiefer B, Haase A. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med. 2002 Jun;47(6):1202-10.
6. Bernstein, Matt A. Handbook of MRI Pulse Sequences (pp. 109-110). Elsevier Science. Kindle Edition.
Figures