0278
USPIO-enhanced MRI for pre-operative lymph node staging in patients with pancreatic and periampullary carcinoma: a feasibility study1Radiology and Nuclear Medicine, Radboudumc, Nijmegen, Netherlands, 2Diagnostic and Interventional Radiology, Osaka University Graduate School of Medicine, Suita, Japan, 3Pathology, Radboudumc, Nijmegen, Netherlands, 4Pathology, UMC Utrecht, Utrecht, Netherlands, 5Gastroenterology and Hepatology, Radboudumc, Nijmegen, Netherlands, 6Surgery, Radboudumc, Nijmegen, Netherlands
Synopsis
Detecting lymph node metastases is important but challenging in patients with pancreatic or periampullary carcinoma. USPIO-MRI is a promising tool to detect lymph node metastases. In 13 patients we detected on USPIO-MRI 86/307 suspect lymph nodes (28/78 regional and 58/229 distant). All patients with suspect regional lymph nodes had positive regional lymph nodes at histopathology. In evaluation of paraaortic lymph nodes discrimination between ganglions and lymph nodes showed to be important. Node-to-node analysis and follow-up of this study will give more accurate information on the value of USPIO-MRI for the detection of lymph node metastases in these patients.
Background
Adenocarcinoma’s of the pancreas and periampullary region (distal bile duct, ampulla of Vater and duodenum) are cancers with a poor survival1. Good preoperative TNM staging is important to determine the appropriate therapy and prognosis. An important negative prognostic factor is the presence of para-aortic lymph node (LN) metastases which are regarded as distant metastases and precluding a curative resection. Determining LN status, however, is challenging. Ferrotran, (SPL Medical) an ultra-small superparamagnetic iron oxide (USPIO) particle, has proven to be a valuable contrast agent for detecting LN metastases of solid tumours, like prostate and breast cancer, using magnetic resonance imaging (MRI)2-5. The aim of this study is to validate USPIO-MRI to pathology in patients with pancreatic or periampullary cancer.Method
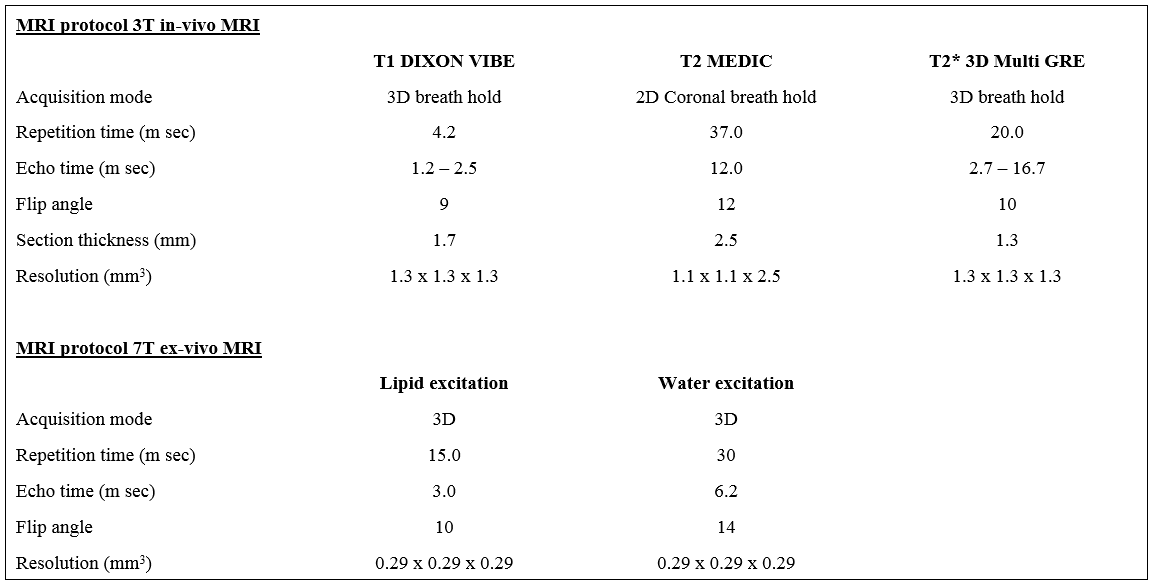
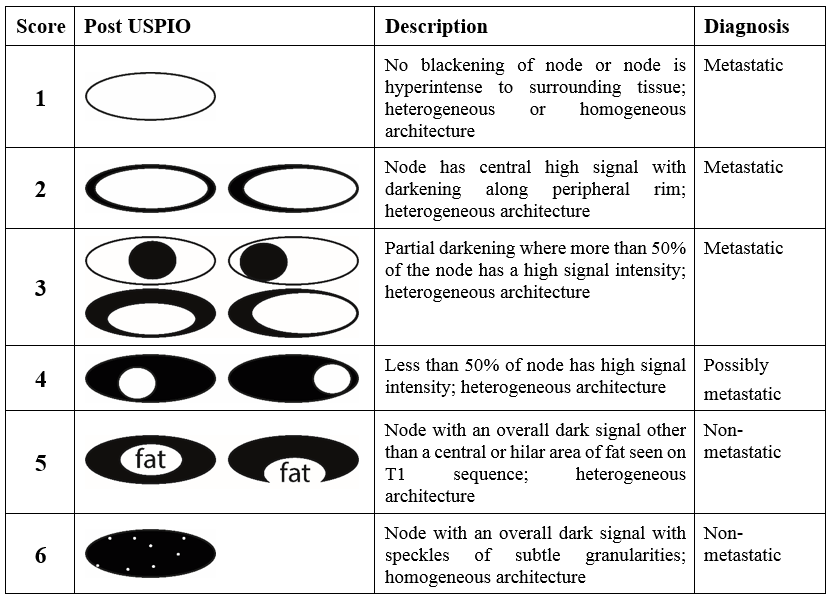
An interim analysis of a prospective ongoing single-centre feasibility study in patients (N=14) undergoing resection of pancreatic or periampullary adenocarcinoma. USPIO-nanoparticles (Ferrotran, 2.6mg Fe/kg body weight) are infused intravenously 24 to 36 hours prior to MRI (3T Magnetom PrismaFit, Siemens Healthcare). MRI protocols are summarized in figure 1. Before surgery the location of LNs on MRI is discussed with the surgeon. After resection, but before pathological examination an ex-vivo MRI of the fresh resection specimen is acquired on a 7T preclinical MRI scanner (Bruker Clinscan). Subsequently the specimen is routinely histopathologically examined. All MRI scans are evaluated by a radiologist blinded for the clinical outcome and results are discussed with a second, also blinded, radiologist. LNs are scored on T2-weighted 2D-Medic and T2star 3D-multigradient echo using a pre-defined 1-7 score proposed by Anzai et al6 (figure 2). LNs with scores 1-4 are considered suspect. LNs from histopathology are matched to LNs on USPIO-MRI using the ex-vivo MRI. Additionally, LNs are scored on the portal venous phase of routinely performed preoperative CT scan, based on expert opinion (combination of shape, size and internal structure). In this phase of the study the node-to-node analysis is not completed yet. In this first analysis all LNs are divided between regional and distant according to the tumour specific TNM classification7.Results
In all 14 patients USPIO-MRI was performed without any adverse events. One patient was excluded from analysis, due to unexpected perioperative peritoneal metastases. Of the 13 analysed patients, 6 patients had a cholangiocarcinoma, 3 a pancreatic, 3 an ampullary and 1 a duodenal adenocarcinoma.On MRI in total 307 LNs (78 regional; 229 distant) were detected, with a mean diameter of 5.3mm (range 2-22mm); 86 of these were suspect (28 regional; 58 distant). On CT in total 132 LNs (39 regional; 93 distant) were detected, with a mean diameter of 6.2mm (range 2-18mm); 57 of these were suspect (12 regional; 45 distant). In total 293 LNs were analysed histopathologically (260 regional; 33 distant); 38 of these were positive for malignancy (35 regional; 3 distant). The regional and distant lymph nodes (RLNs and DLNs) were separately assessed on a per-patient basis.
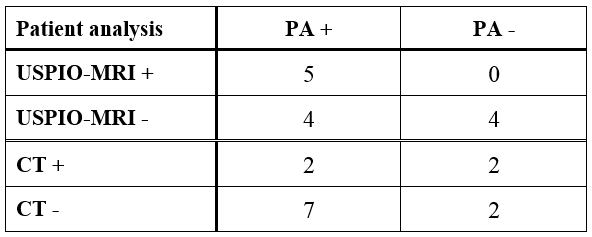
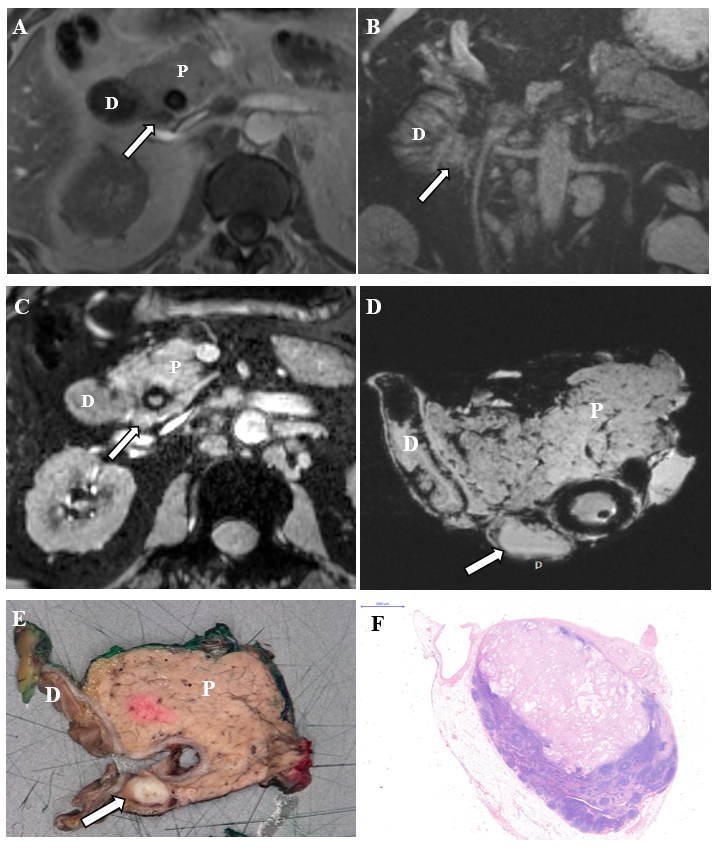
RLNs: on MRI, 5 patients had suspicious RLNs with positive RLNs histopathologically, 4 patients had negative RLNs on MRI, but positive RLNs histopathologically and 4 patients had negative RLNs on MRI with negative RLNs histopathologically. On CT, 2 patients had suspicious RLNs with positive RLNs histopathologically, 2 patients had suspicious RLNs on CT, but negative RLNs histopathologically, 7 patients had negative RLNs on CT but positive RLNs histopathologically and 2 patients had negative RLNs with negative RLNs histopathologically (figure 3). Figure 4 is an example of a positive RLNs in a patient on USPIO-MRI, ex-vivo MRI and histopathology.
DLN: In 6 patients DLNs suspicious on USPIO-MRI were resected: paraaortic in 5 patients and portacaval in 1 patient. In 1 patient (with paraaortic nodes) these LNs were positive on histopathology and in the other 5 patients LNs were negative.
Discussion
The preliminary data of this ongoing study show that it is feasible and safe to perform USPIO-MRI in patients with pancreatic or periampullary adenocarcinoma. USPIO-MRI shows twice as much LNs as CT. Remarkably, most detected LNs on USPIO-MRI and CT were distant. These are not routinely resected. Therefore, histopathological confirmation is usually not possible.All patients with suspect RLNs on MRI, had positive LNs histopathologically. The positive RLNs, not detected on MRI were mostly located close to the tumour and therefore probably difficult to detect on MRI. However, these LNs are of less clinical importance because they are routinely resected.
With regard to the distant LNs we retrospectively looked at the reason for suspect LNs on MRI with negative histopathology (N=5). The paraaortic LNs were probably ganglions misinterpreted for lymph nodes. This implies that USPIO-MRI in these patients has a learning curve with a need for more detailed knowledge of the anatomy of the lymphatic and ganglion system to distinguish suspicious LNs from ganglions. This is important to prevent unnecessary extended lymph node dissections and associated complications, like chylous leakage.
Conclusion
Performing USPIO-enhanced MRI in patients with pancreatic and periampullary adenocarcinoma is feasible and safe. The preliminary results show that on patient basis it is possible to detect regional and distant LN metastases with USPIO-MRI. Further analysis of the data, including a node-to-node analysis and follow-up, will provide more insight in the value of USPIO-MRI in these patients.Acknowledgements
This study is funded by the ‘Stichting UMC St. Radboud Radiologie’References
1: American Cancer Society. Cancer Facts & Figures 2018. Atlanta: American Cancer Society; 2018
2: Fortuin AS, Bruggemann R, van der Linden J, et al: Ultra-small superparamagnetic iron oxides for metastatic lymph node detection: back on the block. Wiley Interdiscip Rev Nanomed Nanobiotechnol 10, 2018
3: Harisinghani MG, Barentsz JO, Hahn PF, et al: Noninvasive Detection of Clinically Occult Lymph-Node Metastases in Prostate Cancer. The N Engl J Med; 348:2491-9, 2003
4: Heesakkers RAM, Hövels AM, Jager GJ et al: MRI with a lymph-node-specific contrast agent as an alternative to CT scan and lymph-node dissection in patients with prostate cancer: a prospective multicohort study. The Lancet. 2008
5: Go Nakai, Mitsuru Matsuki,Tomoaki Harada, et al: Evaluation of Axillary Lymph Nodes by Diffusion-Weighted MRI Using Ultrasmall Superparamagnetic Iron Oxide in Patients With Breast Cancer: Initial Clinical Experience. Journal of Magnetic Resonance Imaging; 34:557-562, 2011
6: Anzai Y, Piccoli CW, Outwater EK, et al: Evaluation of neck and body metastases to nodes with ferumoxtran 10-enhanced MR imaging: phase III safety and efficacy study. Radiology 228:777-88, 2003
7: International Union Against Cancer. TNM Classification of Malignant Tumours, Seventh Edition. 2010
Figures